
Abstract
Abstract
Background:
This systematic review and meta-analysis were performed to summarize available evidence comparing totally minimally invasive pancreaticoduodenectomy (TMIPD) versus open pancreaticoduodenectomy (OPD)
Materials and Methods:
We searched PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov for comparative cohort studies published from January 1990 through April 2018 comparing TMIPD versus OPD. Outcomes evaluated were postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), postoperative hemorrhage, wound infection, estimated blood loss, transfusion rate, retrieved lymph nodes (RLNs), R0 rate, reoperation rate, length of hospital stay, and mortality. Statistical analysis was performed with Review Manager, version 5.3 (Cochrane Collaboration).
Results:
Sixteen comparative studies were included. Meta-analysis showed no significant difference between TMIPD and OPD in rates of POPF (risk ratio [RR] = 0.80; 95% confidence interval [CI]: 0.58–1.11; P = .18), DGE (RR = 0.80; 95% CI: 0.63–1.01; P = .06), postoperative hemorrhage (RR = 1.32; 95% CI: 0.87–2.00; P = .19), or reoperation (RR = 0.68; 95% CI: 0.45–1.05; P = .08). TMIPD resulted in fewer wound infections (RR = 0.49; 95% CI: 0.33–0.74; P = .0006), less blood loss (mean difference [MD] = 371.65 mL; 95% CI: −473.77 to −269.53; P < .00001), and lower transfusion rate (RR = 0.59; 95% CI: 0.48–0.72; P < .00001) than OPD. No significant differences were found in the rate of R0 resection (P = .32), RLNs (P = .09), hospital stay (P = .73), or mortality (P = .67). However, TMIPD had much longer operative times than OPD (MD = 80.78 minutes; 95% CI: 29.25–132.31; P = .002).
Conclusion:
TMIPD appears to be as safe and effective as OPD for periampullary disease. These findings need confirmation with large volume well-designed randomized controlled trials.
Introduction
Pancreaticoduodenectomy (PD) is a standard procedure for the treatment of periampullary disease. To address the high rate of postoperative morbidity, minimally invasive PD techniques have been developed since the 1990s. Gagner and Pomp 1 reported the first laparoscopic PD in 1994. The development of surgical instruments such as the da Vinci system allowed the introduction of robotic PD, which was first described in 2003. 2 Minimally invasive PD (MIPD) has developed rapidly in recent decades. MIPD procedures described in previous studies and meta-analyses include laparoscopic-assisted PD (LAPD), totally laparoscopic PD (TLPD), robotic-assisted PD (RAPD), robotic-laparoscopic PD (RLPD), and totally robotic PD (TRPD).3–8 However, the evidence concerning minimally invasive techniques remains scarce. In recent years, there have been many additions to the literature regarding minimally invasive approaches to PD,4,9 including several studies that have compared the safety and efficiency of MIPD versus open PD (OPD).10–12 Because of the difficulty of extensive dissection and reconstruction, many previous studies on MIPD have included hand-assisted MIPD. Few studies have compared the safety and feasibility of total MIPD (TMIPD, including TLPD, TRPD, and RLPD) versus OPD. We aimed to perform an up-to-date meta-analysis comparing TMIPD with conventional OPD.
Materials and Methods
Search strategy
Two authors (Y.X.C. and B.W.) independently conducted systematic searches of PubMed, Embase, Web of Science, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov to find articles published through April 2018. TMIPD was defined as PD performed totally laparoscopically or robotically. English search terms included but were not limited to the following: “minimally invasive,” “laparoscopy,” “robot,” “robotic,” “Da Vinci,” “pancreaticoduodenectomy,” “Whipple,” “PD,” and “pancreatic resection.” References listed in the articles identified in the initial search were also manually reviewed. The language of the publications was confined to English.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were the following: (1) prospective or retrospective comparative study assessing surgical outcomes of TMIPD and OPD and including >20 cases and (2) availability of adequate raw data for categorical outcomes.
We excluded review articles, case reports, abstracts, editorials, and letters to the editor; articles published repeatedly by the same author or agency; articles published in any language except English; and articles with insufficient data on outcome measures.
Outcome measures
The outcomes investigated in this study included postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), postpancreatectomy hemorrhage (PPH), wound infection, estimated blood loss (EBL), transfusion rate, number of retrieved lymph nodes (RLNs), R0 resection rate, reoperation rate, length of hospital stay, and mortality rate. POPF, DGE, and PPH were diagnosed in accordance with the criteria of the International Study Group for Pancreatic Fistula (ISGPF).13–16 Clinically relevant POPF (CR-POPF) in this meta-analysis was defined as ISGPF Grade B/C. 13 Mortality was defined as postoperative death from any cause.
Data extraction
Two authors (Y.M.X. and W.B.D.) independently extracted the original data from the literature to ensure the homogeneity of the extracted data. The standardized selection form included the first author, year of publication, type of study, country in which the study took place, study period, TMIPD procedure, and sample size. Conflicts in data abstraction were resolved by consensus, with reference to the original article. Extracted data were entered in a pregenerated standard Microsoft Excel file (Microsoft Corporation, Redmond, WA).
Risk-of-bias assessment
The Newcastle–Ottawa Quality Assessment Scale was used to evaluate the quality of the nonrandom studies. The scale ranges from 0 to 9 stars: studies with a score of 6 or higher were deemed methodologically sound.
Statistical analysis
All statistical analyses were performed with the Review Manager (RevMan), version 5.3 (Cochrane Collaboration). Risk ratios (RRs) with 95% confidence intervals (CIs) were used for dichotomous outcomes; the weighted mean difference (MD) was used to assess continuous variables. A two-tailed P value of <.05 was considered statistically significant. We also assessed the potential for publication bias through a visual inspection of funnel plot asymmetry.
Results
Study selection and characteristics of the trials
With our search criteria, we identified 2198 articles that focused on the use of TMIPD; of these, 1647 duplicate articles were excluded. The remaining 551 studies were retrieved on the basis of their titles and abstracts. Sixteen of these studies, involving 1896 participants, met the eligibility criteria and were included in the meta-analysis.7,10,11,17–29 A detailed flowchart of the selection process is shown in Figure 1.

PRISMA flow diagram of the meta-analysis.
The 16 included studies were conducted in eight countries: TMIPD procedures included TLPD (8 studies),7,23,24,26–29 TRPD (2 studies),17,19 RLPD (5 studies),18,20–22,25 and TLPD combined with RLPD (1 study). 10 The 1898 patients were divided into the TMIPD group (721 patients) and the OPD group (1177 patients). The sample sizes of the studies ranged from 28 to 322 patients; the year of publication ranged from 2011 to 2017. The general characteristics of included studies are given in Table 1.
General Characteristics of the Included Studies
ISGPF, International Study Group for Pancreatic Fistula; LTPD, laparoscopic total pancreaticoduodenectomy; MIPD, minimally invasive pancreaticoduodenectomy; OPD, open pancreaticoduodenectomy; PF, pancreatic fistula; RLPD, robotic-laparoscopic pancreaticoduodenectomy; RTPD, robotic total pancreaticoduodenectomy; NA, data not available; NOS, Newcastle–Ottawa Quality Assessment Scale.
Methodological quality and risk of bias
The methodological quality of the included studies was evaluated by 2 investigators (Y.X.C. and B.W.) and is given in Table 1.
Outcome Measures
Clinically relevant postoperative pancreatic fistula
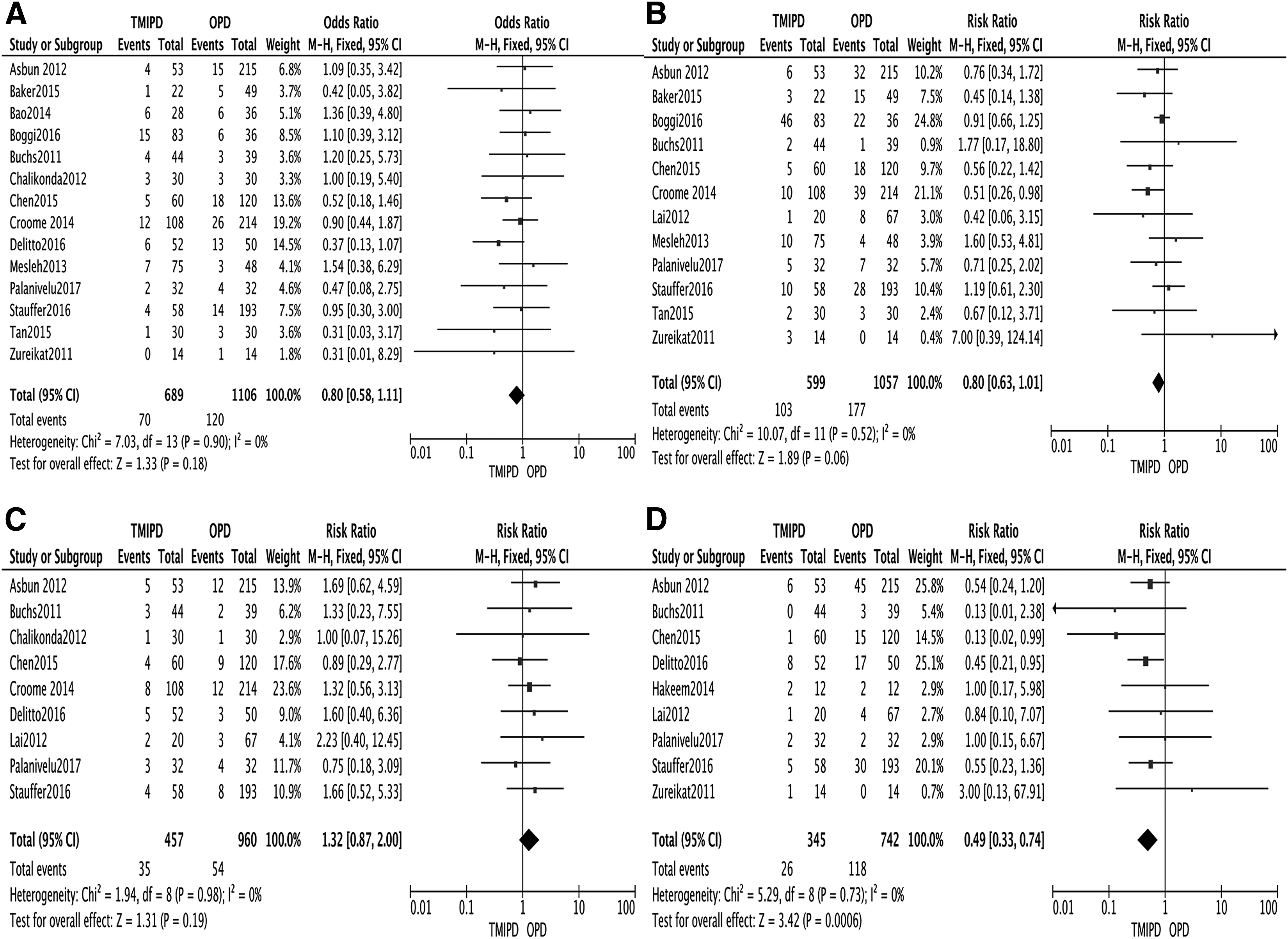
Among the 16 studies, 12 reported CR-POPF, which is considered a serious complication after PD. This meta-analysis found no significant difference in the incidence of CR-POPF between the TMIPD and OPD groups (RR = 0.80; 95% CI: 0.58–1.11; P = .18) (Fig. 2).
Forest plot of the meta-analysis:
Delayed gastric emptying
The incidence of DGE tended to be lower in the TMIPD group than in the OPD group, although the difference was not statistically significant (RR = 0.80; 95% CI: 0.63–1.01; P = .06) (Fig. 3).
Forest plot of the meta-analysis:
Postpancreatectomy hemorrhage
Nine trials provided data for meta-analysis of PPH; no significant difference in PPH was found between TMIPD and OPD groups (RR = 1.32; 95% CI: 0.87–2.00; P = .19) (Fig. 4).
Forest plot of the meta-analysis:
Wound infection
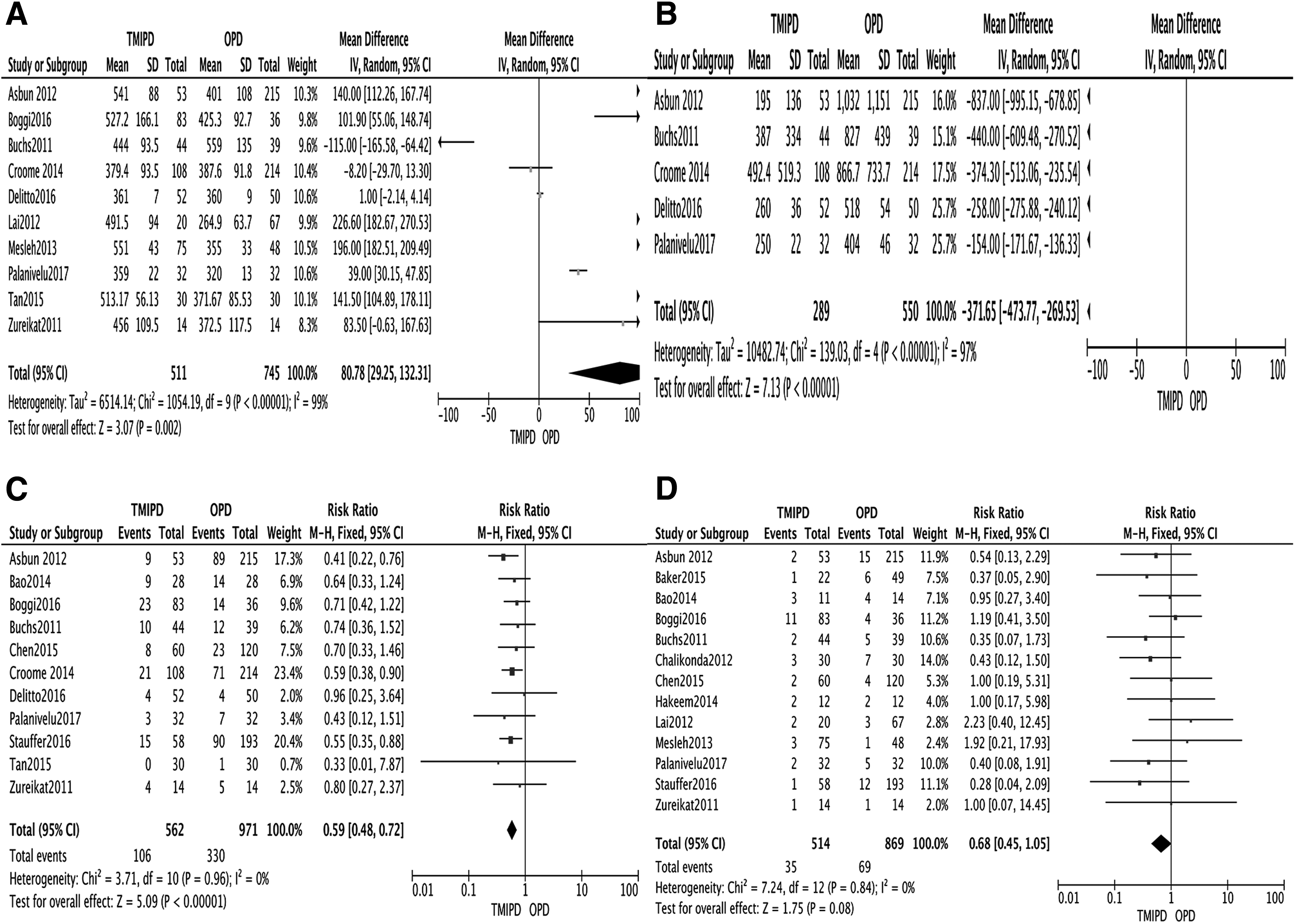
The data from nine trials, including 1087 patients, demonstrated that TMIPD resulted in fewer wound infections than OPD (RR = 0.49; 95% CI: 0.33–0.74; P = .0006).
Operation time
Ten trials reported operation times. There was a significant difference in operation time between the groups (MD = 80.78 minutes; 95% CI: 29.25–132.31 minutes; P = .002).
Estimated blood loss
Five studies provided EBL data; meta-analysis showed that TMIPD was associated with less intraoperative EBL (MD = 371.65 mL; 95% CI: −473.77 to −269.53 mL; P < .00001).
Transfusion rate
The TMIPD group had a significantly lower transfusion rate than the OPD group (RR = 0.59; 95% CI: 0.48–0.72; P < .00001).
Reoperation rate
Thirteen studies involving 1383 patients reported reoperation rates; there was no significant difference in reoperation rate between TMIPD and OPD groups (RR = 0.68; 95% CI: 0.45–1.05; P = .08).
Retrieved lymph nodes
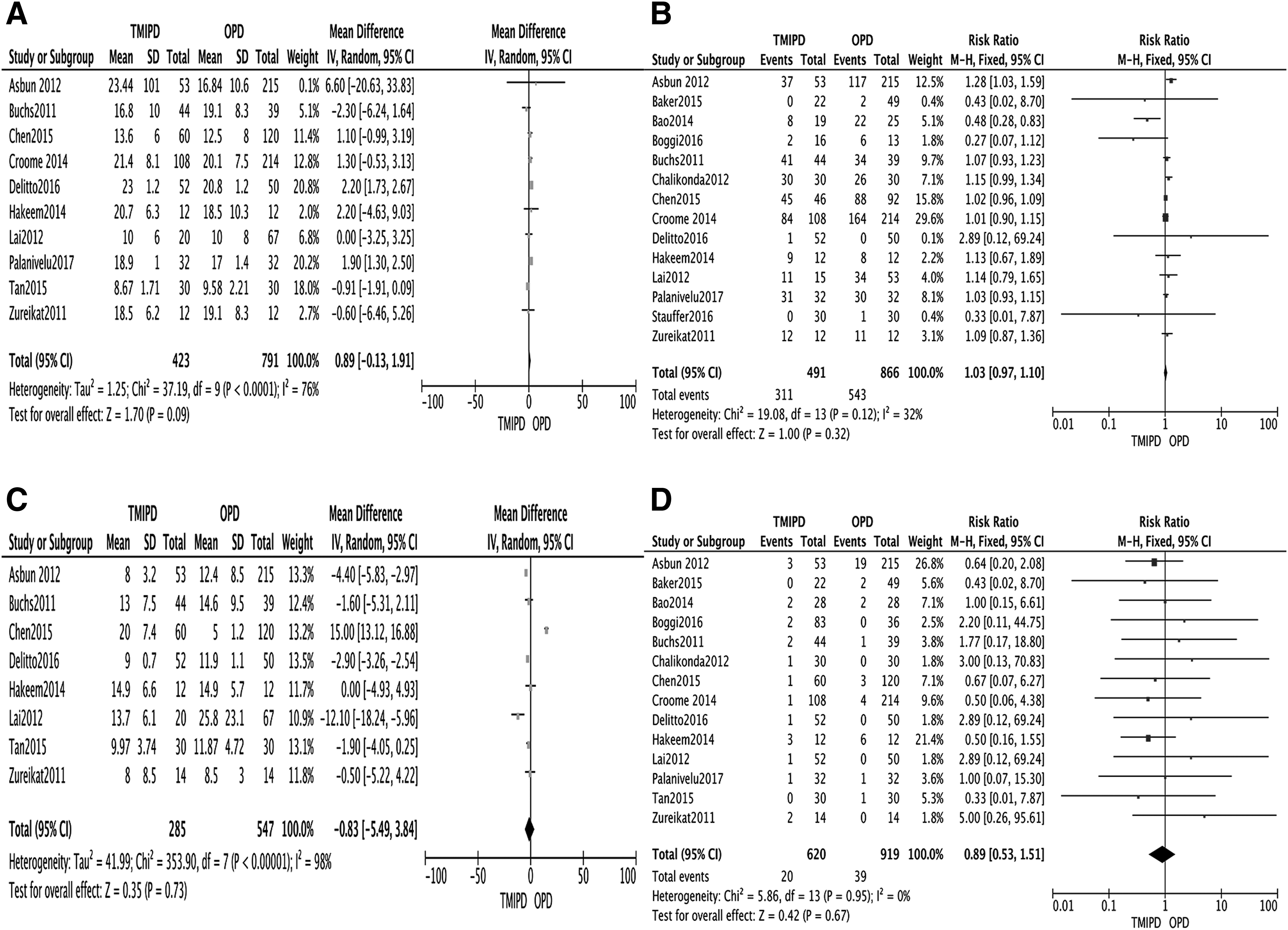
Ten included studies reported the number of RLNs; results of meta-analysis showed no significant differences in RLNs between TMIPD and OPD groups (RR = 10.89; 95% CI: −0.13 to 21.91; P = .09).
R0 resection rate
The R0 resection rate was reported for 1375 patients; results showed no significant difference between TMIPD and OPD groups (RR = 1.03; 95% CI: 0.97–1.10; P = .32).
Hospital stay
Eight trials reported data on length of hospital stay. There was no significant difference in length of hospital stay between TMIPD and OPD groups (MD = −0.83 days; 95% CI: −5.49 to 3.84 days; P = .73).
Mortality
Fourteen studies compared mortality rates between groups. The result of this meta-analysis showed no significant difference in mortality rates between the TMIPD and OPD groups (RR = 0.89; 95% CI: 0.53–1.51; P = .67).
Sensitivity analysis
The influence of any single study on the overall meta-analysis estimates was investigated by omitting one study at a time. The omission of any single study made no significant difference in results, indicating that our results were statistically reliable.
Publication bias
Most graphical funnel plots of the parameters were symmetrical. Egger's test revealed no significant publication bias.
Discussion
Our up-to-date meta-analysis included 16 trials that provided the most reliable and robust evidence related to TMIPD and OPD. The results of this study revealed no significant differences between the two procedures in CR-POPF, DGE, PPH, or reoperation rate. Similar results were also observed in the R0 resection rate, RLNs, length of hospital stay, and mortality. TMIPD was associated with less EBL, a lower incidence of wound infection, and lower transfusion rate than OPD, but was associated with longer operative times.
POPF is the most common serious complication after PD. CR-POPF, especially Grade C POPF, is strongly associated with postoperative recovery. CR-POPF, with a prevalence of 5% to 45% after PD,30,31 remains a clinically relevant problem. The CR-POPF rates in this study ranged from 3.57% to 31.25%. The present analysis revealed no significant difference in CR-POPF rates between TMIPD and OPD groups. Similar results have also been observed in previous studies.3,4 However, in many previous meta-analyses, the MIPD procedure included not only totally minimally invasive approaches but also LAPD or RAPD. Our results indicate that TMIPD is as safe as OPD for pancreatic fistula avoidance. It is worth noting that the definition of pancreatic fistula has varied in previous studies. In the present meta-analysis, the criteria of the ISGPF were used to define CR-POPF. However, the included studies ignored pancreatic texture and pancreatic duct diameter. These two factors are closely related to the occurrence of CR-POPF. 13
Our results indicate that TMIPD had no advantage over OPD in avoiding DGE or PPH. However, DGE and PPH data are variable in previous studies.5,6 Possible reasons for this variability include differences in the MIPD procedure and in the definition of MIPD. These results suggest that TMIPD has some degree of safety in terms of CR-POPF, DGE, and PPH.
Postoperative mortality is an important measure of the safety of surgical procedures. This pooled review revealed no differences in mortality between the TMIPD and OPD groups. However, not all included trials clearly reported mortality. It is challenging for surgeons to report unpleasant complications; the heterogeneity of patients' characteristics in previous studies could also lead to bias. Therefore, more high-quality data and studies are needed to further evaluate overall complication rates.
Our results suggest that TMIPD has advantages over OPD in EBL and transfusion rate. Intraoperative EBL is an important indicator of the safety of PD. 3 EBL in this pooled review was lower in the TMIPD group than in the OPD group, as was the need for transfusions. The use of laparoscopic or robotic assistance broadens the surgeon's view of the structures surrounding the intended surgical site. More precise resection results in less bleeding. It is worth noting that in preoperative assessment, those patients with an increased risk of intraoperative blood loss are more likely to have OPD. 32 Comparison of operative blood loss requires high-quality articles with matched cases.
A minimally invasive approach in abdominal surgery has been shown to be associated with lower rates of wound infection. 33 As in previous studies,4,34 our meta-analysis confirmed that patients who underwent TMIPD had fewer wound infections than patients who underwent OPD. A minimally invasive approach limits contamination of the surgical site because of the comparatively small abdominal incisions.
The operative time was significantly longer for TMIPD than for OPD, a common feature observed in other laparoscopic procedures. The longer duration of laparoscopic PD has several explanations, including the complexity of the overall procedure, hemorrhage control of the major vasculature, difficulty in accessing and exposing the pancreas, and the technically demanding reconstruction of the biliary and pancreatic ducts. 35 In contrast, recent studies have shown that hand-assisted laparoscopic operations do not last significantly longer than open operations.36–39 With ongoing advances in technology and accumulation of experience, surgeons who perform many MIPD surgeries may become more skillful. Buchs et al. reported that the operative time for laparoscopic procedures was lower than that for open procedures. 20
Previous studies have indicated that the type of MIPD surgery does not significantly influence reoperation rates compared with OPD surgery.3–5 The common causes of reoperation in the included trials were PPH, abdominal abscess, and sepsis.23,27 These outcomes were equivalent for MIPD and OPD in our meta-analysis. However, not all postoperative complications require reoperation. Patients with known vascular or other organ involvement before surgery were more likely to undergo OPD.40,41 As a result, these data should be interpreted with caution.
Decreased length of hospital stay is frequently cited as a benefit of minimally invasive operations. 42 However, previous studies have presented conflicting information about length of stay. As in our study, Adam et al. found no difference in length of stay between MIPD and OPD in a series of 7061 patients (983 MIPD and 6078 OPD) in the National Cancer Database. 43
Few studies reported long-term oncologic outcomes. Previous studies have shown that TLPD can be performed with good oncologic outcomes.10,44,45 The rates of R0 resection and lymph node retrieval are used as indicators of the oncologic adequacy of minimally invasive techniques. 32 Previous R0 and RLNs results have been variable. Zhang et al. reported that MIPD had a significantly higher R0 resection rate and more RLNs than OPD. 46 However, that study included trials in which LAPD and RAPD were performed. After excluding LAPD and RAPD studies, we found that TMIPD had no advantage over OPD in R0 rate or number of RLNs. The analysis of Rooij et al. revealed similar results. 6 A possible reason for these differences may be variations in tumor characteristics in previous studies. Another possible explanation is the preoperative selection of patients at low risk for positive-margin status. 47 Because few reports have compared long-term survival outcomes among methods, we did not have enough data to perform a meta-analysis of long-term oncologic results after MIPD versus OPD.
This meta-analysis has some limitations that must be considered. First, selection bias is a common problem in cohort studies. MIPD was often selected for patients with small tumors, no comorbidity, and no adiposity. Second, only one randomized controlled trial was included in this review, resulting in a lack of unbiased data. This is an important indication that the widespread application of these techniques is yet to be achieved. A third major limitation is the possibility of publication bias, in which centers and individual surgeons with positive MIPD outcomes are more likely to publish their findings than those with negative outcomes.
In conclusion, our systematic study demonstrates that TMIPD is feasible and safe for PD, especially at experienced centers. Because of the inherent limitations of our study, these findings need confirmation with large volume well-designed randomized controlled trials.
Footnotes
Acknowledgment
Authors' Contributions
Y.L. performed the experiment conception and design. Y.C. and B.W. performed the research and retrieved the data. Y.X., and W.D. performed the data analysis. Y.L. did the paper writing. All authors read and approved the final article.
Disclosure Statement
Y.L., Y.C., B.W., Y.X., and W.D. have no conflicts of interest or financial ties to disclose.