
Abstract
Abstract
Background:
This study aimed to evaluate single-port laparoscopic appendectomy (SPLA) in comparison with three-port laparoscopic appendectomy (3PLA) in children about the extent of surgical trauma after SPLA and 3PLA measured by serum interleukin-6 (IL-6) and C-reactive protein (CRP) concentrations.
Materials and Methods:
A total of 50 patients with a median age of 11.5 were randomized to two groups. Experts in both methods performed the surgeries. The decision on the type of planned surgery was randomly determined. Serum IL-6 and CRP levels were measured using an enzyme-linked immunosorbent assay before, and at 12 and 36 hours after surgery. Furthermore, we compared operating time, hospital stay, postoperative pain, and complication rates.
Results:
The operative time in the 3PLA group was shorter than that in the SPLA group (P < .05). Preoperative IL-6 levels were not different between the two groups, but the rise (pre- versus postoperative) of IL-6 in the SPLA group was remarkably higher when compared with the 3PLA group (P < .05). Similar results were obtained for CRP; basal serum CRP levels were not different between the two groups, but the rise of CRP in the 3PLA group was significantly lower compared with that in the SPLA group. During the first 12 hours postoperative, the SPLA patients reported more severe postoperative pain and longer inpatient opiate usage was noted that after 3-PLA. Only one SPLA case was converted to 3PLA. There were no conversions to open surgery. The length of hospital stay and complication rate were not different between the two groups.
Conclusions:
SPLA in children is associated with longer operative times, increased pain level, and more severe surgical trauma as measured by postoperative CRP and IL-6 levels in comparison with a 3PLA. The two approaches were comparable regarding the length of hospital stay and complication rate.
Introduction
Each surgical intervention causes an injury to tissues. Such a trauma induces hormonal, metabolic, immunological, and hemodynamic disturbances. Depending on the extent of the surgery varying degree of hypermetabolic and catabolic reactions occur, which are often aggravated by the underlying disease. Increased protein degradation, hyperglycemia, and insulin resistance hinder the healing process. Surgical stress also affects cytokine synthesis, which can cause transient immunosuppression. 1 Several authors consider especially interleukin-6 (IL-6) to be an exponent of the severity of the surgical stress that correlates with blood loss, duration of the surgery, and overall surgical trauma intensity.2–4 The highest levels of this cytokine are noted between 3 and 24 hours postoperative. 5 Therefore, perioperative immunological changes facilitate wound infections and stimulate inflammatory processes.
Appendectomy is the most commonly performed abdominal surgical procedure in the acute settings in pediatric surgery. Since 1894, when Mc Burney described the first open appendectomy, new approaches have emerged in this field, 6 mainly to minimize the tissue damage to promote “scarless surgery” idea. 7 The techniques in use today are as follows: three-port laparoscopic appendectomy (3PLA), transumbilical laparoscopic-assisted appendectomy 8 (TULAA), and single-port laparoscopic appendectomy (SPLA). Various rules of conduct can be found utilizing the three approaches. The proposed benefits of this type of treatment include earlier return to regular activity, better aesthetic results, fewer complications and, above all, less severe operative stress. There are relatively few studies comparing and proving lesser surgical stress during laparoscopic appendectomy compared with an open appendectomy,5,9–12 of which a study by Almagor et al. 5 is a noteworthy example, but little is known about the effects of SPLA versus standard 3PLA. Moreover, there is a need for studies comparing endoscopic-only surgeries because of different physiological responses linked to pneumoperitoneum with carbon dioxide (CO2) and patient positioning as it was thoroughly described by Ure et al. 13 Therefore, we conducted a study comparing the effects and efficacy of conventional 3PLA and SPLA in children with an emphasis on surgical tissue damage.
Materials and Methods
The null hypothesis of the study is that there is no difference in the extent of the tissue injury between 3PLA and SPLA. An alternative hypothesis is that SPLA causes greater tissue injury than 3PLA. The primary outcome is the IL-6 and C-reactive protein (CRP) serum concentration of 12 and 36 hours after surgery. The secondary outcome measures are the duration of surgery, length of stay, postoperative pain intensity, and early complications.
To test this hypothesis a total of 50 children (29 boys and 21 girls) with a median age of 11.5 (range 4–17 years) were included in the study. The clinical diagnosis of acute appendicitis was made by radiological signs (ultrasound examination) and laboratory tests (complete blood count and CRP levels). Patients with all stages of appendicitis were included in the study, apart from an inflammatory tumor and periappendiceal abscess (Table 1). Patients <2 and >18 years of age and those who had had previous abdominal surgery were excluded from the study. Also, patients with additional active accompanying disease processes were excluded from the study (2 patients—type 1 diabetes patient and a patient with the previous laparoscopy for undescended testis).
Stages of Appendicitis
Patients were randomized utilizing the random number generator. 14 Patients attributed even numbers underwent 3PLA and attributed odd numbers underwent SPLA. The randomization took place after qualification for surgery and after signing by parents/legal guardians a proper informed consent. The study was approved by a local ethical committee of the Medical University of Gdansk.
During 3PLA, patients were placed in the supine position and given general anesthesia. An orogastric tube was placed in each case. Unless the patient had just voided, a Foley catheter was placed in the bladder. The left arm was tucked and the abdomen shaved as necessary. The umbilical skin was anesthetized with 2% lidocaine and 0.5% bupivacaine mixture in 1:1 ratio (LiB). A 1.5 cm vertical or transverse skin incision was made within the umbilical stalk, the fascia was retracted, and a 1.5 cm vertical fascial incision was made with a scalpel. A 5 mm port was placed in an open manner (according to Hasson technique) through the fascia and the abdomen insufflated with CO2 gas. Diagnostic laparoscopy was then performed, and internal organs, including the stomach, liver, gallbladder, colon, small intestines, and pelvis, were inspected. If a diagnosis other than acute appendicitis was made, the patient was excluded from the study and treated appropriately. If the appendix looked normal and no other pathology was found in the abdomen, the patient remained enrolled in the study providing the surgeon decided to remove the appendix. Additional 5 mm ports were placed in the left lower quadrant and suprapubic midline after the skin and peritoneum were anesthetized with LiB. A 5 mm camera was transferred to the left lower quadrant port site, and the appendix was exposed and retracted anteriorly. The mesoappendix was divided with monopolar cautery. The base of the appendix was ligated with Endoloop™. The appendix was removed through the umbilical incision after first placing it into the trocar lumen. Only minimal irrigation of the peritoneal cavity was used. Perforated appendix cases were treated with suctioning of intra-abdominal pus and prolonged postoperative intravenous antibiotics course. Umbilical incision length was measured in millimeters, and then closed with Maxon absorbable suture. All skin edges were reapproximated with 4-0 suture.
During SPLA, patients were positioned similarly as in 3PLA. The base of the umbilical stalk was everted by two penetrating towel clamps placed either side of the midline. A vertical skin incision was made within the umbilical stalk, the fascia was retracted, and a 3 cm vertical fascial incision was made with a scalpel. The incision was retracted anteriorly, and the SILSPort™ was inserted into the incision using a shoehorn maneuver (Fig. 1). Five-millimeter trocars were placed in the SILSPort, and the abdomen insufflated with CO2 gas, after which the trocars were repositioned into a staggered elevation.

Shoehorn maneuver used to introduce the SILSPort™ into the incision.
With the induction of anesthesia, all patients were given antibiotics (a single dose of intravenous cefazoline). The dose was adjusted according to the weight of the patients. The antibiotic treatment was continued after surgery (amoxicillin and clavulanic acid) and modified according to the stage of the disease. The operating time, hospital stay, and perioperative complications were recorded. The operating time was measured from the incision to placement of the last suture. The discharge was decided by the surgeon based on body temperature, white blood cells count, incision, and overall clinical condition of the patient.
Blood samples were collected at the beginning of the surgery, and at 12 and 36 hours after surgery. Blood samples were stored at −86°C. IL-6 and CRP concentrations were measured by enzyme-linked immunosorbent assay (ELISA) using commercially available ELISA kits and Flow Cytometry Human Cytokine kit according to the manufacturer's instructions.
We also analyzed conventional parameters—duration of surgery, length of stay, postoperative pain (incorporating the visual analog scale—see Fig. 2) intensity, and early complications, namely wound dehiscence, wound infection, and suppuration, the formation of intra-abdominal abscesses and late complications, and adhesion formation leading to intestinal obstruction at a monthly follow-up.

The visual analog scale used to determine pain felt by the patient.
The statistical differences were analyzed using an adaptation of Student's t-test, Welch's unequal variances t-test. A statistical difference was assumed in all cases when the P-value was <.05. The differences in the complication rates were estimated using the chi-squared test and Fisher's exact test.
After the minimal sample size calculation was done on the basis of the previous studies, 15 we decided to enroll 50 patients to obtain equinumerous groups of patients and a two-sided α value of 5% with a power of 95%.
Results
Collected data were divided into two groups—3PLA and SPLA—based on the intention-to-treat concept. Patients' characteristics are provided in Table 2. The groups are homogenous, and there are no statistical differences between the groups. Also, the appendicitis staging did not differ between the groups. All enrolled patients completed the study.
Characteristics of the Patients Participating in Single-Port Laparoscopic Appendectomy Versus Three-Port Laparoscopic Appendectomy Study
3PLA, three-port laparoscopic appendectomy; SPLA, single-port laparoscopic appendectomy.
Table 3 shows the conventional parameters. SPLA took longer time than 3PLA procedures (70 minutes versus 60 minutes; P < .05) statistically. In contrast, there was no difference in the duration of hospital stay. Also, the subjectively perceived pain was more significant after SPLA (mean value—5 points (pts); ranging from 2 to 9 pts) than after 3PLA (mean value—3 pts; ranging from 1 to 7 pts) as measured with visual analog scale. Two postoperative wound infections occurred in the SPLA group, and one intra-abdominal abscess formation was noted in 3PLA group.
Results of Surgical and Hospital Stay Parameters of Patient Groups Single-Port Laparoscopic Appendectomy and Three-Port Laparoscopic Appendectomy Participating in Single-Port Laparoscopic Appendectomy Versus Three-Port Laparoscopic Appendectomy Study
Bold fonts present statistically significant data.
3PLA, three-port laparoscopic appendectomy; pts, points; SPLA, single-port laparoscopic appendectomy.
One conversion from SPLA to 3PLA was noted. The reason for the conversion was a retrocecal appendix difficult to dissect with the use of articulating instruments.
Table 4 presents the results of laboratory tests. There were no differences found between the groups in CRP and Il-6 levels before surgery. In contrast, results clearly show that both the CRP levels and Il-6 levels after surgery were higher in SPLA group than in 3PLA group. The difference is depicted in Figures 3–6. Table 5 shows average changes in the levels of CRP and IL-6. The statistical difference is seen in both cases. CRP levels were the highest 36 hours after surgery, whereas IL-6 levels were the highest 12 hours after surgery.
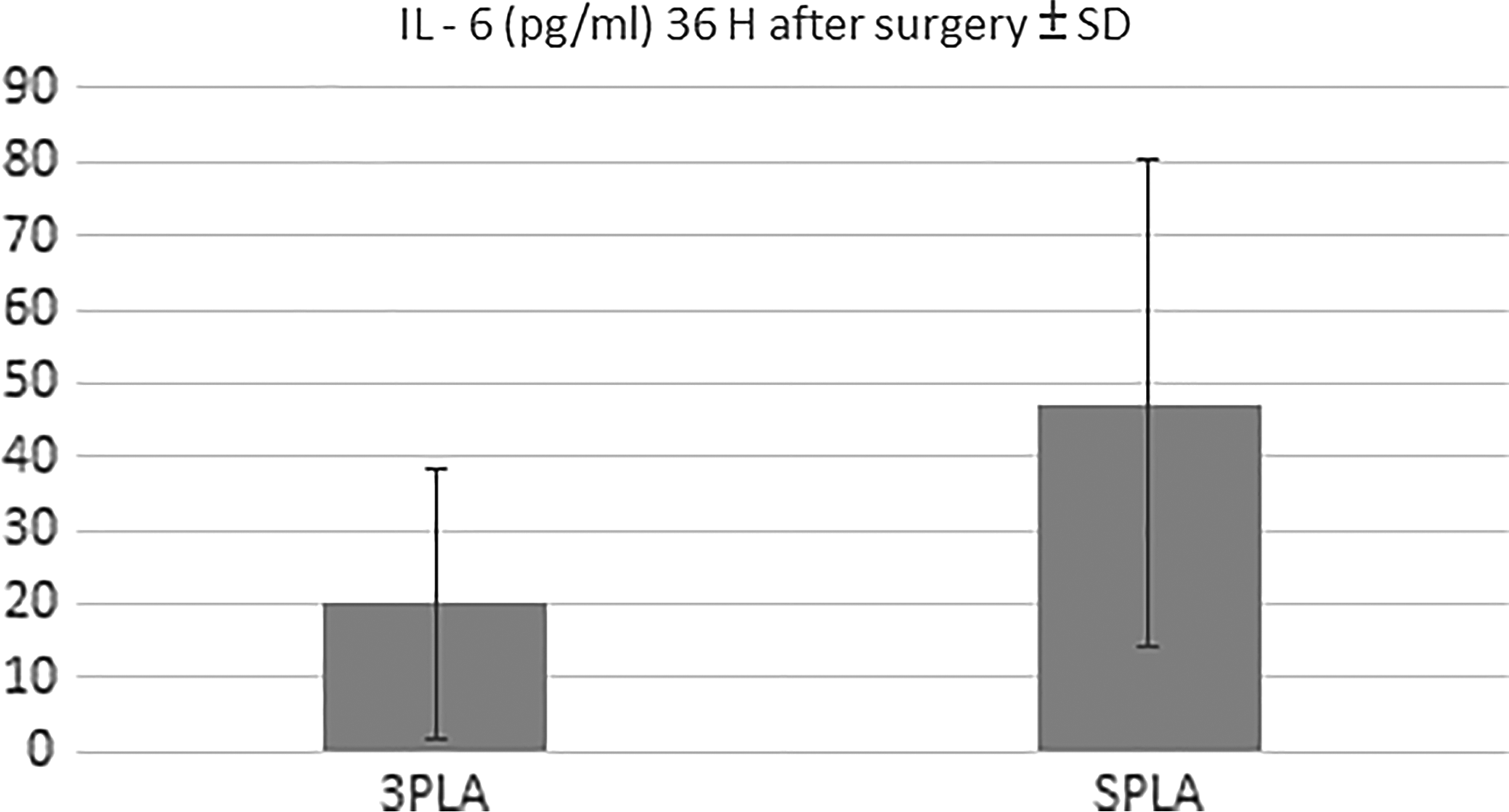
IL-6 levels 36 hours after surgery in two groups. IL-6, interleukin-6.
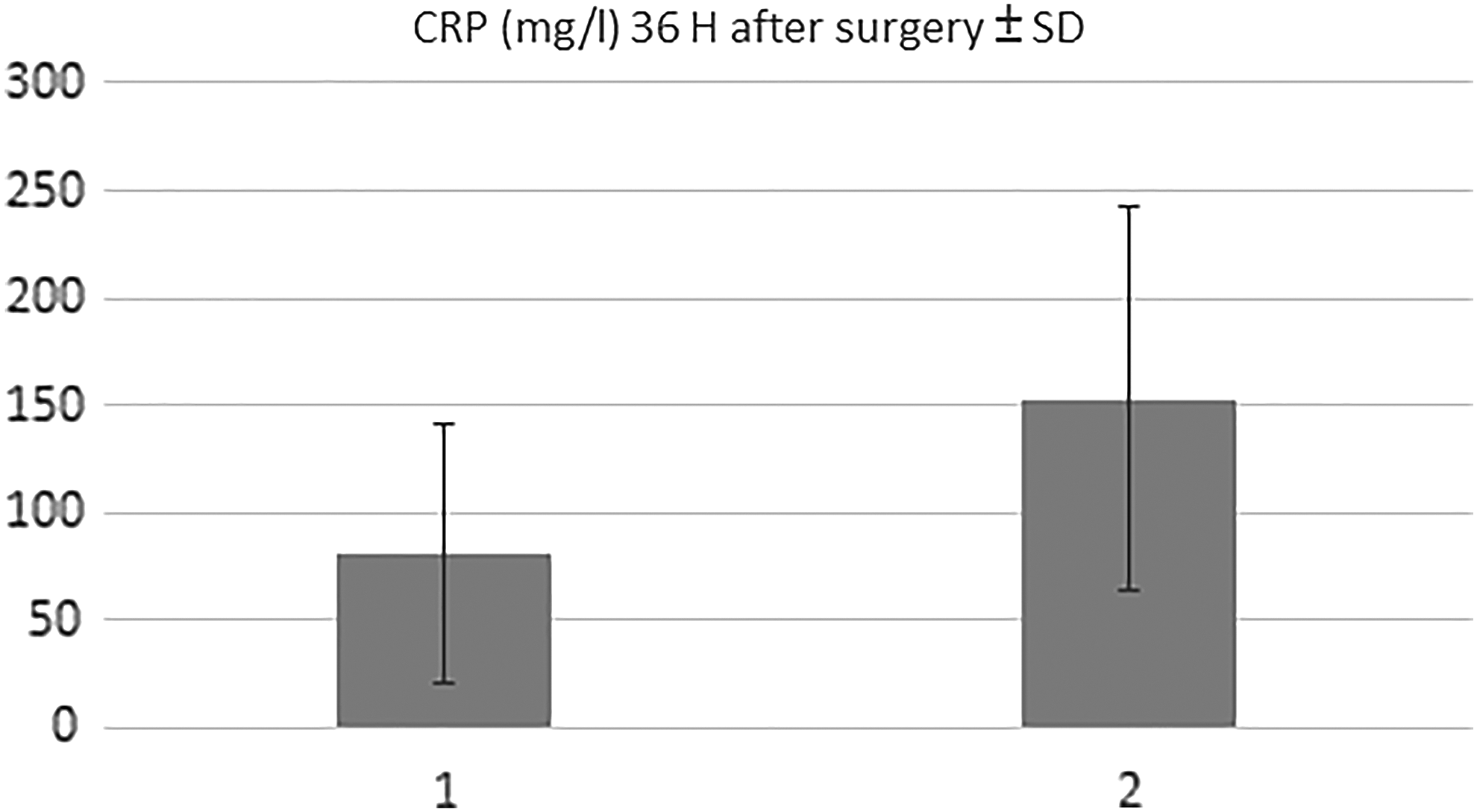
CRP levels 36 hours after surgery in two groups. CRP, C-reactive protein.
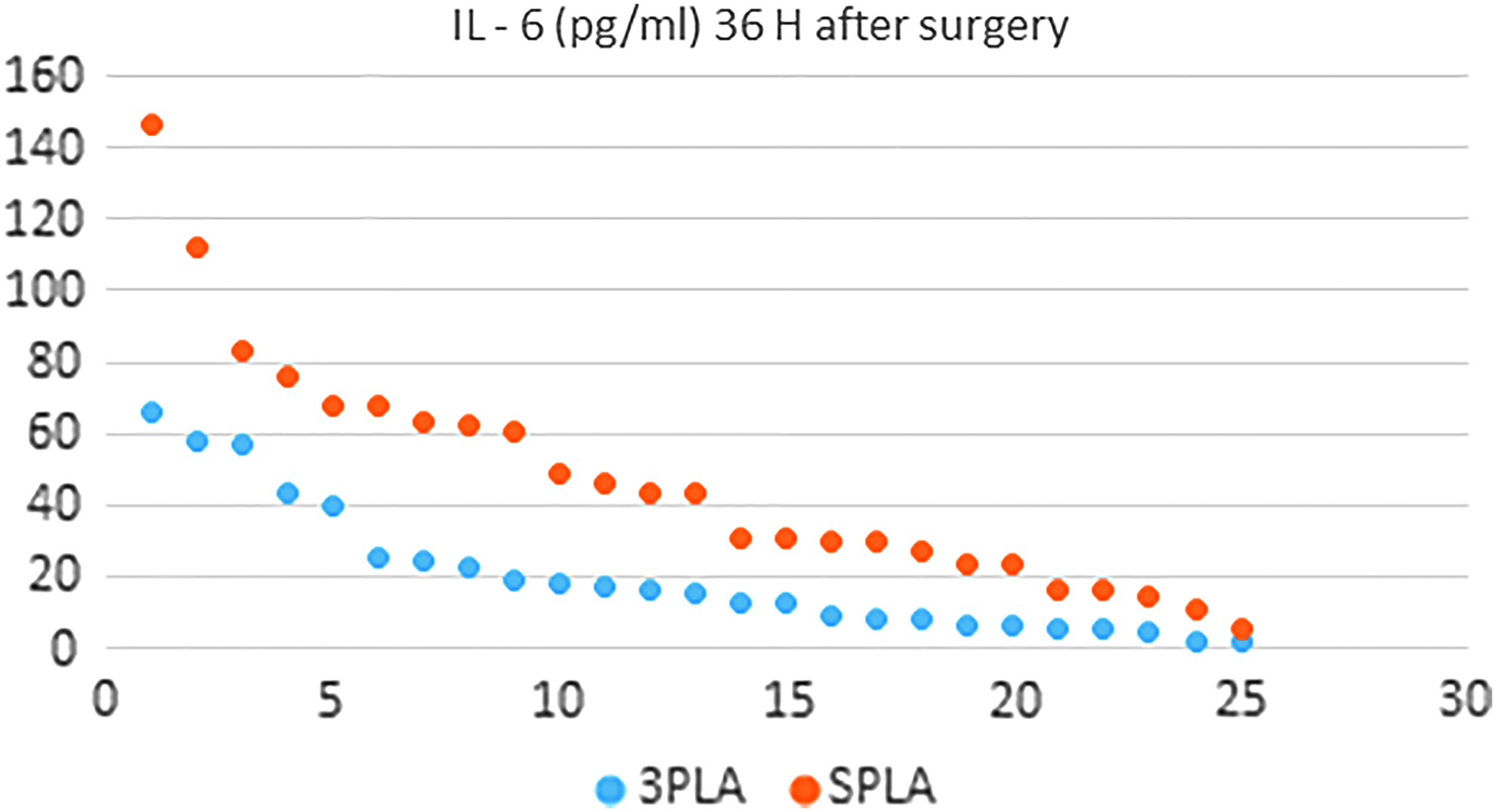
Dot plot presenting IL-6 levels 36 hours after surgery in two groups. The results are ordered from the highest to the lowest. IL-6, interleukin-6.

Dot plot presenting CRP levels 36 hours after surgery in two groups. The results are ordered from the highest to the lowest. CRP, C-reactive protein.
Laboratory Test Results of Patients in Single-Port Laparoscopic Appendectomy and Three-Port Laparoscopic Appendectomy Group of Single-Port Laparoscopic Appendectomy Versus Three-Port Laparoscopic Appendectomy Study
Bold fonts present statistically significant data.
3PLA, three-port laparoscopic appendectomy; CRP, C-reactive protein; IL-6, interleukin-6; SPLA, single-port laparoscopic appendectomy.
The Difference (Δ) in the Levels of Interleukin-6 and C-Reactive Protein in Patient Groups Single-Port Laparoscopic Appendectomy and Three-Port Laparoscopic Appendectomy of the Single-Port Laparoscopic Appendectomy Versus Three-Port Laparoscopic Appendectomy Study
Bold fonts present statistically significant data.
3PLA, three-port laparoscopic appendectomy; CRP, C-reactive protein; IL-6, interleukin-6; SPLA, single-port laparoscopic appendectomy.
Discussion
It might seem that SPLA is the best minimally invasive technique available, as it is the newest and the most advanced, yet it is necessary to overcome this opinion bias and include scientific results, so as to believe what one sees, not see what one believes. 16 In some areas of surgery, there may be a question that SILS is industry driven 7 and that some single-incision operations may be performed as a cause of fashion and prestige it creates, regardless of underlying scientific evidence.
What seems to be typical for comparison between SPLA and 3PLA17,18—there is no difference between the length of hospital stay and complication rate when we compare groups with the similar staging of appendicitis. Other hallmarks of SILS are the duration of surgery, postoperative pain reduction, analgesic use reduction, and what is the primary concern of the article, tissue stress, and inflammation caused by surgery are discussed as follows.
Duration of surgery
The results show that on average the SPLA took 10 minutes longer than 3PLA. The difference did not diminish with consecutive surgeries as the operating surgeons were experts in the field of single-incision laparoscopic surgery being already on the plateau of the learning curve. Also, other studies confirm that SPLA lasts longer that 3PLA.18–20 This may be caused by the fact that SPLA requires more steps to reach, dissect, and remove the appendix; in other words, it is associated with higher operational difficulty. It is also suggested that obesity is an unfavorable factor extending the duration of SPLA, length of stay, and length of postoperative analgesia, without any impact on 3PLA.
Postoperative pain
In our study, we used the visual analog scale (Fig. 1), which was feasible for all our patients. The SILS group rated pain statistically higher, and this result differed from the result obtained and published by the SCARLESS study group in 2015 17 but was in accordance with Kim et al. results from 2012 21 and Carter et al. results from 2014. 18 The patients commonly localized pain in the vicinity of the umbilicus, in the right lower quadrant of the abdomen, and of the right shoulder. The higher pain score probably is associated with a larger than the conventional diameter of the SILSPort used, more intra-abdominal manipulations and longer duration of surgery. We have also found that patients after SPLA required the longer intake of opioid medications. The difference was statistically and clinically significant, and our result agreed with the results of a recent meta-analysis of the subject. 19
The World Health Organization's “analgesic ladder” can be applied to acute pain, such as postoperative pain. Therefore, in our department in postoperative pain management protocol, we use paracetamol, ibuprofen, and an opioid nalbuphine hydrochloride 0.2 mg/kg b.w. 4 × a day.
Surgical stress
We have discovered that there was a significantly higher rise in CRP and IL-6 levels in SPLA group (Figs. 2 and 3). The difference was especially visible 36 hours after surgery. Because the staging of appendicitis was similar in both groups and there were no additional ongoing disease processes, we assumed that the difference is caused by greater tissue injury in SPLA group. Generally, the level of trauma response is determined by the extent of tissue damage, and this is proportional to the severity of surgical stress. 22 It is known that the surgical stress is more significant after open than laparoscopic appendectomy in children 10 and after open than TULAA, 9 but there were no such comparisons between SPLA and 3PLA earlier. Numerous controlled trials in adults demonstrated reduced IL-6 levels after laparoscopy versus open approach. 23 Fewer studies have compared this phenomenon after laparoscopy versus open surgery in children. 24
Nevertheless, lower cytokine levels are assigned to pneumoperitoneum, and specific effects of CO2 on peritoneum that leads to lower immune responses, 25 and this fact is well documented. The question remains what the effect of mechanical irritation of tissues during laparoscopic surgery on the cytokine levels is. Also, it is not sure that the postoperative rise in CRP and IL-6 levels and especially the difference in the rise of cytokine levels between the two studied procedures.
Postoperative peritoneal adhesions are a significant cause of morbidity after an appendectomy. Particularly they can lead to mechanical bowel obstruction and technical difficulty during subsequent surgical procedures. There is evidence from studies on animals that IL-6 plays a significant role in the formation of peritoneal adhesions. 4 and that there is a link between IL-6 and adhesion formation after surgery. 26 Therefore, it is possible that SPLA may lead to a more substantial proportion of postoperative adhesions in the SPLA group, but there is a need for long-term follow-up studies to confirm this supposition.
Efficacy and safety
No differences were found when it comes to length of hospital stay and complications rate. Both SPLA and 3PLA provided postoperative recovery with equal efficacy and safety. Similar results have been reported earlier.19,20 One meta-analysis showed that, statistically, patients after SPLA returned to full activities earlier although these differences were not clinically significant. 27
Cosmesis
It is not disputable that there is only one incision in SPLA instead of multiple in 3PLA. One study found, however, that the cosmetic results are found to be more important from surgeons than from patient's perspective. 27 On the one hand, patients generally accept the single-port surgery concept but seem to be reluctant to NOTES (Natural Orifice Transluminal Endoscopic Surgery).28,29 Cosmetic effects in adults seem to be better after SPLA compared with standard 3PLA, 29 and we have strong evidence from the SCARLESS study group. 17 On the other hand, there is no evidence that cosmetic effects of SPLA are better than of 3PLA in children and that it will make any difference when they become adults, and there are results of another randomized controlled trial implying that long-term body image and cosmetic appearance are excellent in both SPLA and 3PLA groups. 18 Finally, patients evaluate cosmetic effects after 3PLA very well, 30 and there is probably little, if any, room for improvement.
Single-port surgery is expensive and usually out of reach in most of the low- and even middle-income countries. Unique ports, instruments, and their maintenance generate high costs. It is also unclear whether the use of those instruments is well grounded?
To maximize patients' safety, improve the feasibility, and to rationalize the approach to laparoscopic appendectomy we devised an algorithm 15 incorporating TULAA 31 as a starting point. We believe that our approach is cost-effective, improves cosmetic results, and shortens the operative time. A recent multicenter European study of 1092 patients 32 confirms our results. This study supports the decision not to include SPLA in the algorithm. Strong evidence from systematic reviews and meta-analysis also do not support the higher efficacy of SPLA. 33
Conclusion
In our opinion, SPLA leads to more pain, more opiate use, longer OR times, higher inflammatory markers, and longer LOS.
We believe that three-port laparoscopic appendectomies are more beneficial to patients mainly because the time needed to operate is shorter compared with single-port laparoscopic appendectomies and secondly, as they render less operative trauma. What is more, it is reasonable and cost-effective to use a three-step protocol using one, two, or three ports depending on the clinical situation.
We suppose that a more considerable increase in cytokine levels observed after SPLA is associated with a greater mechanical tissue injury and longer operative time, but this hypothesis requires further research.
Footnotes
Disclosure Statement
No competing financial interests exist.