
Abstract
Abstract
Introduction:
Creation of pneumoperitoneum and laparoscopic entry into the abdominal cavity are crucial initial steps of laparoscopic surgery and associated with bowel and major vessel injuries. Various methods have been described in literature such as Veress needle, open access technique (OAT), direct trocar insertion (DTI), and optical port. There is no consensus on the safest method of gaining access to the peritoneal cavity to create a pneumoperitoneum. DTI technique appears to be not well accepted by many due to the fear of causing injuries as it is a blind procedure.
Objective:
To compare the outcome of DTI in terms of feasibility and complications with a well-established and widely practiced OAT for a laparoscopic procedure.
Materials and Methods:
Nine hundred fifty-five participants were randomized to be in either of the two groups, that is, Group “A” for DTI and Group “B” for OAT. The primary endpoint was major complications (bowel, major vessel, and solid organ injury) and the secondary endpoint was port access time and minor complications directly related to access. Patients were assessed on the first postoperative day, at the time of discharge, 3 months, 6 months, and a year after discharge, for complications.
Results:
There was no statistical difference in major complications between DTI and OAT groups, however, DTI was found to be superior to OAT in terms of port access time (P = .01), umbilical port-site hernia, port-site infection, and port-site pain (P = .01).
Conclusion:
This study further strengthens the literature on DTI being a good and safe technique of laparoscopic access. The technique of DTI is still underutilized and needs to be adopted by surgeons without fear.
Introduction
Establishing an acceptable pneumoperitoneum is the first and most important stage of laparoscopy. Initially, laparoscopic surgery was termed as minimally invasive surgery, but this term was changed to minimal access surgery as laparoscopic surgery is an invasive procedure associated with similar risks of major complications, as open surgery. The major difference between laparoscopic surgery and open surgery is the access. Access is associated with injuries to gastrointestinal tract and major blood vessels and at least 50% of these major complications occur before commencement of intended surgery.1–5 This complication rate has remained the same during the last 25 years. 6 The majority of injuries are due to insertion of the primary umbilical trocar. 7
To minimize entry-related injuries, several techniques, instruments, and approaches have been introduced. Of the several, the four basic techniques most commonly used are (i) blind Veress needle (VN 8 ), (ii) direct trocar insertion (DTI), 9 (iii) optical trocar insertion, 10 and (iv) open access (Hasson technique). 11
DTI appears to be a technique that has not been well accepted by many of the practicing surgeons and gynecologists due to fear of causing injury to the abdominal structures as it is a blind procedure. 12 The aim of this study was to compare the outcome of DTI with a well-established and widely practiced open access technique (OAT).
Materials and Methods
This study was a prospective randomized controlled trial conducted at the department of surgical gastroenterology of a tertiary care center between July 2012 and July 2017. Participants were randomized to be in either of the two groups, that is, Group “A” for DTI and Group “B” for open entry using a central randomization system with a simple convenient sampling method. Sample size was calculated for a noninferiority randomized trial. Based on the existing literature where complications in both arms were around 0.1% and assuming a noninferiority margin of 0.5%, with a study power of 80% and a confidence interval of 95%, the calculated sample size was 950 patients with 475 patients in each arm.
All those patients younger than 10 years, pregnant females, emergency surgeries, patients with previous midline abdominal surgery, respiratory compromise, uncorrected coagulopathy, or peritonitis were excluded from the study. Written informed consent was taken from all the study participants. Permission from the institutional ethics committee was obtained before starting the study. The trial was registered with the clinical trial registry (CTRI/2018/01/011128).
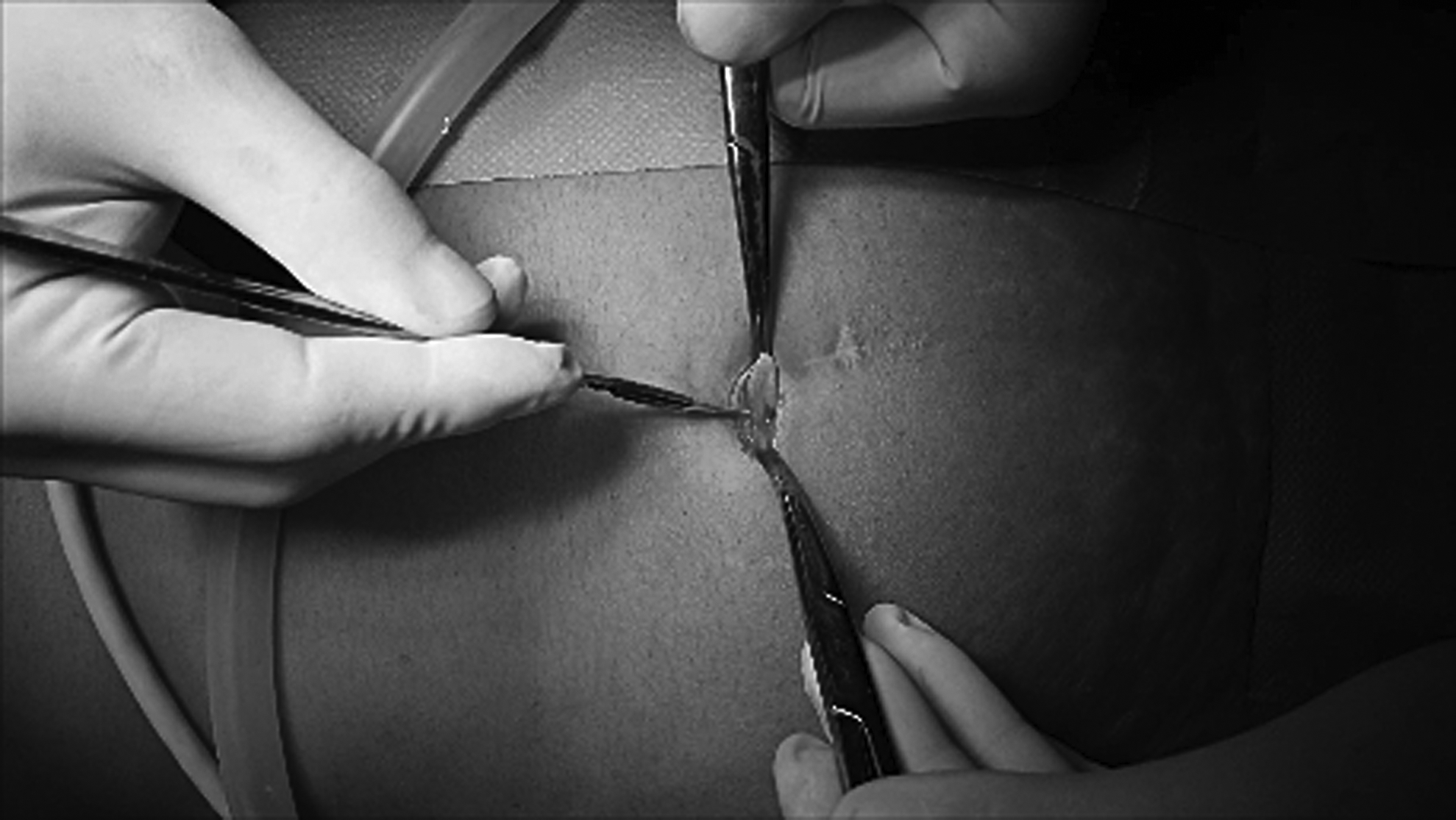
The operating surgeons, all surgical gastroenterologists well-versed in both the access techniques, entered the peritoneal cavity with the technique allotted by randomization. The technique adopted for DTI is as follows (See Supplementary Video S1, “DTI”). First, a vertical 10 mm skin incision through the umbilicus was made followed by holding and elevating the dry anterior abdominal wall of left lower quadrant by the nondominant (left) hand. Thereafter, a 10 mm sharp metal trocar/cannula was held in the dominant (right) hand with the base of the trocar resting at the junction of thenar and hypothenar eminence, and the index finger used as a guard against sudden uncontrolled penetration into the peritoneal cavity by placing it over the cannula, 4 cm short of the trocar tip (Fig. 1). With the dominant hand holding the trocar and aiming toward the side of elevation, twisting semicircular motion was continued till a “give” was felt. At this time the trocar was withdrawn, and cannula was further inserted by 2–3 cm. Entry into the peritoneum was confirmed by putting the scope into the cannula followed by insufflation.

Showing DTI technique by using the nondominant hand to lift the abdominal wall while inserting the trocar with the dominant hand and using index finger as a guard. DTI, direct trocar insertion.
The OAT adopted was a variation from the Hasson technique. 13 In this technique, a 1–1.5 cm skin incision was taken at the umbilicus. Dissection was continued down to the fascia while the skin was held retracted (Fig. 2). Thereafter, the fascia was incised, and the peritoneal cavity entered by the cannula over a blunt obturator. In both methods, fascia was not closed following removal of umbilical port.
Showing the skin retraction with incision on the fascia in OAT. OAT, open access technique.
The outcomes were analyzed on an intention-to-treat basis. The primary endpoint of the study was major complications (blood vessel, bowel, or solid organ injury having the potential of causing Clavien–Dindo complication of grade 3 and above). The secondary endpoint was minor complications (Clavien–Dindo complication of grade 1 or 2 such as umbilical port-site infection and bleed, subcutaneous emphysema, umbilical port-site pain, entry reattempted, and gas leakage from the umbilical port necessitating “U” stitch with a 1/0 Prolene to tighten the port site to seal the leak) and mean port access time. Port access time was defined as the time interval between skin incision and introduction of the laparoscope for confirmation of access.
Patients were assessed on the first postoperative day, at the time of discharge, 3 months, 6 months, and a year after discharge, for complications. Those patients who could not come for review were telephonically interviewed for complications.
Continuous data presented as mean ± standard deviation and categorical data as numbers and percentages. Categorical variables were compared using chi-square test or Fisher's exact test, whichever applicable. Continuous variables were compared using Mann–Whitney U-test. A P-value of <.05 was considered statistically significant.
Results
A total 955 study participants were enrolled in the study. Group “A” had 484 patients who were randomized to DTI, while Group “B” had 471 patients who were randomized to OAT (Fig. 3).

Consort diagram.
Of the 955 patients, 260 were males and 695 were females. Age ranged from 22 to 60 years with a mean age of 42.8 ± 18.6 years in Group A and 45.2 ± 21.1 months in Group B (Table 1).
Demographic Distribution of Study Population
BMI, body mass index.
The bulk of the laparoscopic surgeries done were cholecystectomies (71.20%) and appendectomies (10.2%) (Table 2).
Type of Surgeries Conducted Using Direct Trocar Insertion and Open Access Technique
LAR/APR, low anterior resection/abdominoperineal resection; TAPP, trans abdominal preperitoneal repair.
Major complications were not significantly different between the two groups (Table 3). Two bowel injuries occurred in OAT group while doing laparoscopic cholecystectomy. Both occurred when, while opening the fascia that was held up by artery forceps, the ileum was accidentally entered. Fortunately, these were detected intraoperatively and one of them required conversion to open surgery. No vascular or solid organ injuries occurred in either group. Minor complications were significantly more in OAT group. More than one attempt required to gain access into the abdomen was more in the DTI arm. Significant gas leakage from umbilical port occurred in 39 patients in OAT arm and 4 in DTI arm, respectively. Time taken from incision at umbilicus to introduction of laparoscope was three times higher in OAT arm (Table 3).
Complications Encountered During Surgery and Postoperative Follow-Up Period
Only 471 and 462 patients completed the 1-year follow-up.
Discussion
Over the last decade, rapid advances have been made in laparoscopic surgery. Although it is a well-established procedure, it still generates controversy, particularly with regard to the best method for creation of the pneumoperitoneum. Abdominal access and creation of the pneumoperitoneum carry a risk of bowel and vascular injury.12,14 Bowel injuries occur in 0.7/1000 and major vascular injuries in 0.4/1000. The overall incidence of major injuries at the time of entry is 1.1/1000. 15 It has been said that it is very much possible that these injuries are underreported. 15
The DTI technique was first reported by Dingfelder in 1978. 9 Forty years have elapsed since then, but it still remains the least-utilized technique owing to the fear of causing increased bowel or vessel injuries. As such, the probability of bowel being stuck to the umbilicus in a virgin abdomen is only 0.03%. 16
There are several retrospective studies published on the safety of this method of entry16–24 (Table 4). Although a few studies were prospective, only four were randomized25–28 (Table 5). There are only three level I evidence studies15,29,30 (Table 6). A study by Jacobson et al., 17 involving 1223 patients who had undergone DTI and 22 patients who had undergone OAT for laparoscopic access, showed only one bowel injury in OAT group and none in DTI group. In the study by Falahatkar et al., 21 only one vascular injury occurred in OAT group (n = 86) and none in DTI group (n = 62) (Table 4). Angioli et al. 28 showed no major injury in DTI (n = 187) and OAT (n = 215) groups (Table 5). A meta-analysis conducted by Molloy et al. 15 showed that OAT is statistically more likely to be associated with bowel injury than DTI (10/21,547 and 3/16,739 patients). However, vascular injury rates were almost nil in both groups (1/21,547 and 0/16,739 patients) (Table 6). In line with these studies, our study showed no major complications in the DTI arm, whereas two bowel injuries occurred in the OAT arm, although this was statistically not significant. Minor complications were also significantly lesser in the DTI arm. The DTI arm fared significantly better in terms of umbilical port-site infection (n = 0.01), pain (n = 0.01), and hernia (n = 0.01), respectively (Table 3). The DTI arm was also significantly superior in terms of gas leak and showed a trend toward significance in terms of subcutaneous emphysema (Table 3). Studies have shown that DTI has a significantly shorter access time when compared with OAT 28 and VN24,26–28 (Table 5). Likewise, our study showed mean access time of 80.2 seconds for DTI group versus 180.9 seconds for OAT group (P = .01). The Society of Obstetricians and Gynaecologists of Canada Clinical Practice Guidelines recommended that DTI is not only a safe alternative to VN but is also faster and associated with less complications. 31
Retrospective Studies (Level III Evidence)
DTI, direct trocar insertion; OAT, open access technique; VN, Veress needle.
Prospective Randomized Controlled Trial (Level II Evidence)
DTI, direct trocar insertion; OAT, open access technique; VN, Veress needle.
Systematic Review and Meta-Analysis (Level I Evidence)
DTI, direct trocar insertion; OAT, open access technique; VN, Veress needle.
Although several studies in literature have shown superiority of DTI over the VN technique,15,17,22,24–28,30 only a few studies exist in literature where DTI has been compared with OAT,15,17,21,28 showing that DTI is not only faster but also shows trend toward lesser complications.
Conclusion
This study further strengthens the literature on DTI being a faster, safer, and a good technique of laparoscopic access. The technique of DTI is still underutilized and needs to be adopted by surgeons without fear.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.