
Abstract
Abstract
Purpose:
Management strategies for acutely incarcerated/strangulated groin and obturator hernias may differ from institution to institution, although, conventionally, the open approach has been used. Recently, laparoscopic transabdominal preperitoneal (TAPP) repair and totally extraperitoneal (TEP) repair have become commonly used operative procedures for the repair of groin hernias. It is unclear whether laparoscopic reduction and herniorrhaphy can be successfully accomplished in all cases. This study was aimed at assessing the effectiveness of laparoscopic treatment.
Methods:
We conducted a prospective clinical trial of the laparoscopic approach from December 2011 and comparatively analyzed the surgical outcomes between the open and laparoscopic approaches for incarcerated/strangulated hernias seen from December 2000 to March 2017.
Results:
The open approach for repair was used in 54 patients (50.9%) and the laparoscopic approach in 52 patients (49.1%). There was 1 case in which from the laparoscopic approach to laparotomy (1.9%) was required. The operation time treated by the laparoscopic approach was significantly longer than the open approach (126.4 minutes versus 104.6 minutes; P = .0079); however, the incidence of postoperative complications and the postoperative length of hospitalization were also less in the former group than in the latter group (3.9% versus 18.5%; P = .0172 and 5.6 days versus 14.7 days; P = .0096). Second-stage TAPP herniorrhaphy was performed in 7 patients (15.2%) after bowel resection or closure of bowel perforation, and first-stage TEP herniorrhaphy was performed in 1 patient after bowel resection. There was no case of mesh infection in the group treated by the laparoscopic approach, and there was 1 case of mesh infection in the group treated by the open approach. The mortality rate was 0% in the group treated by the laparoscopic approach.
Conclusions:
Laparoscopic reduction and herniorrhaphy for acutely incarcerated/strangulated groin and obturator hernias is effective, safe, and feasible.
Introduction
E
Patients and Methods
We conducted a prospective trial of laparoscopic approach from December 2011 to March 2017 and a retrospective analysis of the clinical and surgical data of 106 patients with acutely incarcerated/strangulated groin and/or obturator hernias treated at the Institute of Gastroenterology from December 2000 to March 2017. Although reduction and herniorrhaphy was performed through the open approach in patients seen from December 2000 to November 2011, laparoscopic TAPP or TEP approach was performed in patients seen from December 2011 to March 2017 prospectively. Data regarding the age, gender, body mass index (BMI = weight [kg]/height [m]2), affected side, American Society of Anesthesiologists (ASA) grade, and type of hernia were collected from the medical charts.
We analyzed the surgical outcomes between the cases treated by the open and laparoscopic approaches. Before the operative treatment, we performed ultrasonography to determine the presence/absence of any bowel movements in the incarcerated bowel, as well as the confusion of the wall layer, and enhanced CT to determine the presence/absence of blood flow to the hernia contents. If external manual reduction failed, emergency operation was performed laparoscopically. All patients were operated upon under general anesthesia, and the hernia contents were reduced under laparoscopic observation. If there was no intra-abdominal contamination, with no bowel perforation or gangrene, first-stage TAPP hernia repair using a prosthetic mesh was performed without delay. If there was contamination, the umbilical port wound was extended, and the bowel was brought out of the abdominal cavity and resected, or the perforation was closed, and then elective laparoscopic repair was performed at a future occasion (second-stage TAPP). Even if external manual reduction was successful, laparoscopic intra-abdominal observation was performed as soon as possible. Furthermore, if it was impossible to obtain an adequate intra-abdominal field of view laparoscopically due to dilated bowel loops, repair was undertaken by the TEP approach (Fig. 1). The water pressure technique was used for laparoscopic reduction of incarcerated bowel using a (size, 8Fr.) Nelaton catheter, which was inserted through a 11- or 12-mm camera port using a 5-mm flexible camera and was controlled with forceps inserted through bilateral 5-mm ports. After insertion of the Nelaton catheter into the hernia sac, saline was injected (Fig. 2). 10
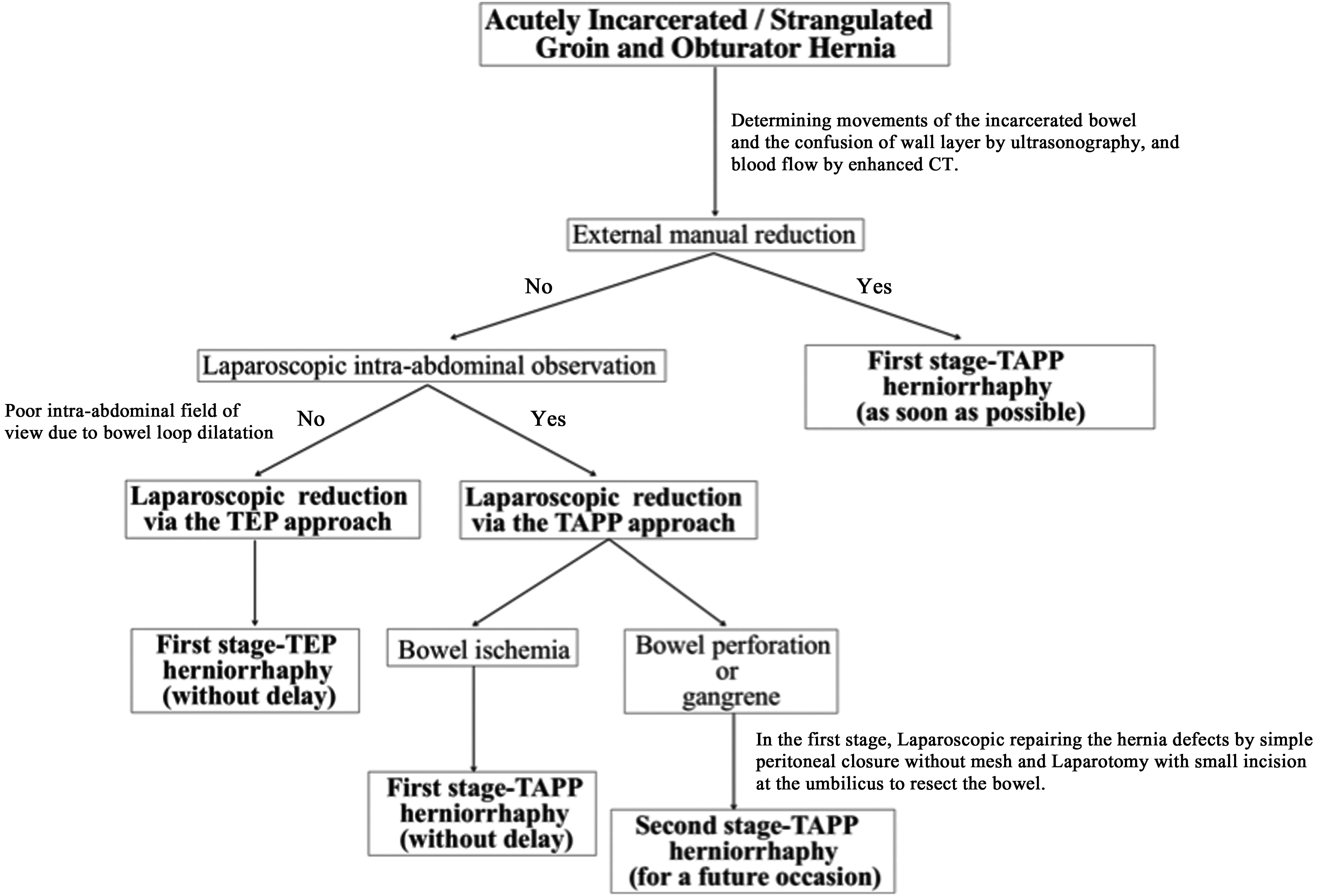
Clinical protocol for acutely incarcerated/strangulated groin and obturator hernias.
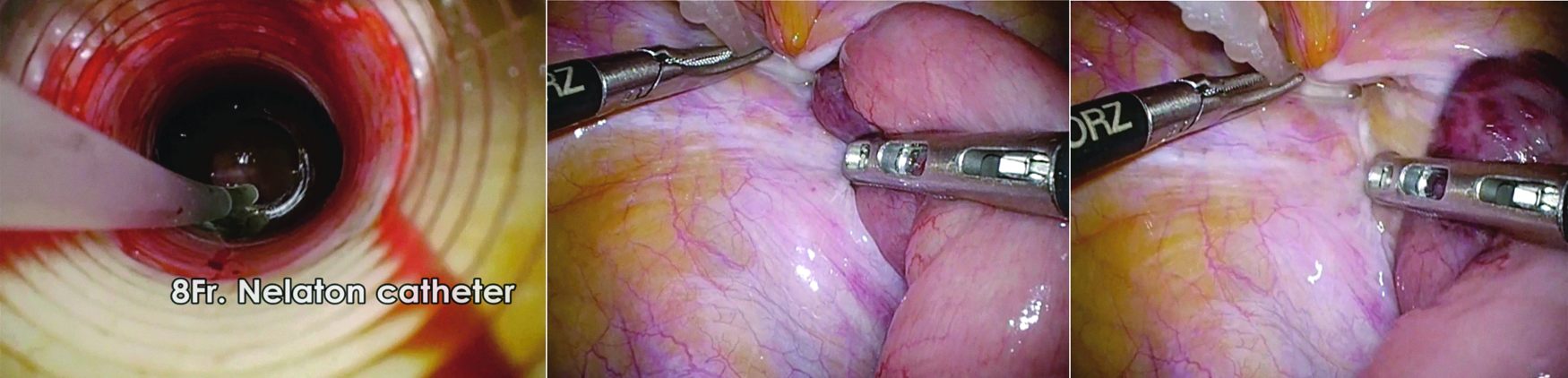
Laparoscopic reduction using the water pressure technique.
Data of the cases were obtained from the medical charts, and the following information was recorded to create a database: the incarcerated hernia contents, operation time, bowel resection or closure of the perforation, intra- and postoperative complications, interval to resumption of oral intake after the operation, postoperative length of hospitalization (in days), mortality, reduction technique, and presence/absence of mesh infection.
Open repair for herniorrhaphy
Open repair for groin and obturator hernias was performed under general anesthesia. The procedure is described as follows. The abdominal approach through an inguinal or low midline incision was made. Tension repair or prosthetic mesh repair was performed for groin hernia, and simple closure of obturator ring or prosthetic mesh repair for obturator hernia.
TAPP repair for herniorrhaphy
TAPP repair for groin and obturator hernias was performed under general anesthesia. The procedure is described as follows. The first port was created at the umbilicus. In addition, two working ports were created bilaterally, on either side of the umbilicus. The CO2 insufflation pressure was set at 8–10 mmHg. For the peritoneal incision, laparoscopic coagulating shears were used. After dissecting the preperitoneal space, a prosthetic mesh was inserted directly into the preperitoneal space and fixed with a resolvable tacker. The peritoneum was closed with a 3/0 multifilament absorbable suture or barbed absorbable suture. The same TAPP procedure as that for inguinal hernias was applied for obturator hernias, where the preperitoneal and prevesical space was sufficiently expanded to the obturator foramen, and a large enough mesh to sufficiently cover the myopectineal orifice and obturator foramen was used.
TEP repair for herniorrhaphy
TEP repair for groin and obturator hernias was performed under general anesthesia. The procedure is described as follows. First, a trocar was inserted at the umbilicus. If the initial laparoscopic view of the intra-abdominal space was not satisfactory due to bowel loop dilatation, the anterior fascia of the rectus was incised. An access device, consisting of a lap protector and EZ access (Hakko Medical Co., Ltd., Nagano, Japan) with a double 5-mm trocar, was introduced into the preperitoneal space. In addition, a working trocar was inserted at the middle point between the umbilicus and the pubis. The preperitoneal space was then expanded to the groin area.
Ethical considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Nippon Medical School Musashikosugi Hospital (approval no. 415-29-40).
Statistical analysis
The entire statistical analysis was performed using JMP, version 10 (SAS Institute, Inc., Cary, NC). Continuous variables (age, BMI, operation time, interval to resumption of oral intake after the operation, and postoperative length of hospitalization) are presented as the means ± standard deviation. The t-test was used for independent samples comparison of continuous variables. The χ2 test was used to compare categorical variables. P < .05 was considered to denote statistical significance.
Results
A clinical series of 106 patients (58 men and 48 women) underwent emergency surgery for acutely incarcerated groin or obturator hernias. The patient characteristics are shown in Table 1. Among them, 54 patients (50.9%) underwent treatment by the open approach and 52 (49.1%) by the laparoscopic approach. Information regarding the age, gender, BMI, hernia side, ASA grade, and type of hernia is shown. There was no statistically significant difference in the characteristics between the groups treated by the open approach (open group) and the group treated by the laparoscopic approach (laparoscopic group).
Values are presented as the mean ± SD or n (%).
ASA, American Society of Anesthesiologists; BMI, body mass index; SD, standard deviation.
The surgical outcomes are shown in Table 2. In regard to the contents of the incarcerated hernia, there were a lot of small bowel segments in both the open and laparoscopic groups (72.7% versus 63.5%). The operation time in the laparoscopic group was significantly longer than in the open group (126.4 minutes versus 104.6 minutes; P = .0079), but the incidence of postoperative complications and postoperative length of hospitalization was also less in the laparoscopic group than in the open group (3.9% versus 18.5%; P = .0172 and 5.6 days versus 14.7 days; P = .0096). There were 2 patients in the open group who died of aspiration pneumonia, whereas none of the patients in the laparoscopic group died. The overall mortality rate was 1.9%.
Values are presented as the mean ± SD or n (%).
POD, postoperative day; SD, standard deviation.
The surgical outcomes in the laparoscopic group are shown in Table 3. Laparoscopic reduction was performed through the TAPP approach in 46 patients, and through the TEP approach in 6 patients. The water pressure technique, which is a very gentle reduction technique, was successful in 6 patients (13%), including 3 cases of indirect inguinal, 2 cases of femoral, and 1 case of obturator hernia. In all of these cases in which the reduction was successful, the type of hernia was a Richter's hernia. Enlargement of the hernia orifice, with a releasing incision made at the lacunar ligament, was undertaken in 1 case of femoral hernia treated by the TEP approach. There was 1 case of massive scrotal inguinal hernia in which conversion from the laparoscopic TAPP approach to open surgery was required. Bowel resection was performed in 6 patients (13%) undergoing TAPP approach, and 1 patient (16.7%) undergoing TEP approach. Closure of bowel perforation was performed in 1 patient (2.2%), with only a simple suture, undergoing TAPP approach. Second-stage TAPP herniorrhaphy was performed in 7 patients (15.2%) after bowel resection/closure of bowel perforation, and first-stage TEP herniorrhaphy was performed in 1 patient after bowel resection.
Conversion to laparotomy due to incarcerated massive scrotal hernia.
TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal.
There were 92 cases (86.8%) of herniorrhaphy using a prosthetic mesh in laparoscopic and open cases. Comparisons of the bowel treatments are shown in Table 4. Mesh infection occurred in 1 patient of obturator hernia who underwent open repair after bowel resection. The mesh infection rate was 1.1% in all the cases in which a mesh prosthesis was used, and 6.7% in the 15 cases that underwent bowel treatment.
Herniorrhaphy was performed at second-stage TAPP repair.
TAPP repair was converted to the open approach to reduce the incarcerated bowel.
TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal.
Discussion
We demonstrated the usefulness of the laparoscopic approach for incarcerated/strangulated groin and obturator hernias; adoption of this approach was associated with significantly fewer postoperative complications and shorter postoperative length of stay at the hospital. There was only 1 case of conversion from the laparoscopic to the open approach, because a massive scrotal inguinal hernia was irreducible in this case under laparoscopic visualization. We believe that if we had made a releasing incision at the hernia orifice, successful reduction would have been accomplished even in this case with the massive scrotal hernia. 11
According to our criteria for laparoscopic treatment, we select the TEP approach when there is bowel dilatation. Entry into the preperitoneal plane can be performed safely, because the gaseous distension of the preperitoneal plane utilizes the peritoneum as a natural retractor, pushing away the distended intraperitoneal bowel loops. 8 There was 1 case of femoral hernia, in which reduction of the incarcerated bowel and herniorrhaphy were performed through the TEP approach at first. Subsequently, complete closure of the anterior rectus sheath was performed and a separate entry into the abdomen was created for laparoscopy. Then, bowel resection was performed because of necrosis. Fortunately, no frank pus, abscess formation or fecal matter within the sac, or any evidence of generalized peritonitis was observed in this case at the time of the laparoscopic intra-abdominal observation. Even, in cases of resection–anastomosis of nonviable bowel, an attempt to avoid contamination must be made by keeping the preperitoneal plane strictly separate from the intraperitoneal space. However, the hernia sacs of direct inguinal, femoral, and obturator hernias, but not those of indirect hernias, can be inverted. Therefore, it is necessary to detach the peripheral sac. There is a risk of contamination of the preperitoneal space if the detached peripheral sac is contaminated, in addition, even if the peritoneum has injury. The optimal approach for first-stage TEP herniorrhaphy in cases with prominent bowel dilatation is controversial and the open approach needs to be considered.
Mesh infection occurred in 1 case of obturator hernia who needed bowel resection in our case series. Although abscess formation occurred in the obturator foramen, we performed mesh plug herniorrhaphy. No case of mesh infection was encountered among the cases of herniorrhaphy performed through the TAPP approach. Second-stage TAPP herniorrhaphy was performed in 5 cases of bowel resection or closure of perforation, and bowel resection after first-stage TAPP was performed in 1 case of successful external manual reduction. In this latter case, since there was no intra-abdominal contamination, prosthetic herniorrhaphy was performed first. Then, a segment of nonviable bowel was found, necessitating bowel resection. There was 1 case of first-stage TEP herniorrhaphy who required bowel resection. Atila et al. reported that 14 adult patients with acutely incarcerated groin hernias who required bowel resection underwent prosthetic herniorrhaphy. All of the bowel resections were performed without any enteric contents contamination. 4 Bessa et al. also reported that there was no case of mesh infection in a series of 32 patients who required resection–anastomosis of nonviable small intestine and Lichtenstein's tension-free repair. However, patients with either frank pus or fecal matter within the sac and/or evidence of generalized peritonitis were excluded from their study. 12 Since the open approach was used in all of these cases, we would like to conduct a study of laparoscopic prosthetic herniorrhaphy with bowel resection.
We confirmed the viability of the incarcerated bowel by the improved color tone and presence of peristaltic movements during the operation. However, there may have been cases of unnecessary bowel resection. Recently, the usefulness of indocyanine green fluorescence for assessing intestinal blood flow has been reported.13,14
The water pressure method is the gentlest technique available for reduction of incarcerated inguinal, femoral, and obturator hernias. In our series, we demonstrated that all the cases of incarcerated hernia were treated by the water pressure method. When the entire circumference of the bowel was incarcerated/strangulated in the hernia orifice, the water pressure method was not effective, even if saline was injected into the hernia sac, which merely bulged. All the cases in which successful reduction was accomplished by the water pressure technique were cases of Richter's hernia, and there was no necessity for bowel resection in any of the cases.
Even in cases in which external manual reduction was possible, intra-abdominal observation was performed as soon as possible, to detect any bowel necrosis or reduction en masse. “Reduction en masse of inguinal hernia” means reduction/migration of the hernia sac as well into the preperitoneal space, likely produced by forcible attempts at reduction, in which reduction of the hernia sac occurs together with its intestinal contents, so that the bowel still remains incarcerated.15–18 There was 1 case of reduction en masse of inguinal hernia and bowel necrosis in this study. If intra-abdominal observation cannot be performed as soon as possible after external manual reduction, CT becomes necessary.
We had two bladder injuries in the open approach, whereas no serious intraoperative complications in the laparoscopic approach. In some reports, the intraoperative complication rate of the laparoscopic herniorrhaphy was equivalent to the open herniorrhaphy.19–21 However, according to a meta-analysis of primary unilateral inguinal hernia, there was a significant difference in the intraoperative complications between the laparoscopic group and the open group. There was a high intraoperative complication rate in laparoscopic group, especially TAPP procedure. 22 Fortunately, in our series, there was no serious intraoperative complication in the laparoscopic group. All laparoscopic series had been performed under the same expert laparoscopic surgeon.
The overall mortality rate was 1.9% in our case series, which is consistent with previous reports.23–26 Especially, in patients with obturator hernias, delay of subsequent treatment can result in high morbidity and mortality rates.27–30 There was no case of death in our cases treated by the laparoscopic approach. In cases of ileus with prominent bowel dilatation, there is no time for decompression and emergency surgery is required. In previous reports, there was no definite laparoscopic protocol for cases with bowel dilatation. In our study, although our protocol mainly consisted of the TAPP approach, we found that with the introduction of the TEP approach laparoscopic reduction could be accomplished even in cases of bowel dilatation. We have demonstrated one clinical protocol for the treatment of incarcerated/strangulated groin and obturator hernias in this study.
Conclusions
The laparoscopic approach for acutely incarcerated/strangulated hernia was not associated with any mortality. The procedure from reduction to herniorrhaphy was accomplished by the laparoscopic approach in most cases. Moreover, the laparoscopic reduction could be performed safely, with the approach affording adequate visualization of the incarcerated bowel. Therefore, laparoscopic reduction and herniorrhaphy for acutely incarcerated/strangulated groin and obturator hernias are effective, safe, and feasible.
Footnotes
Acknowledgments
The authors thank the nursing and anesthesia staff at Nippon medical school, Musashikosugi hospital.
Disclosure Statement
No competing financial interests exist.