
Abstract
Abstract
Background:
Intrahepatic cholangiocarcinoma (ICC) and gallbladder cancer (GC) are relatively uncommon indications for minimal invasiveness, mainly due to the technical complexity required for a laparoscopic loco-regional lymphadenectomy. The aim of this presentation is to provide a step-by-step overview for the technical approach to laparoscopic lymphadenectomy of the hepatic pedicle and parenchymal transection.
Materials and Methods:
Two cases of an ICC and a GC are shown. Patients were placed supine in the modified French position. One optic port was inserted through open access and four more operative trocars were placed under direct vision in a standardized fashion. Lymphadenectomy of the common hepatic artery (station 8) and of the hepato-duodenal ligament for proper hepatic artery, common bile duct, and portal vein (stations 12A, 12B, and 12P, respectively) is shown. Parenchymal transection is depicted using alternation of an energy device with an ultrasonic aspirator, while intrahepatic vascular structures are sealed with bypolar forceps, clips, or stapled according to dimension.
Results:
In the first case operative time was 210 minutes, lymphadenectomy time (LT) 40 minutes, and estimated blood loss (EBL) 200 mL. Final pathology was consistent with ICC pT2N1(1/7)M0.
In the second case, operative time was 180 minutes, LT 35 minutes, and EBL 150 mL. Final pathology reported gallbladder adenocarcinoma pT2N0(0/7)M0.
Postoperative courses were uneventful; drains were removed on postoperative day (POD) 2. Patients were discharged on POD 3.
Conclusions:
Overcoming the technical limitation embodied by the need of performing an appropriate lymphadenectomy represents the milestone for having patients affected by primary biliary tumors of the liver enrolled to laparoscopy; therefore, this subgroup of patients can benefit from the advantages offered by minimal invasiveness. The leading assumption, however, remains the requirement of performing an oncologically adequate lymph nodal dissection.
Introduction
I
The aim of this video-presentation is to provide a step-by-step overview for the technical approach to laparoscopic lymphadenectomy of the hepatic pedicle and parenchymal transection, with particular emphasis to the technical aspects involved in lymph nodes harvesting. See digital Supplementary Video S1 “Laparoscopic Lymphadenectomy” (Supplementary Data available online at www.libertpub.com/lap).
Materials and Methods
Lymph nodal stations involved in the lymphatic drainage of the liver can be appointed following the classification of the Japanese Gastric Cancer Association for Gastric Cancer. 9 Beginning from the celiac trunk, the loco-regional lymphatic drainage of the liver flows into lymph node station 8–which encompasses nodes around the hepatic artery–and station 12, proper of the hepatoduodenal ligament. Station 12 itself can be divided into stations 12A, 12B, and 12P, respectively for the proper hepatic artery, common bile duct, and portal vein.
Two cases of primary biliary malignancies of the liver are presented for the description of the laparoscopic approach to lymphadenectomy.
Laparoscopic lymphadenectomy for ICC
An ICC in Sg5 was diagnosed, in close vicinity with the gallbladder. An en-bloc bi-segmentectomy of Sg4b and 5 with cholecystectomy was planned, associated to loco-regional lymphadenectomy. Patient was placed supine in a modified French position, where both knees and hips are slightly bent, conferring better stability during reverse Trendelenburg tilting. 10 Five 12 mm ports were placed under direct vision. As lymphadenectomy is particularly demanding due to its proximity with major vascular structures, it is advisable to perform this procedure at the beginning of the surgery.
Station 8 is retrieved by skeletonizing the common hepatic artery at its origin. The hepatic pedicle becomes fully accessible by dividing the cystic duct and cystic artery. Station 12B and 12P are taken from the anterior side of the common bile duct to the posterior side of the portal vein (Fig. 1). Station 12P is completed by taking inter portal-caval nodes, on the posterior aspect of the hepatic ligament. The skeletonization of the anterior aspect of the hepatic ligament completes the lymphadenectomy of station 12A, on the proper hepatic artery, which is encircled on a vessel loop for better traction.

Stations 12B and 12P are retrieved after skeletonizing the common bile duct and the portal vein.
After having completed lymphadenectomy, parenchymal transection takes place, facilitated by an intermittent Pringle maneuver that is performed with tiny vascular clamps rather than with an umbilical tape, due to the exposure of vascular structures. Parenchymal transection is performed associating the use of an energy device and an ultrasonic dissector for parenchymal fragmentation. Intra-parenchymal vessels are either sealed with wet bypolar forceps or interrupted between clips, according to dimension. The transection is conducted on the plane for Sg4b and then for Sg5, using the gallbladder as a site for retraction. The root of the middle hepatic vein is stapled once it is encountered.
A drain tube was left in place to monitor for possible bile leakage.
Laparoscopic lymphadenectomy for GC
The case of a patient affected by GC is presented, presenting a vascular anomaly of the hepatic pedicle. An en-bloc resection of Sg4b and 5 with cholecystectomy was planned.
The dissection is performed analogously to the previous case, retrieving lymph node station 8. After opening the Calot triangle, full exposure of the lateral aspect of the hepatic pedicle gives access to station 12B and 12P, which are harvested.
In this case, a replaced right hepatic artery was present on the lateral side of the hepatic pedicle (Fig. 2). In the absence of a tactile feedback in laparoscopy, an accurate preoperative instrumental assessment must be performed on CT scan to avoid intraoperative vascular injuries. Parenchymal transection is performed, as previously described, once lymphadenectomy is completed.
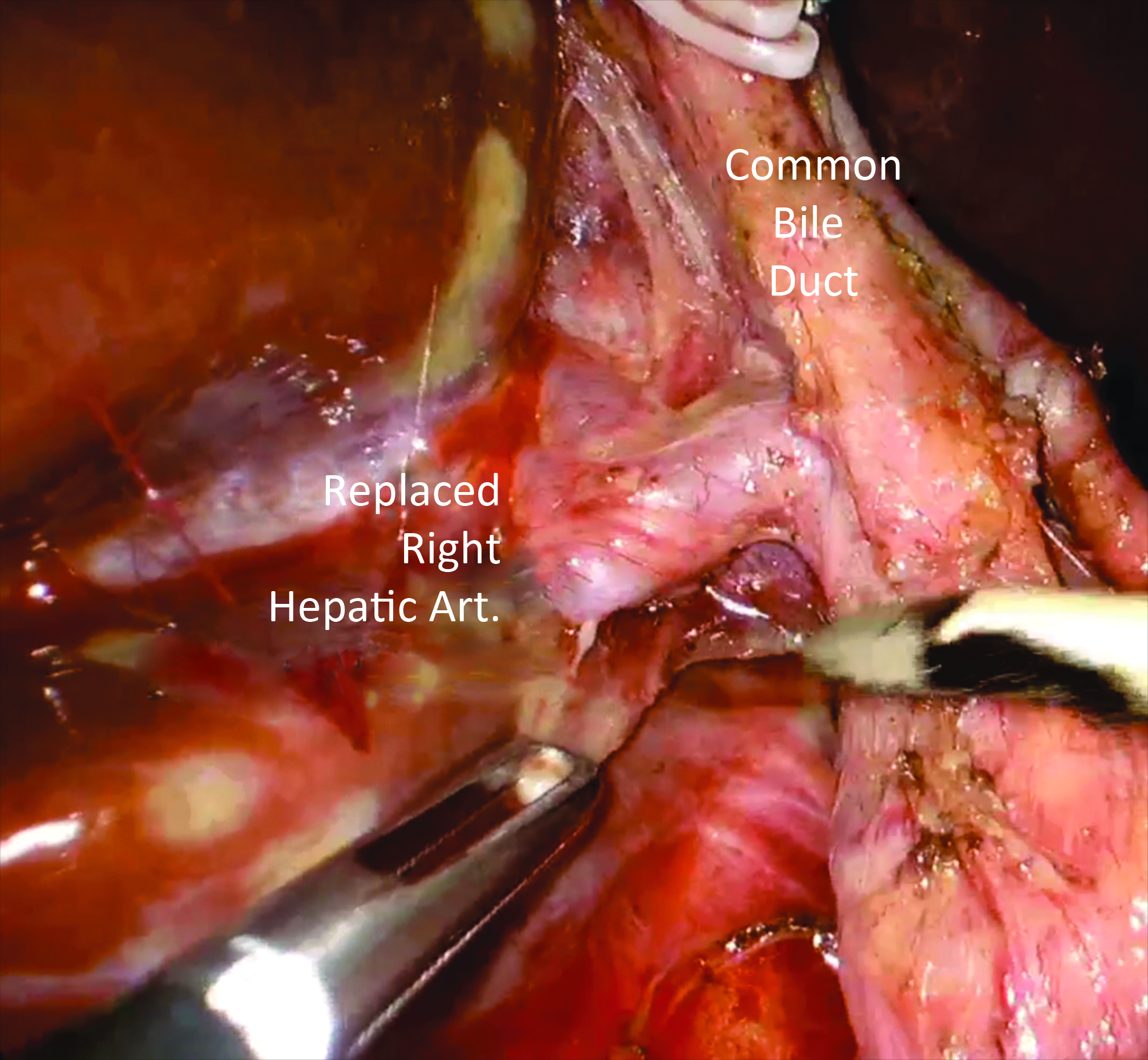
A replaced right hepatic artery flowing on the right side of the hepatic pedicle must be recognized at the instrumental preoperative assessment.
Results
In the first case operative time was 210 minutes, lymphadenectomy time (LT) 40 minutes, and estimated blood loss (EBL) 200 mL. Final pathology was consistent with ICC pT2N1(1/7)M0.
In the second case, operative time was 180 minutes, LT 35 minutes, and EBL 150 mL. Final pathology reported gallbladder adenocarcinoma pT2N0(0/7)M0.
Postoperative courses were uneventful; drains were removed on postoperative day (POD) 2. Patients were discharged on POD 3.
Discussion
A surgical operative technique is presented in a step-by-step fashion with particular emphasis to the laparoscopic approach of lymph nodes station 8 and 12 involved in the lymphatic drainage of the liver.
The need for a routine lymphadenectomy for primary biliary tumors of the liver is a debated topic in literature, being authors who upfront recommend it and others who discourage it.
The supporters of an upfront lymphadenectomy sustain its role not just as a prognostic, but also as a curative one. Bagante et al. 11 analyzed the effect of not performing a lymphadenectomy on a multicentric series of 561 patients from 12 hepatobiliary centers. In the results, they report the short-term postoperative period (within 18 months since surgery) was characterized by a disease-specific survival (DSS) of 70.2% versus 60.6% for N0 versus Nx (P = .019), supporting a therapeutic role of lymphadenectomy. Nevertheless, they found DSS was comparable in the short-term period comparing N1 and Nx (P = .13), while in the long-term period, N1 patients were characterized by shorter DSS in comparison to Nx (DSS at 60 months N1 versus Nx was 15.2% versus 45.8%, P < .001), reinforcing the notion of a prognostic role of lymphadenectomy as one of the strongest predictors of survival. Their conclusion was that lymphadenectomy should be performed for all patients undergoing surgery for ICC and that lack of nodal staging may lead to heterogeneous and potentially incorrect prognostic classification of patients with ICC.
The concept of lymphadenectomy with a curative goal has been adopted by more and more surgeons through time. Zhang et al. 12 investigated on the trends of performing lymphadenectomy in cholangiocarcinoma through years, basing on a multi-institutional database of patients operated with curative intents. Among 1084 cases analyzed, almost a half (49.4%) did undergo concomitant lymphadenectomy and hepatic resection. Authors of this retrospective study evaluated how this trend increased over time, showing an increasing propensity during the study period (from 44.4% to 81.5% between 2000 and 2015, P < .001). Further, authors stratified patients for tumor stage, observing that even in the presence of T1a tumor, 1 out of 5 patients presented nodal metastasis. They concluded that an increasing trend in performing lymphadenectomy suggests a growing adoption of AJCC recommendations in the treatment of ICC.
Other authors retrospectively analyzed their experience on this topic, focusing on lymphadenectomy just for staging purposes. Kim et al. 13 analyzed their casuistry in the last 12 years, encompassing 215 cases of operated ICC. Among these, almost a half (52.6%) did not undergo lymphadenectomy and they observed lymphnodal metastasis rate was independently associated to the risk of recurrence. They finally assessed that a routine lymphadenectomy for ICC did not show in their series any survival benefits and, therefore, it can be considered just for the completion of staging.
Despite these items concerning the curative versus the prognostic role of lymphadenectomy, another topic is a matter of debate, that is, the possibility of performing lymphadenectomy with laparoscopy, criteria which has restricted the minimally-invasive treatment of ICC and GC for a long time. The main reason for this is technical challenge represented by lymphadenectomy, requiring dissection along major vascular structures of the hepatic pedicle. In the literature mainly case reports and case series can be found. Among these, Levi Sandri et al. 14 conducted a review collecting the most significant experiences, aimed principally to assess feasibility and safety of the laparoscopic approach. Ratti et al. 15 performed a propensity score-based study aimed to analyze their single institutional experience: 20 patients operated for ICC with curative intent were compared to 60 open cases. Inside the laparoscopic arm, 85% of patients did undergo a major resection. Noninferiority was demonstrated for the laparoscopic series in terms of perioperative morbidity and mortality and for disease-free survival. Laparoscopic cases, anyhow, were associated to less intraoperative blood loss and to a higher number of harvested lymph nodes, other than to a faster functional recovery.
Eventually, with a look to the future, Beard et al. 16 in their review on minimally invasive treatment of liver tumors introduced the topic of robotic treatment of cholangiocarcinoma. Few experiences are present in the literature tackling cholangiocarcinoma with robot-assisted techniques. An expansion of this field could be hypothesized in the future, given the increased degrees of motility granted by the endo-wrist technology.
Conclusion
Overcoming the technical limitation embodied by the difficulty of performing a minimally-invasive lymphadenectomy marks the step-up point for having patients affected by primary biliary tumors of the liver eligible to laparoscopy; therefore, this subgroup of patients can benefit from the advantages offered by minimal invasiveness. 17 The leading assumption, however, remains the requirement of performing an oncologically adequate lymph nodal dissection.
Footnotes
Disclosure Statement
All authors have no conflicts of interests to disclose, and further disclose any commercial interest they may have in the subject matter of the study and the source or material support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.