
Abstract
Abstract
Background:
Pectus excavatum is an anomaly of chest wall development in which anterior ribs curve inward and the sternum is displaced toward the vertebral column. The Nuss procedure is a minimally invasive technique in which one or more metal bars are implanted to brace the sternum in a corrected position. Over time, the chest wall remodels into an anatomically corrected shape and the bar(s) are removed at a later date. During the procedure, passage of an introducer instrument and then the repair bar(s) may shear the intercostal muscles from the adjacent ribs. This creates larger than necessary defects in the chest wall, improper or unstable bar placement, and inadequate repair.
Instrument Design:
We report a new surgical instrument for guiding the introducer through the contralateral chest wall. This capture-guidance instrument (CGI) redirects and channels forces to keep the introducer true while preventing muscle stripping during passage of the introducer and repair bar(s).
Instrument Use:
The CGI has been piloted at two pectus centers with a notable decrease in intercostal muscle stripping.
Conclusion:
The CGI addresses the problem of shear and intercostal muscle stripping during traversal of the chest as part of Nuss repair of pectus excavatum.
Background
Pectus excavatum is an anomaly of chest wall development in which anterior ribs curve inward and the sternum is displaced toward the vertebral column 1 (Fig. 1). Loss of pulmonary domain and/or compression of the heart result in cardiopulmonary compromise.2–5 Pectus excavatum is the most common form of chest wall anomaly with a reported incidence of 1 per 400–1000 live births (male to female ratio, 4:1). Currently, the Nuss procedure is the most widely used repair for pectus excavatum. This minimally invasive technique uses one or more implanted metal bars to place and maintain the sternum in a corrected position. Over time, the chest wall remodels into an anatomically corrected shape. 6

Pectus excavatum.
During the Nuss procedure an introducer instrument is passed between the anterior ribs on one side (generally the right), under the sternum, and then between the ribs and out through the chest wall on the contralateral side (Fig. 2). The introducer is then replaced with a custom-bent repair bar that further elevates the sternum into position.
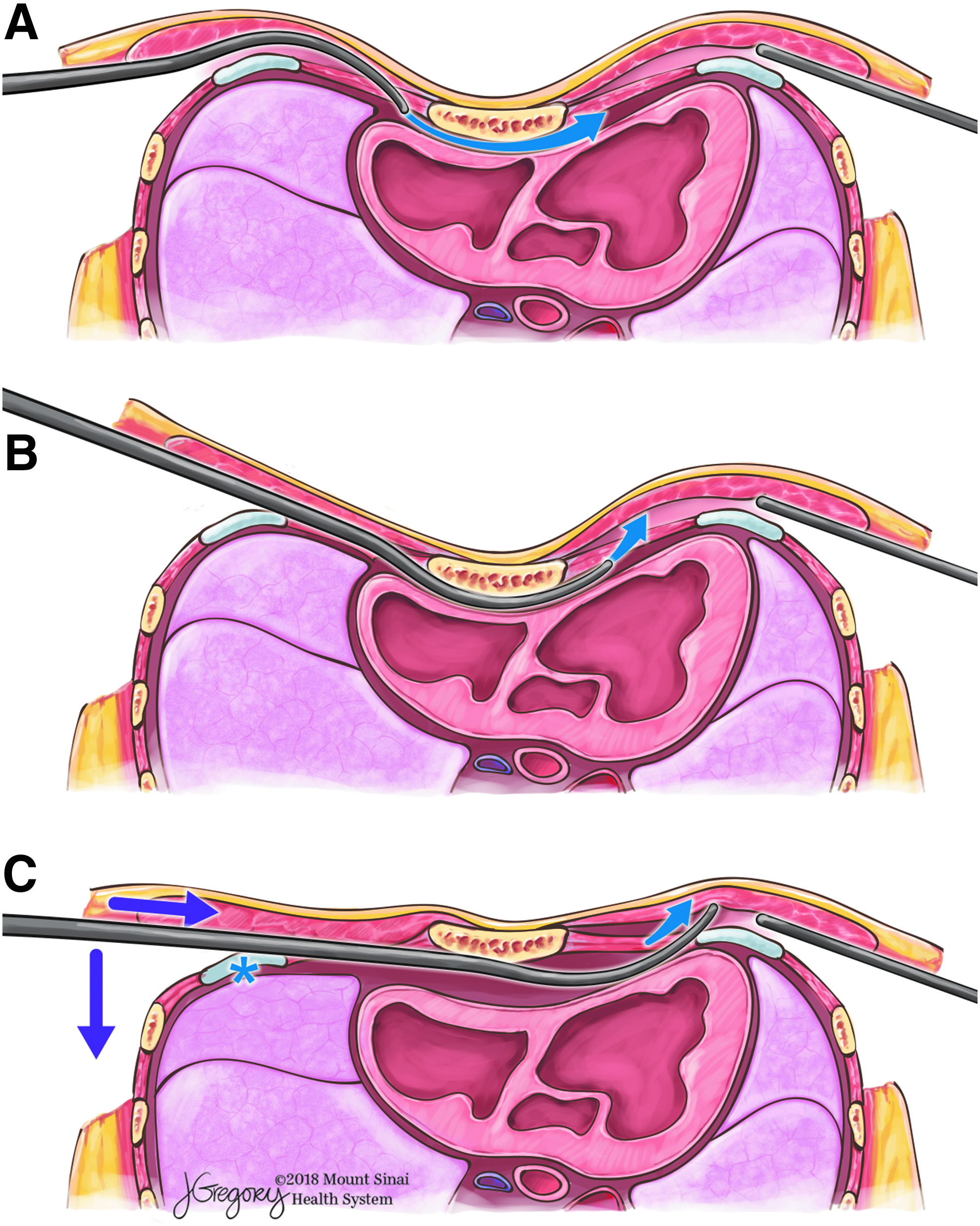
Introducer insertion.
Two issues are routinely encountered when passing the introducer. First, depending on the size of the introducer, the depth of the sternal depression and the rigidity of the sternum, exiting the contralateral chest wall using leverage may be difficult (Fig. 2). Second, and most notably, as the introducer exits the chest, the introducer may shear the intercostal muscles off the contralateral rib. This intercostal muscle stripping creates a larger than necessary defect in the chest wall, improper or unstable bar placement, and inadequate sternal lift. The intercostal muscle stripping occurs because the ribs, being oblique, allow the introducer to slide inferiorly along the intercostal space in response to transversely directed (across the chest) force. Obtaining leverage to bring the introducer out of the contralateral chest wall can also cause stripping of the intercostal muscles on the ipsilateral side (Figs. 2 and 3).

Intercostal shear and muscle stripping. Because the medial inferior ribs are oblique downward from the sternum, the leverage and transverse force used to pass the introducer (Fig. 2) may cause the introducer to shear along the ribs, stripping the intercostal musculature and mispositioning the bar. ©Mount Sinai Health System, used with permission.
Loss of integrity of the intercostal musculature during these maneuvers may predispose to additional muscle stripping when rotating the bar into position and postoperatively. 7 Muscle stripping allows the bar to settle in a more posterior (lower pressure) position. This movement within the intercostal space decreases the effectiveness of the outward (anterior) force on the sternum and undermines the repair. The risk of muscle stripping is increased with more severe sternal depression and increased chest wall rigidity. 8 Stripping and bar migration is sufficiently problematic to have fostered numerous methods to secure the bar.9–12
Instrument Design
A new surgical instrument for guiding the introducer and repair bar(s) through the chest wall was designed by the lead author (L.B.) and fabricated by Zimmer Biomet (catalog #SP-3088) as part of their Rapid Response Program (Fig. 4). The instrument features an oblique tongue, which is pressed through the intercostal musculature and engages the introducer as it traverses the chest. Because the tongue acts as an inclined plane, transverse force is translated outward and aids in exiting the introducer through the chest wall (Fig. 5). This lessens the need for leverage to exit the introducer and instead relies only on transverse force pushing across the chest. By minimizing the need for leverage, the device decreases the risk of shear and muscle stripping along the ipsilateral rib. Once the introducer tip exits the chest wall, the instrument's channel keeps the introducer in-line without slippage along the contralateral rib. This protects the integrity of the contralateral intercostal muscles. Similarly, the instrument is effective during the exchange of the introducer for the repair bar to prevent stripping from passage of the bar itself.

CGI. The CGI consists of (1) a tongue that is used to engage the introducer in the intercostal space, (2) a channel that guides the introducer (and later bar) in a straight manner, and (3) a handle. CGI, capture-guidance instrument.
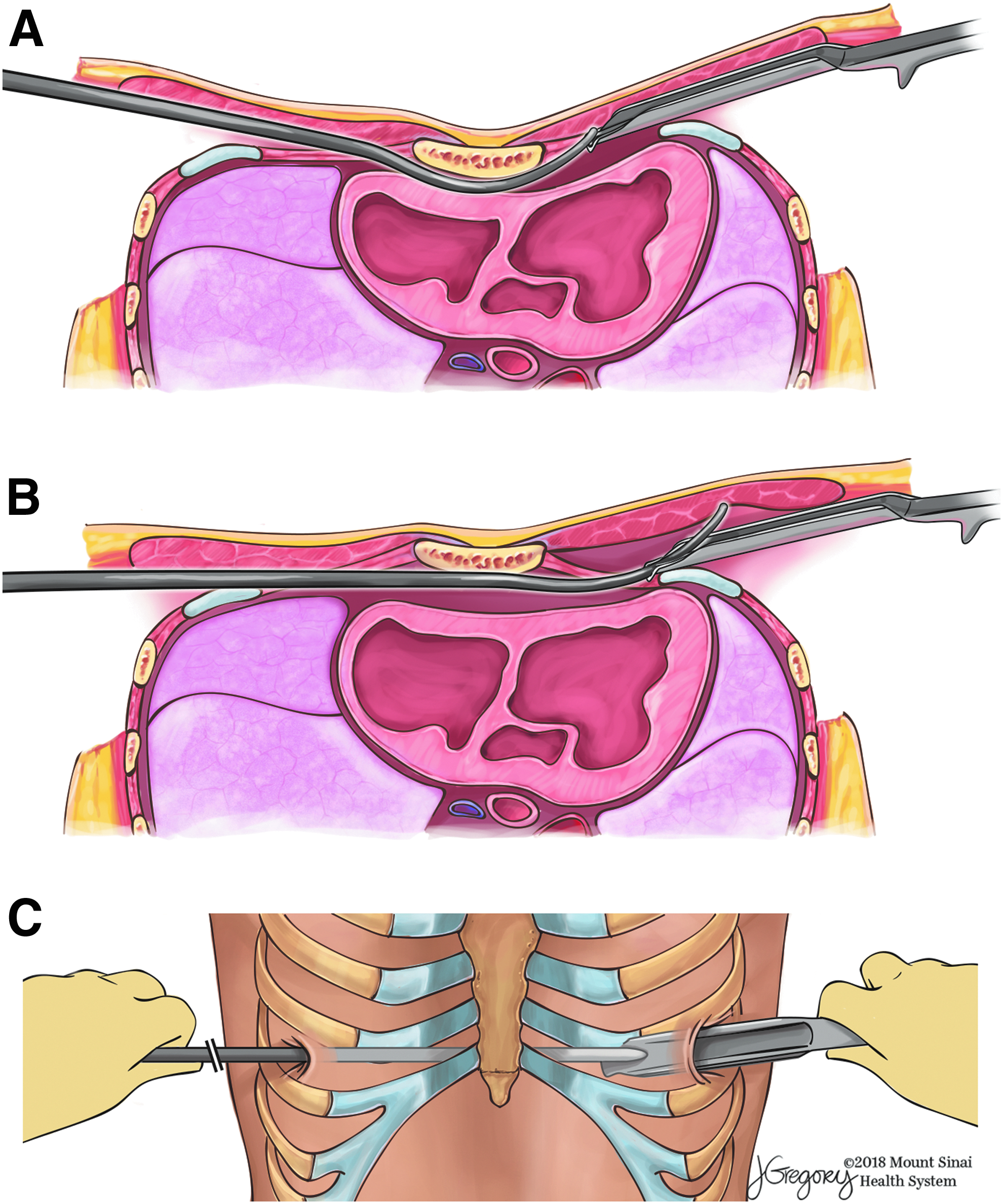
Use of the CGI.
Instrument Use
Five surgeons at two centers have piloted use the capture-guidance instrument (CGI). The mean age of the population for the first 103 patients was 15.6 ± 2.4 years, male to female ratio 4:1, and number of bars 1.7 ± 0.5. In this experience, the CGI prevented shear and stripping of the intercostal muscles during passage of the introducer and pectus bar. The introducer and bar exit the chest wall surrounded by intact intercostal muscles, which decreases the risk of posterior bar displacement (Fig. 6). Before use of the CGI, stripping of the intercostal muscles in children with rigid sternums created a defect of several centimeters in length and made it difficult to maintain the bar in an effective position. If multiple bars were required, one or more ribs may have been stripped completely within the operative field. The CGI was easy to use and did not lengthen the procedure (Supplementary Video 1). It was not associated with any adverse events. We use external elevation of the sternum either selectively (Center 1) or routinely (Center 2), which also helps prevent stripping. Additional methods to secure the bar and prevent postoperative slippage (referenced earlier) are used as well.
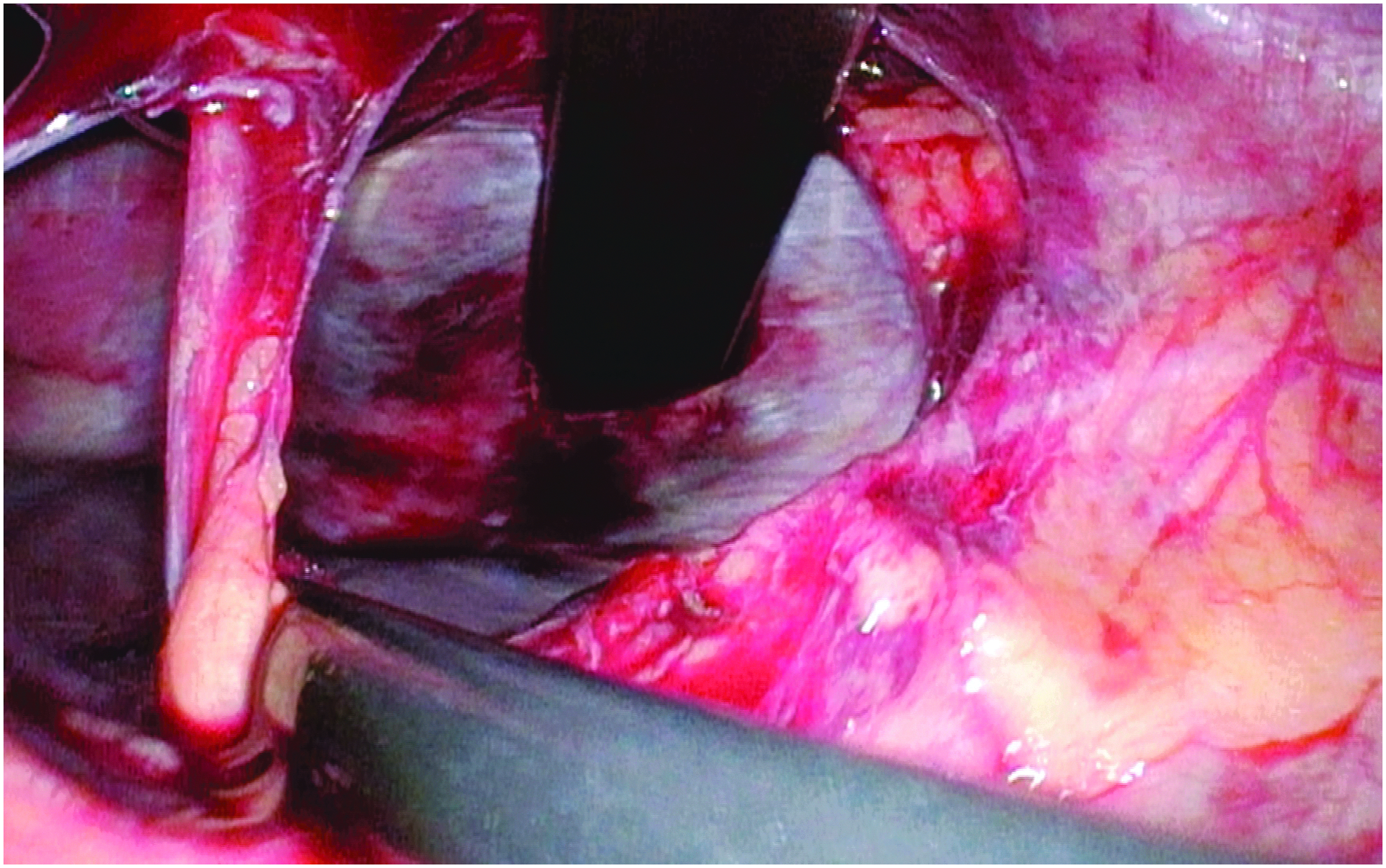
Repair bar in position. As viewed across the mediastinum from the right chest, the repair bar is seen to exit the left chest wall tightly surrounded by the intercostal muscles. Muscle stripping is absent despite sequential chest wall traversal by the introducer and then the bar.
Technical Notes
Once the exit site is identified, the CGI is introduced into the contralateral interspace. Care is taken to control entry to allow only the tongue to enter the chest. The CGI is held in position, and not forced into the chest beyond the tongue, especially while the introducer is being pushed from the other side. The introducer is passed across the chest, engages the tongue of the CGI, and is guided out the interspace a short distance. Sternal elevation may be used to assist in traversal of the chest. 8 The skin and pectoralis muscles are lifted over the introducer, and the introducer is then pushed across the chest while the CGI guides the introducer and protects the intercostal space. Umbilical tape, FiberWire®, or sterile tubing is attached to the introducer and the introducer is withdrawn with the CGI still in place. The Nuss bar is then guided into place along the path created by the introducer, again using the CGI to protect the interspace. The CGI is withdrawn before rotating the bar into final position.
Conclusion
The CGI addresses the problem of intercostal muscle stripping during passage of the introducer and Nuss bar during repair of pectus excavatum. The benefits of reduction in intercostal stripping include avoiding partial loss of correction due to shifting within the intercostal space and decreased freedom of movement of the bar. The described instrument is easily adopted by surgeons familiar with the Nuss procedure and does not negatively impact procedure cost or time.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.