
Abstract
Abstract
Background:
This prospective cohort study is aimed to compare the efficacy and safety of three-dimensional (3D) versus two-dimensional (2D) laparoscopy in laparoscopic-assisted transanal pull-through (LATP) for the surgical treatment of Hirschsprung's disease (HD) in children.
Methods:
This study enrolled 80 children who were histologically diagnosed with HD and undergone LATP performed by a single experienced surgeon at our department between January 2015 and November 2017. Children were randomized to receive 2D laparoscopy (n = 40) or 3D laparoscopy (n = 40). Data on patient characteristics, operative parameters, and the surgeon's assessment on utilization of laparoscopic system were prospectively recorded and analyzed.
Results:
Patient characteristics, including age at surgery, gender, weight, and the level of aganglionosis, were comparable between the two groups (each P > .05). Compared with 2D imaging system, 3D system significantly shortened the performance time of laparoscopic phase (27.0 ± 3.6 minutes versus 38.3 ± 4.3 minutes, P < .001) with a 29.5% reduction, and the total time of the entire surgery (106.0 ± 19.5 minutes versus 122.1 ± 18.7 minutes, P < .001). No statistical difference was observed in terms of estimated intraoperative blood loss and intraoperative laparoscopic complications between the two groups (each P > .05). In addition, 3D system significantly improved depth perception and precision, and reduced surgical strain for the surgeon.
Conclusions:
3D LATP is feasible and safe in the surgical treatment of HD in children. Further studies are still needed to investigate the application of 3D in both experienced and inexperienced surgeons.
Introduction
Hirschsprung's disease (HD) is one of the most common congenital malformations, which is characterized by the absence of ganglion cells in the submucosal (Meissner's) and myenteric plexus along a variable length of the intestine. 1
Since Georgeson et al. 2 first described the conventional laparoscopic-assisted transanal pull-through (LATP) in 1995, LATP, as a minimal access technique, has gained extensive acceptance in surgical treatment of HD.3–5 Previous studies have demonstrated that laparoscopic-assisted approaches have significant advantages over open laparotomy in children suffering from HD, such as minimizing surgical trauma, accelerating postoperative recovery, shortening the length of hospital stay, and decreasing postoperative complications.3,6 Compared with the totally transanal approach, laparoscopy provides macroscopic view of the transition zone, allows early intraoperative biopsy, and decreases the risk of colonic torsion.5,7,8
Conventional laparoscopy relies on two-dimensional (2D) imaging system. The lack of stereoscopic vision in 2D system could result in impaired depth perception and spatial orientation. 9 Compared with open surgery, surgeons who operate in three-dimensional (3D) space but are guided by 2D vision have to transfer 2D representation of the anatomical structures to real and stereoscopic anatomy, and thus experience a higher visual and cognitive load.9–11 These limitations of 2D system pose considerable challenges for surgeons, particularly for surgical novices, increase the difficulty of laparoscopic performance, and hence could make laparoscopic operations more difficult to master. 12
With the development of laparoscopic technology, 3D vision system has been introduced to overcome the shortcomings of 2D. 13 Multiple comparative studies have demonstrated that 3D vision significantly improves depth perception and spatial orientation during surgery, and has obvious advantages over 2D.14,15 Although inconsistent results are observed among previous studies,13,16,17 significant heterogeneity exists in terms of task types, outcome measures, individual stereoacuity, applied equipment and other factors, and thus conclusions should be drawn carefully. Of note, the most recent 3D vision system offers superior quality of images and stereoscopic vision for surgeons, and has been recommended as a safe and feasible alternative for conventional 2D system.10,18,19
Although 3D system has been investigated gradually in various forms of operations in adults, researches on 3D vision system in pediatric surgery are still scarce. To our knowledge, to date there is no study comparing the application of 3D versus 2D system in the management of HD. The intention of this prospective cohort study was to compare the efficacy and safety of 3D and 2D imaging system for LATP in children diagnosed with HD in terms of surgical aspects.
Patients and Methods
Study design and patients
This prospective cohort study was designed to recruit children who were histologically diagnosed with HD and undergone LATP performed by the same surgeon from January 2015 to November 2017 in our center. This study was approved by the Institution Review Board of Huai'an Women and Children's Hospital.
Children were eligible if they were diagnosed with HD preoperatively based on clinical symptoms, barium enema, rectoanal inhibitory reflex, and preoperative rectal biopsy. Before assignment, patients or legal guardians of each child were informed of both surgical procedures and provided written consent. Children were excluded if their parents or legal guardians rejected participation or surgical treatment of HD.
On the day of surgery, all children enrolled were randomized into 2D group or 3D group at a 1:1 ratio. Assignments were based on computer-generated randomizations that were kept in sealed, sequentially numbered envelopes until used. The histological diagnosis of HD was confirmed by intraoperative frozen biopsy and postoperative histopathology of the resected specimen. All children were given the same protocols of preoperative preparation and postoperative management.
Surgical procedures
All operations were performed by a single senior surgeon who had accumulated extensive experience on laparoscopic surgery and mastered the key points of both 2D and 3D LATP to attenuate the effect of learning curve. Meanwhile, the senior surgeon was assisted by an attending surgeon who acted as assistant and a resident surgeon who acted as camera operator.
Conventional 2D laparoscopic surgery was performed with the Karl Storz 2D-HD vision system, whereas 3D laparoscopic surgery was performed with the Karl Storz 3D-HD vision system. The 3D monitor was also placed at the foot of the operating table. Unlike 2D laparoscope capturing a single image at a time, the 3D laparoscope had two image sensors inside, and could capture two respective images by each sensor. Signals of the two images were processed and then synchronized on the 3D monitor, which subsequently created stereoscopic visualization for surgeons wearing passive polarizing glasses during laparoscopic procedures. Except for laparoscopic vision systems, other surgical instruments were identical between the two groups.
Surgical principles and procedures in the 2D and 3D groups were identical and standard, including two phases: the laparoscopic phase and the transanal phase. The surgical details of LATP have been described by previous publications. 20 General anesthesia was given by means of tracheal intubation. The patient was placed on the operating table in a supine position. The monitor was placed on the feet side of the operating table. Three trocars were positioned for LATP. First, a trocar for the laparoscope was inserted through an umbilical skin incision, and carbon dioxide pneumoperitoneum with a pressure of 8–10 mmHg was established. Then, the second and third trocars were inserted, respectively, at the right lower and upper side of the abdomen just lateral to the edge of the rectus abdominis muscle. In some cases, an extra trocar could be placed at the left upper quadrant to facilitate the operation if required.
After the insertion of the laparoscopic instruments, the abdominal cavity was inspected to estimate the extent of the involved intestine under 3D or 2D visualization. Intraoperative frozen biopsies of tissue specimens obtained from the narrowed and the dilated segment proximal to the macroscopic transition zone were performed routinely to confirm the diagnosis of HD and the level of the transitional zone, respectively (Fig. 1). The colonic mesentery and its relative vessels were dissected with the assistance of an ultrasound scalpel, and the marginal arcade was preserved. The colon was mobilized to adequate length so that it could be pulled out through anus without tension (Fig. 2).

Colonic seromuscular biopsy using 3D laparoscopic system: two respective images synchronously captured by two sensors in the 3D laparoscope. 3D, three-dimensional.
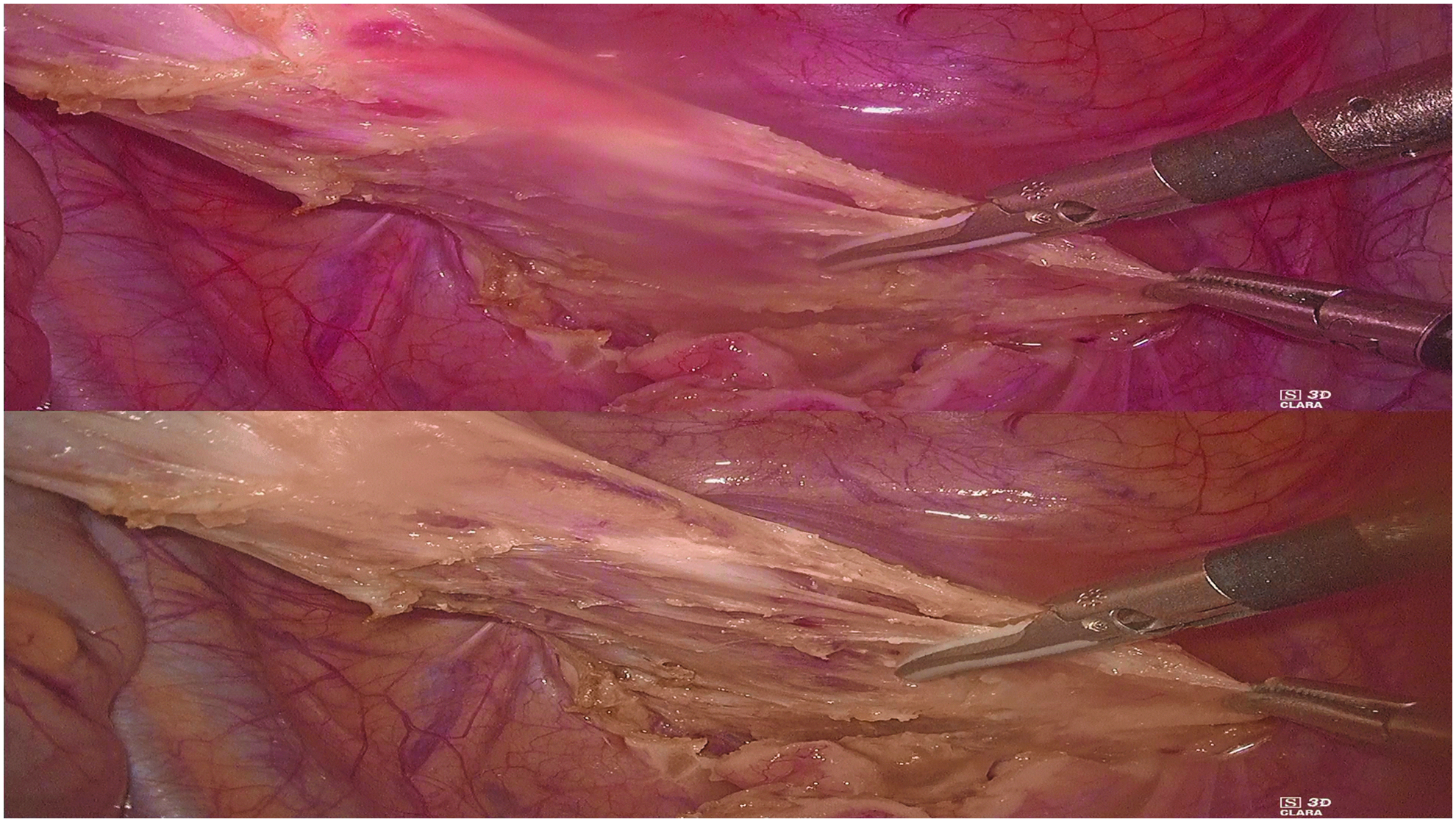
Mobilization of the aganglionic bowel using 3D laparoscopic system: two respective images synchronously captured by two sensors in the 3D laparoscope. 3D, three-dimensional.
At the beginning of transanal phase, eight traction sutures were performed to fully expose the anus. Endorectal mucosectomy was started at the proximal to the dentate line and continued upward until the rectum and colon are completely free. The part of rectal muscularis below the peritoneal was resected posteriorly. After the mobilized bowel segment was pulled out and resected, coloanal anastomosis was performed with 5–0 absorbable sutures.
Data collection
Data were prospectively recorded and collected, including patient characteristics (age at surgery, gender, weight, and the level of aganglionosis), and operative parameters (conversion to open surgery, performance time of laparoscopic phase, the total time of the entire surgery, estimated intraoperative blood loss during laparoscopic phase and the entire surgery, respectively, intraoperative laparoscopic complications, and the length of postoperative hospital stay).
To investigate whether the advantages or disadvantages of 3D laparoscopic system transfer into significant effect on subjective experience of surgeons, we designed a standard questionnaire regarding utilization of 2D or 3D imaging system for LATP with a five-point Likert-type rating scale, which was similar to those applied in several recent studies,14,21,22 before the onset of this study.
The surgeon was asked to answer the questionnaire immediately after completing each laparoscopic operation. The scores were graded as poor (score 1), fair (score 2), good (score 3), very good (score 4), and excellent (score 5) for depth perception and precision, and graded as no symptom (score 1), slight (score 2), moderate (score 3), severe (score 4), and extreme (score 5) for surgical strain (eye strain, wrist and hand strain, neck strain, as well as back strain), as well as potential adverse effects (dizziness, headache, and nausea). In addition, the surgeon could register any other symptoms that were encountered during LATP but not mentioned in the questionnaire.
Statistical analysis
All data were analyzed using Stata 12.0 software. Quantitative variables were expressed as mean ± standard deviation, or as median with range. Categorical variables were expressed as numbers and percentages (%). The independent sample t-test or the Mann–Whitney U test was used for comparison of quantitative variables as appropriate. The chi-square test or Fisher's exact test was used for categorical variables as appropriate. A two-sided P value <.05 was considered statistically significant.
Results
Patient characteristics
Figure 3 shows the flowchart of this study. A total of 80 patients were eligible for analysis, with 40 cases in the 3D group and 40 cases in the 2D group. Table 1 summarizes the baseline characteristics of all children in the two groups. There were no statistical differences in terms of age at surgery (P = .389), gender (P = .356), weight (P = .992), as well as the level of aganglionosis (P = .615), respectively.
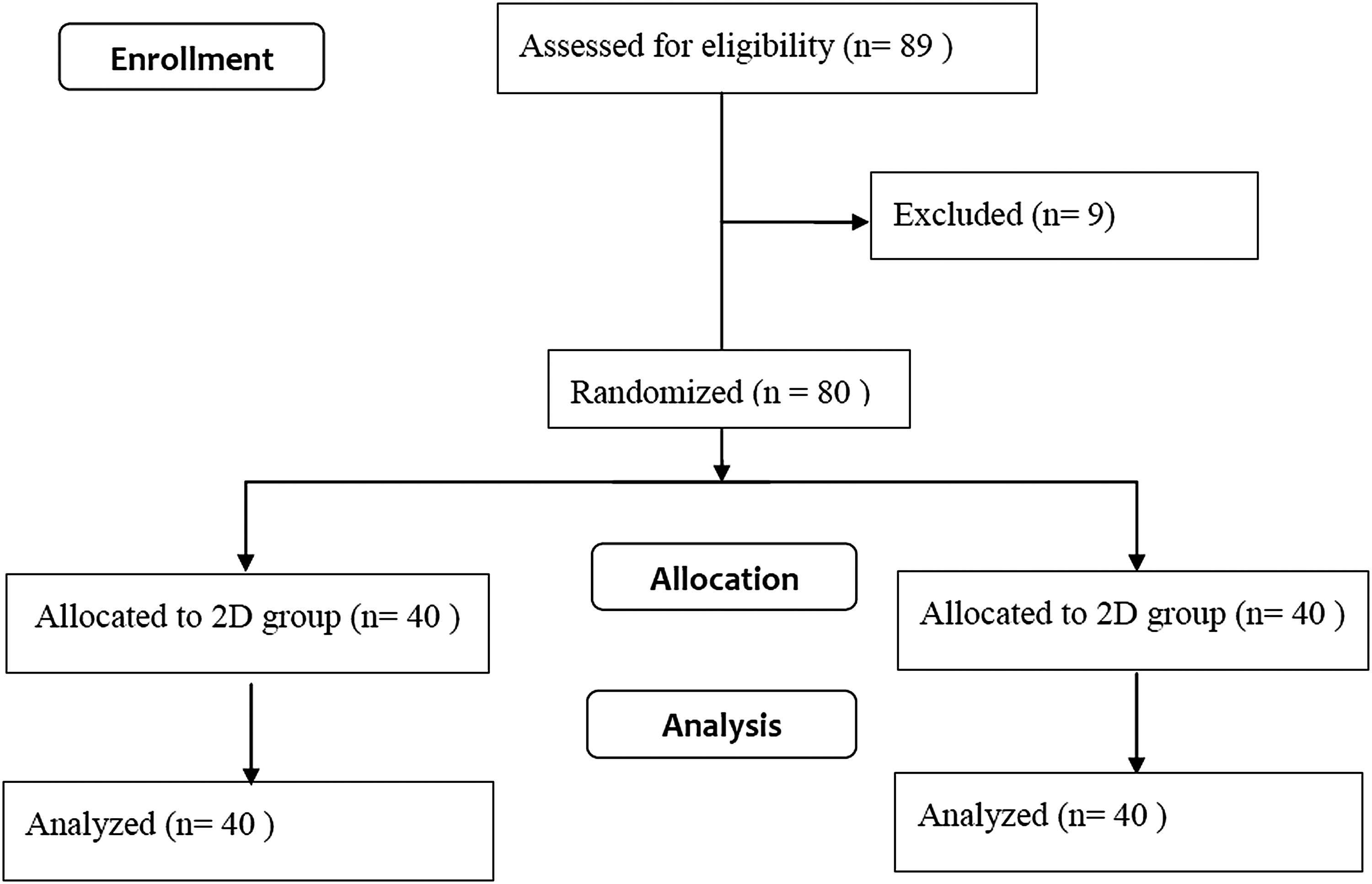
Flowchart of this study in accordance with the CONSORT statement.
Patient Characteristics
2D, two-dimensional; 3D, three-dimensional.
Operative parameters
As displayed in Table 2, LATP was completed successfully in all children, without conversion to laparotomy. The performance time taken for laparoscopic phase was 27.0 ± 3.6 minutes (range: 16–35 minutes) in the 3D group and 38.3 ± 4.3 minutes (range: 28–46 minutes) in the 2D group. Compared with 2D, 3D vision system significantly shortened the performance time for laparoscopic procedures (P < .001), which produced a 29.5% reduction, and thus shortened the total time taken for the entire surgery (P < .001). Moreover, no statistical difference was observed in terms of the estimated intraoperative blood loss during laparoscopic phase (P = .706), or the entire surgery (P = .826). Ureter injury occurred in 1 patient undergoing 2D laparoscopy. There was no statistical difference in the rates of intraoperative complications due to laparoscopic errors between the two groups.
Operative Parameters
Ureter injury occurred in 1 patient undergoing 2D laparoscopy.
2D, two-dimensional; 3D, three-dimensional.
Parameters of the questionnaire
Table 3 gives the surgeon's assessment regarding utilization of 3D or 2D system for LATP. The surgeon reported better depth perception (P < .001) and precision (P < .001) under 3D vision rather than 2D. Besides, surgical strain was reduced with utilization of 3D system, including wrist and hand strain (P < .001), as well as neck strain (P < .001). The surgeon did not report any adverse effects especially attributed to the utilization of 3D system when performing LATP, except slight dizziness in 2 cases. There is no statistical difference in terms of the scores of dizziness (P = .155), headache (P = 1.000), and nausea (P = 1.000) between the two groups.
Parameters of the Questionnaire Regarding Utilization of Three-Dimensional and Two-Dimensional System for Laparoscopic-Assisted Transanal Pull-Through by the Surgeon with a 1–5 Rating Scale
Score 1–5: 1 = poor; 5 = excellent.
Score 1–5: 1 = no strain; 5 = extreme.
Score 1–5: 1 = no symptom; 5 = extreme.
2D, two-dimensional; 3D, three-dimensional; SD, standard deviation.
Discussion
With the development of laparoscopic technology, 3D vision system has been introduced to overcome the shortcomings of 2D.12,19 However, it is still unclear whether the 3D imaging system is superior to conventional 2D system in surgical management of HD. This cohort study demonstrated that 3D imaging system shortened the performance time of laparoscopic phase and the total time of the entire surgery for LATP compared with 2D system. Of note, the surgeon experienced significantly better depth perception and surgical precision, and reported less surgical strain when using 3D system instead of 2D system.
Compared with 2D system, high-quality stereoscopic images provided by 3D system allow surgeons experience as good depth and spatial perception as in the open surgery. 23 The improvement of depth perception and spatial location could enhance the sense of anatomical structures and hand-eye coordination for surgeons, and thus reduce the difficulty of laparoscopic surgery, especially those complex manipulations demanding high degree of accuracy and dexterity.11,19,21 Under 3D vision, laparoscopic manipulations, such as dissection, suturing, the tying of knots, and object transferring, are more easier.19,24 Visual misperception is one of the leading causes of laparoscopic injuries. 9 3D vision could provide stereoscopic vision of the operating field and increase the accuracy of laparoscopic performance, and thus decrease the possibilities of surgical damage to surrounding vessels, nerves, organs, and tissues.9,11
Multiple studies have demonstrated the advantages of 3D over 2D in both clinical and simulated settings. In simulated tasks, the performance time, the number of repetitions, and the number of errors are significantly reduced by the application of 3D system compared with 2D.10,14,15,24 Feng et al. reported that even in rather small and restricted spaces in which the laparoscope was placed very close to the operative field, depth perception could also be improved by 3D vision. 14 In laparoscopic operations, the advantages of 3D system compared with 2D system mainly manifest as shorter operative time, less surgical complications, and less intraoperative blood loss.11,21,23 Furthermore, several studies reported better subjective experience of surgeons for 3D visualization, such as less surgical strain, and personal preference for 3D laparoscopic system.21,25,26
In our center, the adoption of 3D laparoscopic system was first practiced in LATP. During LATP, 3D system could provide stereoscopic visualization of the operating field, and facilitate our understanding of the anatomical relationships compared with 2D system. As far as we are concerned, the technical advantages of 3D laparoscopic system in LATP mainly manifested as the following several aspects. First, seromuscular colonic biopsy and mobilization of the aganglionic bowel were performed more easily and quickly under 3D visualization. Second, with better understanding of spatial distribution of mesenteric vascular branching, surgeons could dissect colonic mesentery and handle relative mesenteric vessels more accurately and properly, and thus avoid accidental damage to vessels. Third, 3D visualization improved depth perception in the pelvic cavity and reduced the risk of laparoscopic injury to pelvic nerves and vessels, and to the prostate, urethra, or other pelvic organs.11,27
Of note, stereoscopic vision of the pelvis, particularly those structures in the deep pelvic cavity, allows more accurate identification of pelvic anatomy, and thus aids in preventing intraoperative bleeding or injuries to adjacent organs. Furthermore, the technical difficulty of mobilizing the aganglionic bowel in the pelvic cavity, which was the most complex technique and the key speed-limiting step in LATP according to our experience, was also significantly decreased under 3D visualization, since 3D laparoscopic system provided great convenience for laparoscopic manipulations in the pelvic cavity. In comparison, mobilizing in the abdominal cavity was technically easier. Hence, the level of aganglionosis could affect the operative speed of LATP, but its significance was relatively minor. In our opinion, advantageous mobilization of the aganglionic bowel may be a major factor to shorten operative time of LAPT.
According to previous studies, there are a number of undesirable effects of 3D system on its users, such as headache, dizziness, and nausea.14,16,17 Nevertheless, recent studies demonstrated that these adverse effects appeared to be mainly correlated with the inferior image resolution of the earlier 3D system.10,13 Zdichavsky et al. reported that visual fatigue during 3D laparoscopic procedures occurred more frequently in children than adults. 28
In our case series, the surgeon did not report any discomfort especially due to the 3D vision itself, which were experienced occasionally at the initial stage of learning curve, except slight dizziness in 2 cases with relatively longer duration of performance time than the other cases in the 3D cohort. We infer that this may be partially explained by that surgeons could adapt well to the 3D environment after the initial learning period. In fact, the 3D laparoscope could be held relatively steady during surgery, whereas 2D laparoscope has to be moved constantly to achieve indirect depth cues, such as movement parallax.15,28 Therefore, surgeons may feel more comfortable when viewing a steady screen in 3D settings instead of a constantly moving picture displayed by 2D monitor, particularly in long and complex operations, which may promote surgeons tend to choose 3D when performing LATP.
In this study, the aforementioned advantages of 3D system translated into shortening the performance time taken for laparoscopic phase and for the entire surgery (Table 2), enhancing depth perception and surgical precision, and relieving surgical strain, as expected (Table 3). Lower technical complexity and shorter OT represented less workload with the use of 3D system to some degree, and potentially explained the less surgical strain in the 3D group. In addition, comparative analysis of postoperative hospital stay and the total cost revealed no statistical difference between the two groups (data not shown).
However, there are several aspects worthy of note when definitive conclusions were drawn. A few studies found that technical level of surgeons and the types of procedures affected the magnitude of surgical improvement,14,22,26,29 and experienced surgeons were observed to benefit relatively less than inexperienced surgeons when using 3D laparoscopy.22,29 During LATP, the reduction in performance time was 29.5% for laparoscopic phase, whereas it translated into only 13.2% for the entire surgery. Besides, only one intraoperative complication (ureter injury) occurred, and the rates of intraoperative complications did not show statistical difference in this study. To experienced surgeons, the use of 3D laparoscopy in LATP appeared to manifest its advantages mainly on its operators, with significantly improved depth perception and surgical precision, and relieved surgical strain.
It is unclear whether rich experience of the surgeon on laparoscopic operations hindered more superior results of 3D LATP in this study. More studies are required to further investigate the application of 3D and 2D LATP in both experienced and inexperienced surgeons, and in other types of pediatric operations. Nevertheless, we believe that more realistic vision of pelvic structures and the operative field with utilization of 3D system may be of great value for inexperienced surgeons, particularly novices,11,27 and ease their mental stress and anxiety due to potential technical errors during LATP. This hypothesis is yet to be proved by further researches.
There are several limitations in this study. First, 2D laparoscopic system was introduced earlier than the 3D system in our center. Thus, the surgeon who performed LATP for all children enrolled had accumulated more surgical experience on 2D laparoscopy than 3D before the onset of this study, which might lead to an underestimation on the advantages of 3D laparoscopy. Second, considering technical safety, 3D LATP, as a new technique, was initially practiced in experienced surgeons who have mastered 2D LATP. Herein, we did not investigate its application in inexperienced surgeons. It needs to be further investigated whether 3D LATP has more significant advantages in inexperienced surgeons and a shorter learning curve than 2D LATP.19,26 Furthermore, the sample size of this study may be not large enough to determine the differences in intraoperative complications between 3D and 2D imaging systems, and more studies with larger sample size are required to confirm our results.
Despite these limitations, to our knowledge, this is the first comparative study on 3D versus 2D laparoscopic system in LATP, and it may provide valuable clues and insights for surgeons when investigating the application of 3D laparoscopy in pediatric surgery.
In conclusion, compared with conventional 2D system, this study provides evidence that 3D laparoscopic system could shorten the performance time, improve depth perception, and reduce surgical strain when surgeons perform LATP, and has no significant association with intraoperative complications in an experienced surgeon. These findings support that 3D system is a feasible and safe alternative to 2D system for the surgical treatment of HD in children. However, more studies are needed to further validate the application of 3D in pediatric surgery.
Footnotes
Acknowledgments
This study was sponsored by the Key Research and Development Plan Project (Social Development) of Huai'an City (HAS201615) and the Maternal and Child Health Research Project of Jiangsu Province (F201713).
Disclosure Statement
No competing financial interests exist.