
Abstract
Abstract
Purpose:
The purpose of this report was to evaluate the safety and efficacy of the simple laparoscopic percutaneous extraperitoneal closure (LPEC) method for treating ovarian hernia patients, including newborns and low-birth-weight infants.
Methods:
We retrospectively reviewed the cases of ovarian hernia that were treated in our institution from May 2012 to September 2017.
Results:
Thirty-four infants were included in this study (right side, n = 8; left side, n = 22; bilateral, n = 4). The mean corrected age was 2.3 ± 2.8 months and the mean body weight was 4.4 ± 1.6 kg. The contralateral positive rate was 53%, and 34% of the cases showed sliding of the fallopian tube. Umbilical hernias were observed in 24 cases (71%). The mean operative time was 53 ± 20 minutes. The LPEC procedure was successful in 32 cases; two cases were converted to open surgery.
Conclusion:
Small infants with ovarian hernia have some specific features such as a shortened round ligament and the presence of peritoneum cavities that require skillful techniques when being surgically repaired. The simple LPEC procedure can be performed safely with a low risk of recurrence, even in infants with sliding of the fallopian tube.
Introduction
T
In our institution, most ovarian hernia cases are treated by LPEC. In addition to outpatients, very–low-birth-weight infants (VLBWI) and extremely low-birth-weight infants (ELBWI) with ovarian hernia also undergo hernia repair before discharge. The purpose of this report was to evaluate the safety and efficacy of LPEC for female infants with ovarian hernia.
Materials and Methods
We retrospectively reviewed the cases of ovarian hernia that were treated in our institution from May 2012 to September 2017. The corrected age and body weight at surgery, operative time, the presence or absence of sliding of the fallopian tube, the existence of contralateral hernia, additional port insertion, conversion, complications, recurrence, and associated malformations such as umbilical hernia were extracted from the patients' medical records.
Ovarian hernia
Ovarian hernia was defined as the ovary herniation to the inguinal hernia sac that was diagnosed based on the preoperative ultrasonography or intraoperative laparoscopic findings.
Sliding hernia
Gaspar et al. 6 defined sliding hernia as “Sliding hernias are those in which part of the wall of the sac is formed by a viscus.” Cases of ovarian hernia in which the ovary can easily be reduced are not included in the definition of “ovarian sliding hernia.” In this study, a sliding hernia was defined as a hernia in which the fallopian tube formed part of the wall of the sac and prolapsed over the internal hernia ring, even after the reduction of ovary (Fig. 1).
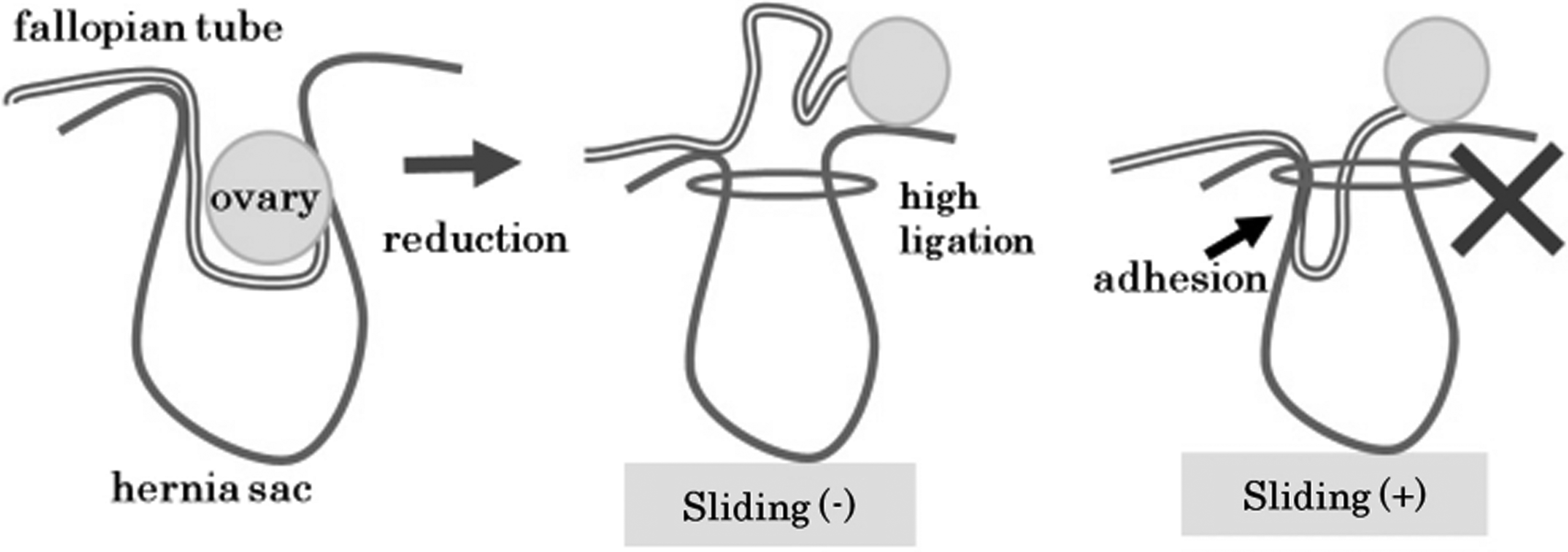
Sliding hernia. In a sliding hernia, the fallopian tube forms part of the sac and prolapses over the internal hernia ring even after reduction of the ovary.
LPEC procedure
A 5 mm laparoscope was inserted through umbilical incision. In patients with umbilical hernia, a subumbilical incision was made and umbilical plasty was performed after LPEC. A mid-umbilical incision was made in patients without umbilical hernia. A 2.7 mm grasping forceps was inserted through the right lateral abdomen. A herniated ovary will be reduced during operation by retracting the round ligament with compression from the inguinal surface. A 19-gauge LPEC needle holding a 2-0 nonabsorbable thread was inserted from the skin just above the internal inguinal ring. The thread was passed through by inserting the tip of the needle hemicircumferentially into the extraperitoneal cavity. First, internal side dissection was performed. The peritoneum was punctured and the thread was left inside the abdominal cavity. Second, after dissecting the external side, the thread was collected; this enables circumferential ligation.
The features of ovarian hernia in small infants are specific. In comparison with older patients, the peritoneum is edematous and the remarkably short round ligament is accompanied by peritoneum cavities on both sides (Fig. 2a, b). The round ligament is retracted strongly to the cranial side with forceps, and caution must be exercised when the LPEC needle is used in the extraperitoneal cavity to avoid puncturing or damaging the peritoneum. In case of a sliding hernia, the tip of the LPEC needle should be inserted distal to the fallopian tube to avoid ligating the tube (Fig. 3a, b). After the procedure, the thread should be tied five times extracorporeally. The round ligament should be pulled to confirm that the hernial ring is tightly closed (Fig. 3c).

Left inguinal hernia.

LPEC for sliding hernia.
Results
Thirty-four infants were included in this study (right side, n = 8; left side, n = 22; bilateral, n = 4) (Table 1). The mean corrected age was 2.3 ± 2.8 (0–11) months and the mean body weight was 4.4 ± 1.6 (2.39–8.65) kg. Sixteen of 30 unilateral ovarian hernia patients were contralateral positive; in these cases, the contralateral hernias were closed intraoperatively. Thirteen patients had sliding hernias (34%). Umbilical hernias coexisted in 24 cases (71%). Eight patients were ELBWIs and 2 were VLBWIs. The mean operative time was 53 ± 20 (31–123) minutes (sliding hernia positive, 59 ± 26 minutes; sliding hernia negative, 50 ± 13 minutes; umbilical hernia positive 61 ± 20 minutes; umbilical hernia negative 40 ± 8 minutes).
In one case, the ovary was irreducible because of adhesion to the hernia sac. In the other case, we found it difficult to treat a 2.39 kg infant with marked sliding of the fallopian tube by LPEC because of a very small abdominal cavity.
LPEC, laparoscopic percutaneous extraperitoneal closure.
Laparoscopic procedures were successful in 32 cases; two cases were converted to open surgery. In one case the bilateral ovaries were herniated. Despite the insertion of an additional port the right ovary was irreducible; in contrast, the left ovary was reduced with ease. The conversion of right side ovarian hernia was determined when the ovary was irreducible, at ∼15 minutes after the start of the operation. At the time of conversion, we found that the right ovary was strongly adhered to the hernia sac, such that it formed a partial wall of the hernia sac (the strict definition would be ovarian sliding hernia). One hundred twenty-three minutes were spent in total. The laparoscopic approach was ultimately unsuccessful in this case. The second case, involved a left-side ovarian hernia in an infant weighing 2.39 kg; marked sliding of fallopian tube was observed and the abdominal cavity was considered to be too small. We decided to convert to open surgery without attempting LPEC. The contralateral side was negative and the operative time was 52 minutes.
Recurrence was observed in a single case at 15 months after original sliding hernia repair with LPEC. Intestinal hernia was confirmed and 2-0 nonabsorbable thread was torn off beside the internal inguinal ring that was thought as a reason of the recurrence. Sliding was no longer observed. LPEC was performed again and the postoperative course was uneventful. The mean postoperative follow-up period was 8.8 (0–48) months.
Discussion
Laparoscopic surgery including LPEC is very useful and is recommended for ovarian hernia repair in girls because it allows for the identification of the genital organs (especially the ovaries and fallopian tubes) and allows the operator to investigate whether contralateral hernia is present. 4 Ovarian hernia often occurs in infants with a small abdominal cavity and practice is required to attain the skills to perform laparoscopic surgery in such cases. Furthermore, sliding of the fallopian tube is observed in ∼1 in 3 patients, and certain techniques are involved in treating such cases by LPEC. This is the first report describing the details of LPEC procedure against sliding positive ovarian hernia.
In this study, the use of LPEC achieved good results in the treatment of infant ovarian hernia. Only one recurrent case was observed among 34 patients (2.9%). In this case, the 2-0 nonabsorbable thread was torn off beside the internal inguinal ring; this was thought to be a reason for the recurrence. This was one of the early cases. At the time of first LPEC procedure, the thread was possibly damaged by the LPEC needle. After that case, the LPEC procedures were carefully performed to avoid damaging the threads. None of the subsequent cases developed recurrent hernia. There were no cases of recurrence because of the low ligation of the hernia sac.
Conversion to open surgery was required in two cases. The LPEC cannot be applied in patients with an irreducible ovary. In one case the ovary had strongly adhered to the hernia sac and formed a wall. Such cases should truly be termed ‘sliding hernia of the ovary,’ which is a contraindication for LPEC.
There are two points that should be considered in the operative procedure.
The markedly short round ligament is accompanied by peritoneum cavities on both sides. Surgeons should be careful with this specific structure and must retract the round ligament to the cranial side when passing the LPEC needle into the extraperitoneal cavity.
In case sliding is detected, the thread must be passed through just beside the fallopian tube to avoid the low ligation of the hernia sac. If it is difficult, operators should not hesitate in inserting an additional port to secure the procedure.
If operators pay attention to these points, then simple LPEC for ovarian hernia can be performed safely even in infants with sliding of the fallopian tube.
The mean operative time was 53 ± 20 (31–123) minutes, which was similar to another report. 7 Among the sliding-positive patients (n = 13, including eight umbilical hernia-positive patients), the mean operative time was 59 ± 26 minutes. Ishii et al. 5 reported that they experienced recurrence when simple LPEC was first applied in a sliding-positive case and recommended LPEC plus an additional procedure or conversion that required a longer operative time. In contrast, this study indicated that simple LPEC can be performed safely and effectively with approximately the same operative time. Even in infants with sliding hernia, the simple LPEC is also recommended.
The umbilical hernias were found to coexist in 24 cases (71%). Umbilical hernia often coexisted with inguinal hernia in infants and can be repaired simultaneously. The surgical closure of umbilical hernia in infancy is easy and results in a good cosmetic outcome. 8
This study is associated with some limitations, including its retrospective nature. Furthermore, the relatively small study population prevented us from statistically analyzing the factors associated with recurrence. A prospective study of a larger study population should be performed to evaluate the safety and the efficacy of LPEC for ovarian hernia in patients with sliding of the fallopian tube.
Ethical Approval
Formal consent was not required for this study.
Footnotes
Acknowledgment
The authors also thank Brian Quinn for reviewing the article.
Disclosure Statement
No competing financial interests exist.