
Abstract
Abstract
Background:
Laparoscopic surgery causes less pain than traditional surgery; however, to relieve postoperative pain, surgeons frequently apply local anesthetic preemptively. The aim of this study was to assess the effect of different local anesthetics on pain intensity in patients who had undergone a laparoscopic appendectomy (LA), who received the anesthetic preemptively at incision sites and postemptively, intraperitoneally and trocar sites.
Patients and Methods:
A total of 120 LA patients (men and women) were randomly assigned to 1 of the 4 groups (N = 30/group): Group 1: no peritoneal or local administration of local anesthetics during LA; Group 2: 5 mL of 1% lidocaine was applied at incision sites and 10 mL 1% lidocaine was injected under direct vision in the right iliac fossa area and around the stump of the appendix and trocar sites at the end of the procedure; Group 3: 5 mL of 0.5% levobupivacaine applied at incision sites +10 mL 0.5% levobupivacaine injected in the same place intraperitoneally and trocar sites at the end of the procedure; Group 4: 5 mL of 0.5% ropivacaine at incision sites +10 mL 0.5% ropivacaine injected in the same place intraperitoneally and trocar sites at the end of the procedure. Postoperative pain was assessed after 2, 6, 24, and 48 hours using a visual analogue scale (VAS).
Results:
By comparing the average values of pain intensity using VAS, we observed significantly different average values of pain intensity in the levobupivacaine and ropivacaine (3 and 4) groups in comparison with the control Group 1 (P < .05) throughout the follow-up period.
Conclusion:
We observed a reduction in postoperative pain, nausea, and vomiting in patients with LA who received intraoperative local anesthetic preemptively at the incision sites and postemptively, intraperitoneally. After the application of levobupivacaine the intensity of pain was significantly lower than in any other tested group.
Introduction
P
Use of local anesthetics in laparoscopic surgery is most commonly applied for laparoscopic cholecystectomy, where different methods of local anesthetic application are used. 5 Usually, local anesthetics, such as lidocaine, bupivacaine, ropivacaine, and levobupivacaine, are used. It has still not been definitely decided whether local anesthetics should be used before or after the surgical procedure. In studies where intraperitoneal local anesthesia was used, a method was usually used where local anesthetics were inserted under the diaphragm and on the site of the operating field. 6
Appendectomy is the most common surgical procedure performed in abdominal surgery. Postoperatively, there is pain that is usually treated by systemic analgesics (nonsteroidal anti-inflammatory drugs and opiates). Considering the fact that local anesthetics reduce the pain after a laparoscopic cholecystectomy, it is to be expected that a similar effect may be achieved in laparoscopic appendectomy (LA). Moreover, there is notable positive effect seen in a decrease in the frequency of postoperative nausea and vomiting (PONV).7–9 So far, studies have been undertaken where a local anesthetic is applied preemptively at the site of the trocar incision. 1 However, we do not know the effect of different local anesthetic in patients who have undergone LA, and in whom the anesthetic is applied preemptively at the sites of the trocar incision and postemptively, intraperitoneally.
Patients and Methods
This was a prospective, clinical, randomized single-blind study that included patients who had undergone surgery, and upon whom LA was performed. The surgery was performed after the ethics committee approval, approved by the General Hospital “Abdulah Nakas,” Sarajevo, and written informed consents were obtained from all the patients.
Inclusion criteria
Patients with indications for LA towing to appendicitis, 18–70 years old, who where classified as American Society of Anesthesiologists (ASA) physical status ASA I or ASA II were included. The operation was performed by a surgeon who had performed 10 or more laparoscopic appendectomies.
Exclusion criteria
Pregnancy; previous surgery in the pelvic area or lower abdomen; local anesthetic allergies; other abdominal conditions that may cause intra-abdominal pain, such as endometriosis, enteritis, adnexitis, and so on; patients where conversion to open appendectomy was undertaken; patients with perforation of the appendix and peritonitis; and patients where normal communication was impaired because of the lack of adequate verbal contact were excluded.
Randomization, allocation concealment, and masking
If the patient satisfied the inclusion criteria for the study, patient randomization was initiated by extracting a note from a closed opaque envelope containing the title of one of the four test groups. After randomization, LA was performed.
Intervention
A total of 120 patients of both genders were included in the study. The 120 patients were randomly assigned to 1 of the 4 groups of 30 patients each:
Group 1: no peritoneal administration or local administration of local anesthetics during the LA; Group 2: 5 mL of 1% lidocaine was applied at the three trocar insertion sites and 10 mL 1% lidocaine was injected under direct vision in the right iliac fossa area and around the stump of the appendix and trocar sites at the end of the procedure; Group 3: 5 mL of 0.5% levobupivacaine was applied at the three trocar insertion sites and 10 mL 0.5% levobupivacaine was injected under direct vision in the right iliac fossa area and around the stump of the appendix and trocar sites at the end of the procedure; Group 4: 5 mL of 0.5% ropivacaine and 10 mL 0.5% ropivacaine was injected under direct vision in the right iliac fossa area and around the stump of the appendix and trocar sites at the end of the procedure.
The anesthesiologist followed the standard anesthesia protocol for laparoscopic operations. Anesthesia was induced with fentanyl, propofol, and pavulon. Anesthesia was maintained using 2%–3% sevoflurane and 50% nitrous oxide in oxygen. No nasogastric probe or urinary catheters was used in any of the 4 groups.
Data collection
The parameters were as follows: age and gender of the patient, the number of postoperative days, pain intensity according to the visual analogue scale (VAS) at the following locations: trocar sites, appendix, and shoulder and localization of pain before surgery. We also evaluated the type of pain (dull, sharp, and constant), nausea, and vomiting; the establishment of peristalsis and the onset of oral feeding; the use of analgesics and antibiotics; postoperative complications; and the adverse effects of local anesthetic application.
Postoperative pain assessment
Two hours after the end of the operation, the pain score was evaluated on the basis of a VAS. The patient was asked to evaluate their pain intensity in three locations: at the spot of the most painful incision site, the site of the appendix, and the intensity of pain in the shoulder. To measure pain intensity, the VAS (0–10 scale) pain score was measured by a blinded investigator at 2, 4, 8, 12, 24, and 48 hours after surgery. The presence of nausea and vomiting was monitored during the first 48 hours after the intervention.
Operative procedure
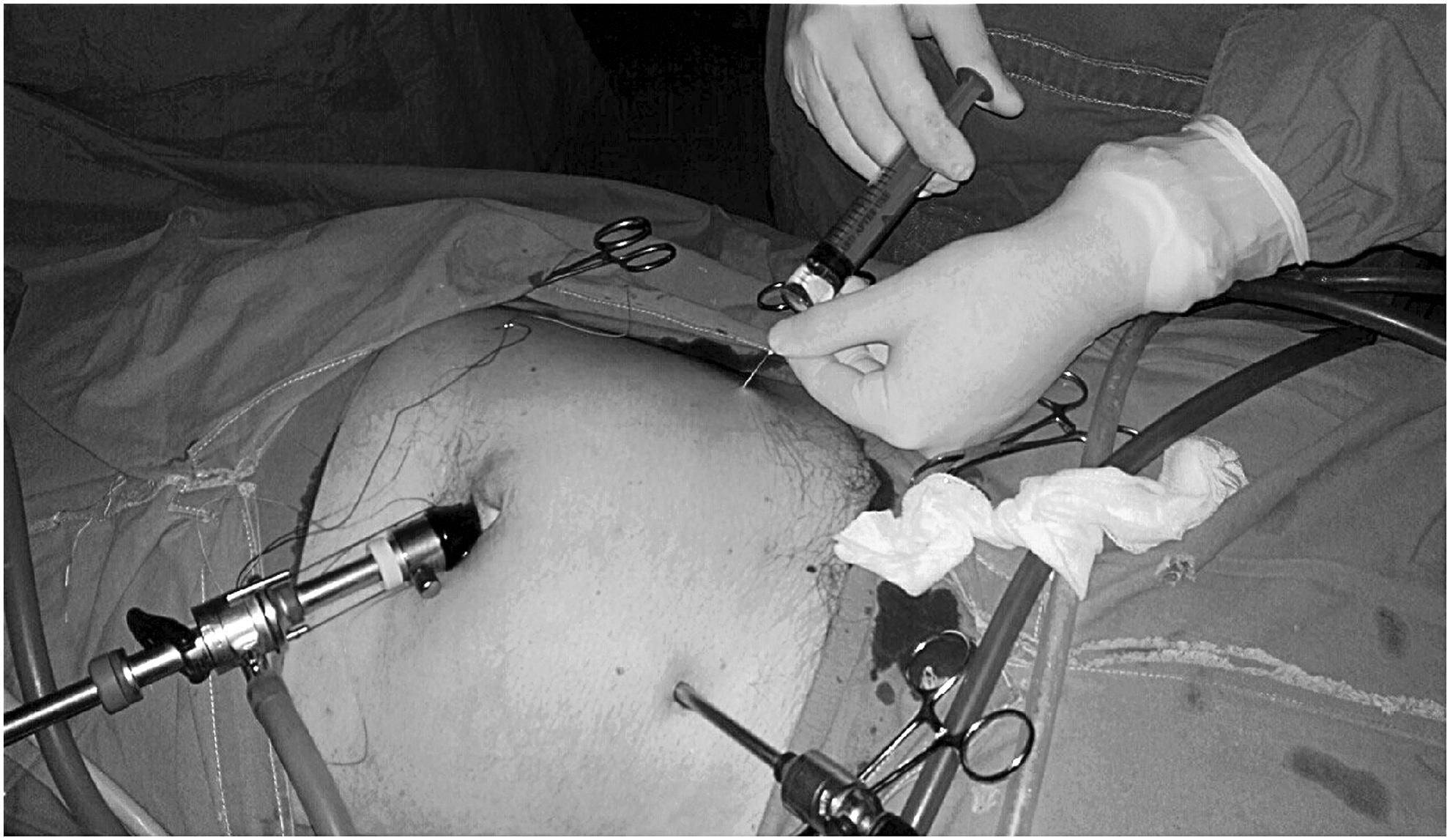
The same team of surgeons carried out all operations. Before incision, 5 mL of local anesthetic was applied in three intervention groups (1% lidocaine group, 0.5% levobupivacaine group, and 0.5% ropivacaine group) at the three trocar insertion sites (Fig. 1). The LA was performed using a two-handed, three-trocar technique (Fig. 2). 9 The mesoappendix was dissected using a harmonic scalpel (Ethicon Endo-surgery). The appendix was doubly ligated with 2-0 Vicryl loop at its base, and was then divided.

Instillation of local anesthetics at the trocar insertion site.
Trocar placement for laparoscopic appendectomy.
Intraperitoneal local anesthetic application
After completing the LA, 10 mL of local anesthetic was dispersed through a 5 mm trocar using the appropriate nebulizer at the site of the appendix and the surrounding tissue, in all three intervention groups (the 1% lidocaine, 0.5% levobupivacaine, and 0.5% ropivacaine groups) (Fig. 3). No local anesthetic was applied in the control group.
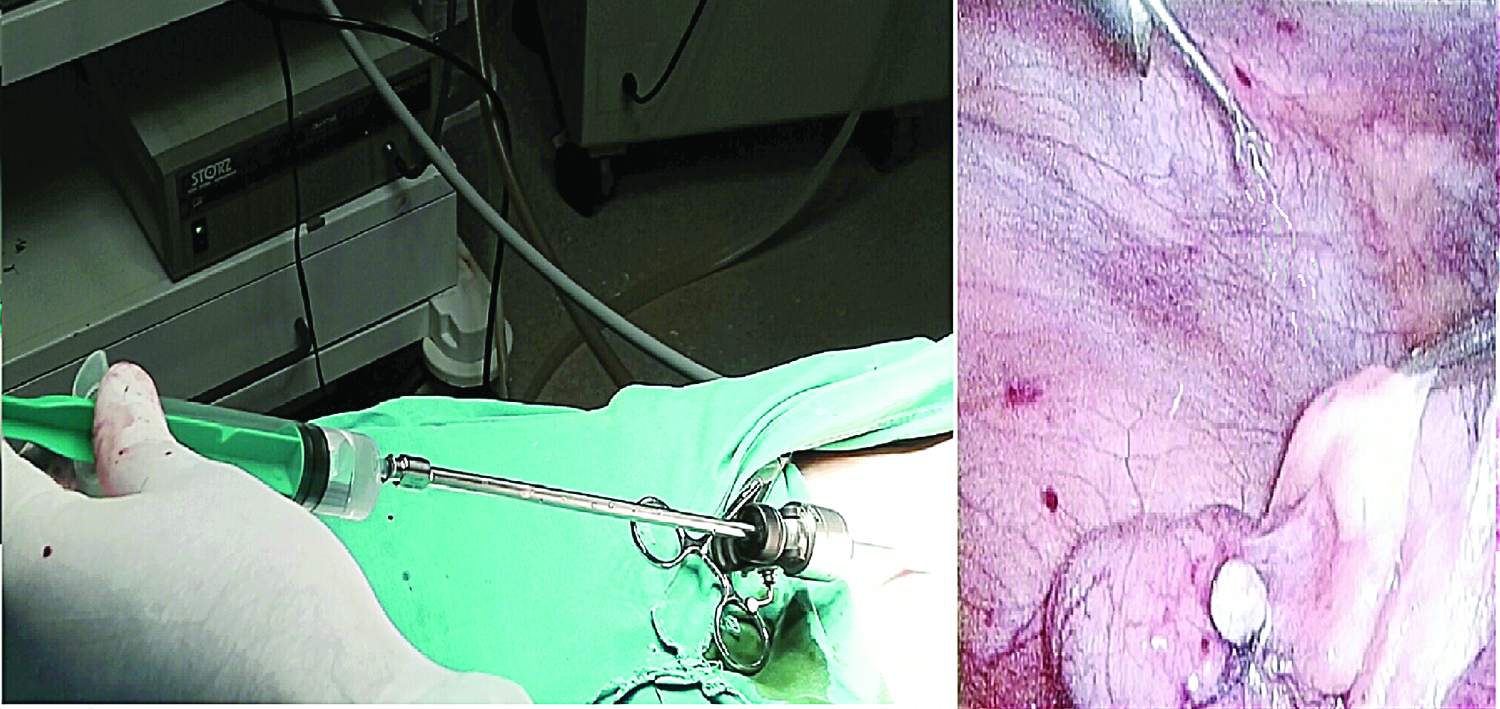
Application of local anesthetics through trocars in the right iliac fossa area and around the stump of the appendix.
Postoperatively, all patients received the same analgesics. In some cases of severe pain, additional analgesics were given to the patients and that was noted. After the start of oral feeding, oral analgesics were administrated.
Statistical analysis
An unpaired t-test for between-group comparison was performed for continuous variables. Descriptive variables were analyzed either by the χ2 test or Fisher's exact test, as appropriate. P < .05 was considered to be statistically significant. The data are reported as mean values with variability expressed as standard deviation. Statistical analyses were performed using the SPSS statistical package.
Results
A total of 120 patients (57 men and 63 women) included in the study were randomized into 4 groups. The average age of the patients was 32.4 years. There were no significant differences between the 4 groups with respect to age, height, weight, ASA class, and duration of anesthesia and surgery. The average duration of hospitalization was 3.45 days for all patients. The average duration of hospitalization for the levobupivacaine and lidocaine groups was 3.1 days and for the ropivacaine group 3.1 days. These differences between the groups are not statistically significant (P > .05). The average number of postoperative days was 2.57 for the control group, 2.37 for the levobupivacaine and lidocaine groups, and 1.9 days for the ropivacaine group. These differences between the groups are not statistically significant (P > .05), except for the difference between the control group and the levobupivacaine group (P < .05).
Pain after appendectomy
Pain after 2 hours
Statistically nonsignificantly different VAS values were recorded in patients with different appendix sites after 2 hours (P > .05). The most common appendix localization was the iliac. The lowest VAS score (2.88) was observed in the levobupivacaine group, in the pelvic localization. The results of the VAS pain scores after 2 hours are given in Table 1.
Pain Intensity According to the Appendix Site and Local Anesthetics Applied, After 2 Hours
There was no appendicitis in subhepatic site.
VAS, visual analogue scale.
Pain after 6 hours
Statistically nonsignificantly different VAS values were recorded in patients with different appendix sites after 6 hours (P > .05). The lowest VAS score (2.33) was observed in the levobupivacaine group, in the retrocecal localization. The results of the VAS pain scores after 6 hours are given in Table 2.
Pain Intensity According to the Appendix Site and Local Anesthetics Applied, After 6 Hours
There was no appendicitis in subhepatic site.
VAS, visual analogue scale.
Pain after 12 hours
Statistically nonsignificantly different VAS values were recorded in patients with different appendix sites after 12 hours (P > .05). The lowest VAS score (1.83) was observed in the levobupivacaine group, in the retrocecal localization. The results of the VAS pain scores after 12 hours are given in Table 3.
Pain Intensity According to the Appendix Site and Local Anesthetics Applied, After 12 Hours
There was no appendicitis in subhepatic site.
VAS, visual analogue scale.
Pain after 24 hours
Statistically nonsignificantly different VAS values were recorded in patients with different appendix sites after 24 hours (P > .05). The lowest VAS score (1.33) was observed in the levobupivacaine group, in the retrocecal localization. The results of the VAS pain scores after 24 hours are given in Table 4.
Pain Intensity According to the Appendix Site and Local Anesthetics Applied, After 24 Hours
There was no appendicitis in subhepatic site.
VAS, visual analogue scale.
Pain after 48 hours
Statistically nonsignificantly different VAS values were recorded in patients with different appendix sites after 48 hours (P > .05). The lowest VAS score (1.00) was observed in the levobupivacaine group, in the retrocecal localization. The results of the VAS pain scores after 24 hours are given in Table 5.
Pain Intensity According to the Appendix Site and Local Anesthetics Applied, After 48 Hours
There was no appendicitis in subhepatic site.
VAS, visual analogue scale.
Average pain intensity according to VAS
By comparing the average values of pain intensity according to the VAS, we may conclude that there is a statistically significant difference between the average values of pain intensity in the levobupivacaine and ropivacaine groups in relation to the control group (P < .05) during the whole period (Table 6).
P Values of the Comparison of the Tested Groups with Respect to the Intensity of the Pain According to Visual Analogue Scale
The values are given in the standard form of 10a. Each value < .05 is significant (bold), there is < 5% chance that the difference is random.
If we compare the lidocaine and the control groups, we may conclude that average pain intensity values are lower in the lidocaine group, but the differences are not statistically significant after 2, 6, and 12 hours (P > .05). After 24 and 48 hours the difference in pain intensity was statistically significant (P < .05).
The average values of pain intensity according to the VAS are given in Figure 4. It is evident that the average pain intensity values decrease progressively in the postoperative period and the differences in these values are statistically significant in all patients (P < .05).
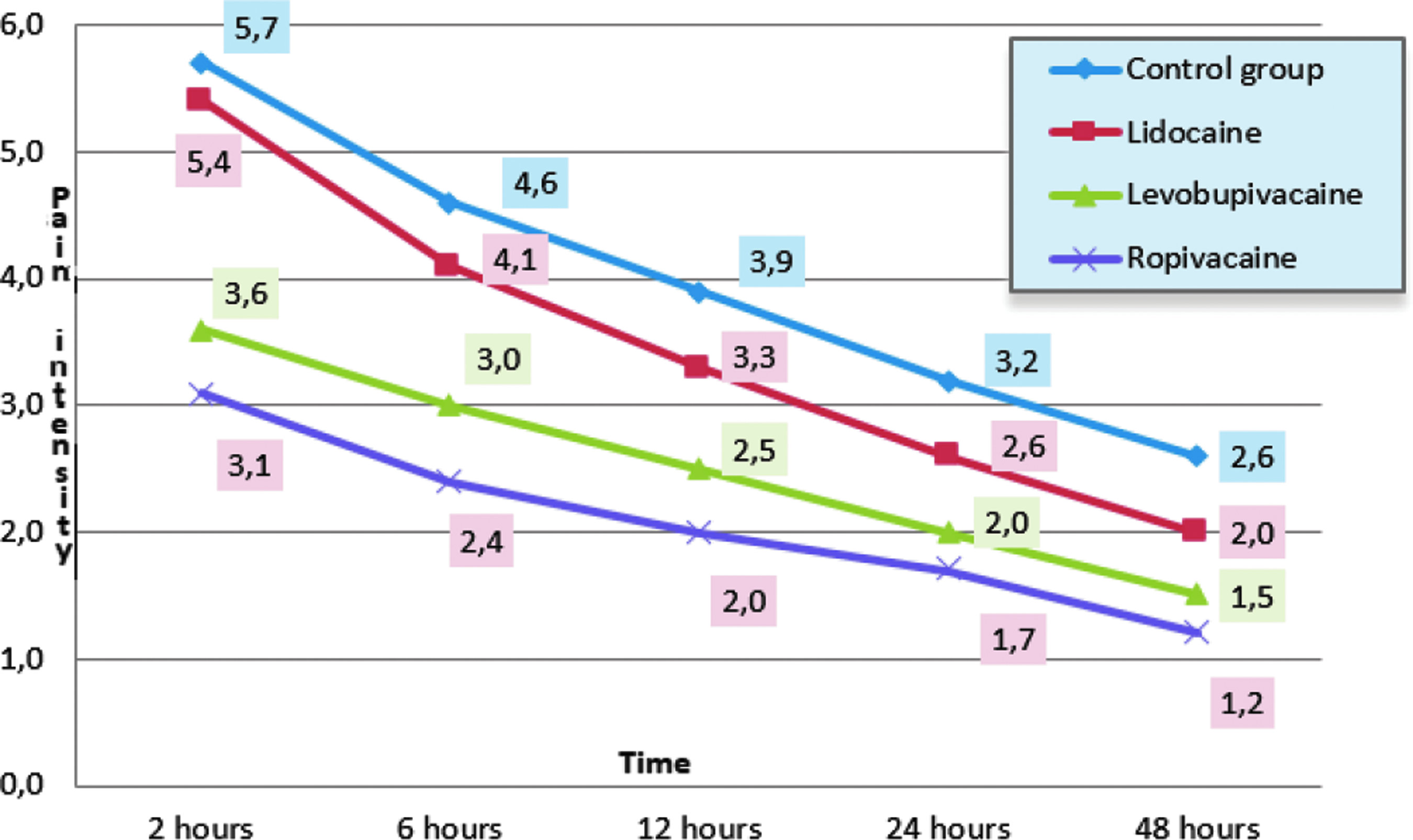
Average pain intensity according to VAS and local anesthetic applied. VAS, visual analogue scale.
Localization of pain
There are no statistically significant differences in the distribution of pain localization in relation to the patient group (P > .05).
Pain in the right shoulder
Of the total number of patients, 33 patients (19.2%) had pain in the right shoulder after LA. Most often the pain occurred in patients in the control group, in 13 patients (43.4%); then substantially less in the lidocaine group, 5 patients (16.7%); the levobupivacaine group, 3 patients (6.7%); and the ropivacaine 2 patients (6.7%). In relation to the control group, there were statistically significant differences (P < .05) in relation to the lidocaine group, the levobupivacaine group, and the ropivacaine group, P < .01 (Table 7).
Frequency of Pain in the Right Shoulder
The character and frequency of pain
There were no statistically significant differences in the distribution, character, and frequency of pain in relation to the patient groups examined (P < .05).
In total, 12 patients had pain that the patients designated as sharp and 108 patients designated their pain as dull. Overall, the pain was documented by 8 patients as continuous, and by 108 patients as occasional.
Postoperative nausea and vomiting
Thirty-seven (30.8%) patients had postoperative nausea. In the control group, more than half the patients had postoperative nausea, that is, 17 (56.7%). In the lidocaine group, 11 patients (36.7%) had postoperative nausea. The levobupivacaine group had 4 patients with nausea (13.3%), and in the ropivacaine group there were 5 patients (16.7%) with nausea. The difference between the control and the lidocaine group was not statistically significant (P > .05); however, the differences between the control group and the ropivacaine group and the control group and the levobupivacaine group were statistically significant (P < .01).
Discussion
The application of local anesthetics early in the preincision period (preemptive analgesia) leads to a reduction in postoperative pain in many types of elective surgical procedures.10–13 Preemptive preclinical infusion of bupivacaine caused a significant reduction in pain in open appendectomy according to the VAS. 14
In this study, the method of preemptive application of local anesthetics was used, using anesthetic infiltration at the sites of the incision, immediately before the incision itself, and the postemptive application of an intraperitoneal local anesthetic in the area of the appendectomy and its environment.
The strongest pain was observed in patients who had not been administered a local anesthetic. Comparing the average value of pain intensity according to the VAS, we may conclude that there is a statistically significant difference in the average intensity of pain in the levobupivacaine and ropivacaine groups compared with the control group.
It may be concluded that the most effective anesthetic was levobupivacaine, after which the intensity of the pain was statistically significantly lower than in any other examined group, and that superiority remained until 48 hours. The second most efficient local anesthetic was ropivacaine, which showed superiority at all the observed intervals in relation to the control and lidocaine groups.
The effectiveness of the preemptive application of local anesthetics during LA was demonstrated earlier. Of the 3 groups, the ropivacaine, levobupivacaine, and the placebo groups, levobupivacaine was the best. 15 But, there is only one study that deals with intraperitoneal ropivacaine application in LA. 16 Ropivacaine is useful for preemptive analgesia, by spraying the peritoneum, including the upper liver surface and subdiaphragmatic space in the Trendelemberg position. After that, a local anesthetic was applied to the area around the pelvis before the start of the LA, 16 as opposed to our study, where ropivacaine was applied only after LA. It was found that the pain according the VAS was significantly lower in the ropivacaine group, except after 24 hours. In our study, this difference for levobupivacaine and ropivacaine was statistically significant in relation to the control group and the lidocaine group.
There is only one study that deals with bupivacaine application in LA 17 in which bupivacaine was given preemptively to the sites of the incision and the insertion of the trocars. Bupivacaine was not administered intraperitoneally. In our search of the available literature, however, we did not find any study comparing the effects of levobupivacaine and lidocaine.
If we take into account the position of the appendix and the severity of pain, we may conclude that the pain is least pronounced if the appendix was in the retrocecal position, but this difference is not statistically significant in relation to the other appendix positions.
In our study, in the ropivacaine group shoulder pain was confirmed in 2 patients (6.7%), whereas in the control group, this pain was reported in 13 (43%) patients, and this difference was statistically significant (P < .01). In the lidocaine group, a significant difference in the frequency of pain in the right shoulder (P < .05) was also found in comparison with the control group. If clonidine, buprenorphine, and dexamethasone are added to a local anesthetic, the local anesthetic's efficiency is increased. 18
One of the most undesirable effects of anesthesia is PONV. The incidence of nausea, according to some studies, ranges from 22% to 38%, and vomiting from 12% to 26%. 19 In our study, the rate of nausea was 30.8% if all investigated groups of patients were considered. However, in the control group, postoperative nausea was determined at as much as 56.7%. In the levobupivacaine group, 4 patients or 13.3% had postoperative nausea. In relation to the control group, the difference was statistically significant. Compared with the results of other studies, we may say that postoperative nausea is less likely to occur. Therefore, we can conclude that the intraperitoneal application of levobupivacaine significantly reduces the occurrence of nausea after LA, which, with the statistically significant reduction in pain, significantly affects the postoperative comfort of the patient. In the ropivacaine group, 16.7% of patients had postoperative nausea that was slightly higher than that with levobupivacaine, although the difference was not statistically significant (P > .05).
The increase in intraoperative opioid administration leads to an increase in PONV. The pain decreases, but the incidence of PONV increases, and hence an optimal balance in opiate administration is required. 20 Therefore, local anesthetics and their analgesic effect have special significance. The use of local anesthetics in our study caused a decrease in the incidence of nausea and vomiting, which was statistically significant with the use of long-acting anesthetics.
LA, compared with classical appendectomy has a shorter hospitalization time. 21 If we apply local anesthetics, then the pain is even less, and recovery and hospitalization are shorter. In our study, the average hospitalization time was 2.3 days. Patients from the control group had longer hospitalization, lasting 2.57 days. In previous studies, the efficacy of anesthetic infiltration was demonstrated at the site of the trocar and the intraperitoneal cavity, so the hospital stay was shorter.16,22 In our study, patients from the levobupivacaine group went home soonest (1.9 days), although the difference was not statistically significant.
We can conclude that in patients in whom LA was performed owing to appendicitis, and intraoperatively local anesthetic was administered preemptively at the incision sites and postemptively intraperitoneally, there was a reduction in postoperative pain, nausea, and vomiting. After the application of levobupivacaine, the intensity of pain was significantly lower than in any other tested group.
We suggest that this is a safe method that leads to a reduction in health care costs because of shortening the length of hospital stay, lower postoperative consumption of analgesics, and a quicker return to daily activities.
Footnotes
Disclosure Statement
No competing financial interests exist.