
Abstract
Abstract
Purpose:
The aim of this study is to compare minilaparoscopic (MLS) and open pyeloplasty (OP) in children <1 year in terms of intra- and perioperative outcomes and esthetic results.
Materials and Methods:
Patients <1 year of age, with prenatal hydronephrosis, who underwent Anderson-Hynes pyeloplasty for monolateral ureteropelvic junction obstruction (UPJO) at our center from January 2016 to August 2017 were enrolled in the study. Outcomes evaluated were as follows: operative time, length of hospital stay, and postoperative pain anterior-posterior pelvic diameter (APD) reduction. The Vancouver Scar Scale (VSS) was utilized to evaluate esthetic results. Mean follow-up was 26.5 months.
Results:
Eighteen patients (11M, 7F) of mean age 8.1 months (range 4–12) and mean weight 8.5 kg (range 7–10) underwent Anderson-Hynes pyeloplasty in the study period. Nine of eighteen underwent OP, and 9/18 underwent MLS. Mean operative time was 167 minutes for MLS versus 153 minutes for OP (P = .14). Mean hospital stay was 3.9 days for MLS versus 5.3 days for OP (P = .11). Mean APD reduction was 13.6 mm for MLS and 16.5 mm for OP procedures (P = .63). Mean VSS score was 1.3 for VLS versus 3.4 for OP (P = .04).
Conclusions:
MLS pyeloplasty is feasible and safe, and reported equivalent results as open procedure for management of UPJO also in toddlers and infants. We found that the only significant difference between the two approaches in children <1 year was represented by the esthetic outcome in the short follow-up period.
Introduction
The use of minimally invasive techniques in children has become the preferred approach for selected procedures in several centers worldwide.
Ureteropelvic junction obstruction (UPJO) is the most common congenital ureteral anomaly, occurring in 1 per 20,000 newborns. 1 Historically, the “gold standard” treatment for UPJO was represented by the open Anderson-Hynes dismembered pyeloplasty, with success rates from 90% to 100% overall. Endoscopic options for UPJO management have also been described with success rates of 60%–80%. 2 Minimally invasive surgical approaches, such as laparoscopy and, more recently, robot-assisted laparoscopy, have reported several advantages, including reduced postoperative morbidity, better cosmetic outcomes, less postoperative pain, and shorter hospital stay compared with the traditional open approach. 3 The first description of laparoscopic pyeloplasty was made in 1995. Since that time, this technique has gained consensus in the pediatric population, with success rates similar to the open one. 4
The main criticism to laparoscopic approach has been the patient's age; in fact, at beginning some surgeons preferred to limit the procedure to children >1 year of age. 5 The feasibility of laparoscopic pyeloplasty in smaller children was thereafter analyzed and assessed by many authors.6–8 Laparoscopic pyeloplasty, in this category of patients, requires advanced technical skills due to a more confined intra-abdominal working space (0.5–1.0 L) and smaller ureteral diameter. 9 The current availability of miniaturized laparoscopic instruments enhances the ability to perform the ureteropelvic anastomosis. 10 In minilaparoscopy, surgeons use very small (3 mm diameter, 20 cm in length) instruments, decreasing surgical trauma and postoperative pain.11,12
The aim of our study is to compare the functional and cosmetic outcomes of minilaparoscopic (MLS) and open pyeloplasty (OP) in children <1 year.
Materials and Methods
Patient enrollment
Patients <1 year of age, who underwent Anderson-Hynes pyeloplasty for monolateral UPJO at our center from January 2016 to August 2017, were enrolled in the study. Nine patients underwent MLS pyeloplasty, and 9 underwent OP. We collected patients' demographics, clinical presentation, and outcomes in addition to pre- and postoperative imaging.
Surgical criteria and outcome parameters
All children were presented with prenatally diagnosed hydronephrosis. The diagnosis of UPJO was confirmed postnatally based on renal ultrasonography (US) and MAG3 renography. Grading of hydronephrosis was based on the Society of Fetal Urology (SFU) classification, and anterior-posterior pelvic diameter (APD) was measured on sonography. Criteria for decision to surgical intervention were as follows: a persistent significant hydronephrosis or its worsening on ultrasound check and an obstructed washout curve on MAG3 renogram.
All the surgeries were performed by a single expert surgeon who completed his learning curve before the study started with >100 pyeloplasties in the adult patient. MLS operations were performed by the transperitoneal route using three or four ports. OP procedures were performed by retroperitoneal route. All anastomoses were stented. Ureteral stent was removed after mean 4 weeks (range 21–32 days). Total operative time was defined as the time taken from the start of the anesthesiologic maneuvers to the wakeup of the patients.
All patients were followed up postoperatively with US at 1, 5, and 8 months after stent removal. Outcome parameters measured included operative time, length of hospital stay, postoperative pain, reduction of APD on ultrasound and esthetic results. The Vancouver Scar Scale (VSS) was used to evaluate the esthetic results. Isotopic renography was done within a year if the dilatation persisted significatively on US, or there were clinical indications.
Surgical technique
MLS technique
After positioning a 8-Ch Foley catheter, the patient was placed in oblique position and placed near the edge of the table. Gel pillows or pads were used to elevate the side to be treated and to protect pressure points. The ipsilateral arm was positioned near the head, and the patient was secured to the bed across chest and legs. The surgeon and the assistant were standing on the same side. A 5-mm trocar for the 30° optic was placed in the umbilicus through open approach, and pneumoperitoneum (8–10 mmHg) was induced. A 5-mm trocar allows the introduction of sutures into the abdomen. After an initial inspection of the peritoneal cavity, the remaining two or three 3-mm working ports were inserted under vision.
We placed the trocars to reach the optimal triangulation of the instruments at the UPJ. We used 3-mm trocars with 20 cm-3 mm-diameter laparoscopic instruments (needle holder, grasper, and monopolar scissors) as the previously reported definition.13,14 The ports were fixed with sterile strip adhesive to minimize the risk of dislodgment during the procedure. After mobilization of the hepatic or splenic flexure of the colon, the ureter was identified in the retroperitoneum and followed toward the pelvis. Once the UPJ was identified, its surface was cleared to identify any polar crossing vessels. The renal pelvis and the ureter were dissected to ensure a tension-free anastomosis. The renal pelvis around the UPJ was incised, and we left it attached to the ureter to serve as a grip. The ureter was cut and spatulated longitudinally until it was wide enough. The UPJ was dismembered preserving the posterior wall. The lower angle of the ureter was fixed with a single stitch to the lowest part of the pelvis. The posterior anastomosis was performed with 6–0 Poliglecaprone 25 (Monocryl®) running suture cut to 15 cm in length and introduced through the camera trocar. The knots were tied intracorporeally and placed outside the lumen. A ureteral double-J stent was positioned in all cases according to antegrade technique, 15 introducing the wire and the stent through one of the 3-mm trocars or percutaneously. A 4.7 Fr-14 cm double-J stent was positioned in 12/18 patients, and a 5 Fr-12 cm double-J stent in 6/18. Successful antegrade stent insertion was facilitated by partially filling the bladder with saline before introducing the wire and checking the external urethral meatus to avoid the exit of wire and stent.
The redundant pelvis was cut, and the anterior anastomosis was completed with a 6–0 running suture same as above. The remaining pelvis was closed. The needles were removed through the 3-mm port under direct vision after manual straightening of the needle. A Penrose drain in the abdomen was positioned according to the surgeon preference.
Open technique
OP was performed according to the standard Anderson-Hynes technique by an anterolateral incision of 3–4 cm. 16
Postoperative management
The patients restarted full oral feeding after they had recovered from anesthesia. The bladder catheter was removed on the second postoperative day and drained the day after, before discharge. The double-J stent was removed under general anesthesia 4 weeks after the operation by cystoscopy.
Postoperative pain management
For postoperative pain management, two different protocols were used depending on the approach.
In MLS approach, no epidural blocking or regional anesthesia was used. The protocol was envisaged using Paracetamol (<10 kg 7.5 mg/kg; >10 kg 15 mg/kg) and Tramadol (1 mg/kg/dose) intravenously. In case of vomiting, Zofran 0.2 mg/kg was administered. In OP approach, the epidural protocol was based on the use of Levobupivacaine 0.1% and Fentanyl. Postepidural antalgic therapy was performed with Paracetamol and Tramadol as previously described. The drugs were administered every 8 hours and at a 2-hour interval between Paracetamol and Tramadol in the first 48 hours. After 48 hours, the administration of the drugs was continued every 12 hours, and was suspended after two consecutive negative algometries. In case of intense pain, a bolus dose (10 minutes) of morphine 0.05 mg/kg diluted in 10 mL of 0.9% saline was administered.
Esthetic results
Esthetic results were evaluated by VSS. The scale takes into account four different parameters: vascularity, pigmentation, pliability, and height. The maximum score possible is 14, indicating the worst possible scar result, with a score of 0 indicating normal skin. 17
Statistical analysis
Statistical analysis was performed using SPSS®. Normal variables were compared between the two groups using the chi-squared test. P < .05 was considered statistically significant.
Results
A total of 18 patients (11 boys and 7 girls) <1 year with monolateral UPJO underwent pyeloplasty in the study period, and they were grouped according to the surgical approach, MLS or OP. In MLS group, the average patients' age at surgery was 10 months (range 7–12 months) and the average weight was 9.14 kg (range 7.4–10 kg). In OP group, the average patients' age at surgery was 6.3 months (range 4–9) and the average weight was 8.01 kg (range 7–9.3 kg). Patients' characteristics are listed in Table 1.
Patients' Characteristics
APD, anterior-posterior pelvic diameter; NA, not applicable; VLP, videolaparoscopic.
Three of nine children in the OP group and 3/9 in the MLS group underwent positioning of a percutaneous nephrostomy before surgery. An aberrant crossing polar vessel was found in 2/9 patients in the MLS group. An abnormal renal rotation was found in 2/9 in the OP group. The average operative time was 167 minutes for MLS (range 140–210 minutes) and 153 minutes for OP (range 95–240 minutes) with no significant difference between the two groups (P = .14). A perirenal drain was placed in 8/9 MLS patients and in 8/9 OP patients (Table 1), and removed after the catheter removal. In 2 very recent patients, the drainage was not positioned according to the surgeon preference without any consequence.
The average hospital stay was 3.9 days in MLS group (range 3–5 days) and 5.3 days in OP group (range 4–12 days), with no significant difference between the two groups (P = .11). No intraoperative complications were recorded. Postoperative pain was well controlled in all patients, and no one required adjunctive therapy. Bladder catheter was removed after 2.3 days in MLS group (range 2–4 days) and after 3.7 days in OP group (range 3–6) (P = 1); in the same way, the drain was removed after 3.2 days in MLS group (range 3–5 days) and after 4.1 days in OP group (range 3–7 days) (P = .63) (Table 1). The average follow-up was 26 months for MLS and 27.1 months for OP.
In all patients, US revealed a statistically significant decrease of hydronephrosis. The average preoperative APD was 24.9 mm for MLS (range 15–42 mm) and 25.5 mm for OP group (range 18–45 mm) (P = .11). The mean follow-up was 21 months. At the fifth postoperative month, the ultrasound showed an average APD of 11.3 mm for MLS (range 8–23 mm) and 9 mm for OP (range 5–15.5 mm) (P = .63). In 1/18 patients of MLS group, there was a residual dilatation with good drainage at renography (Fig. 1).
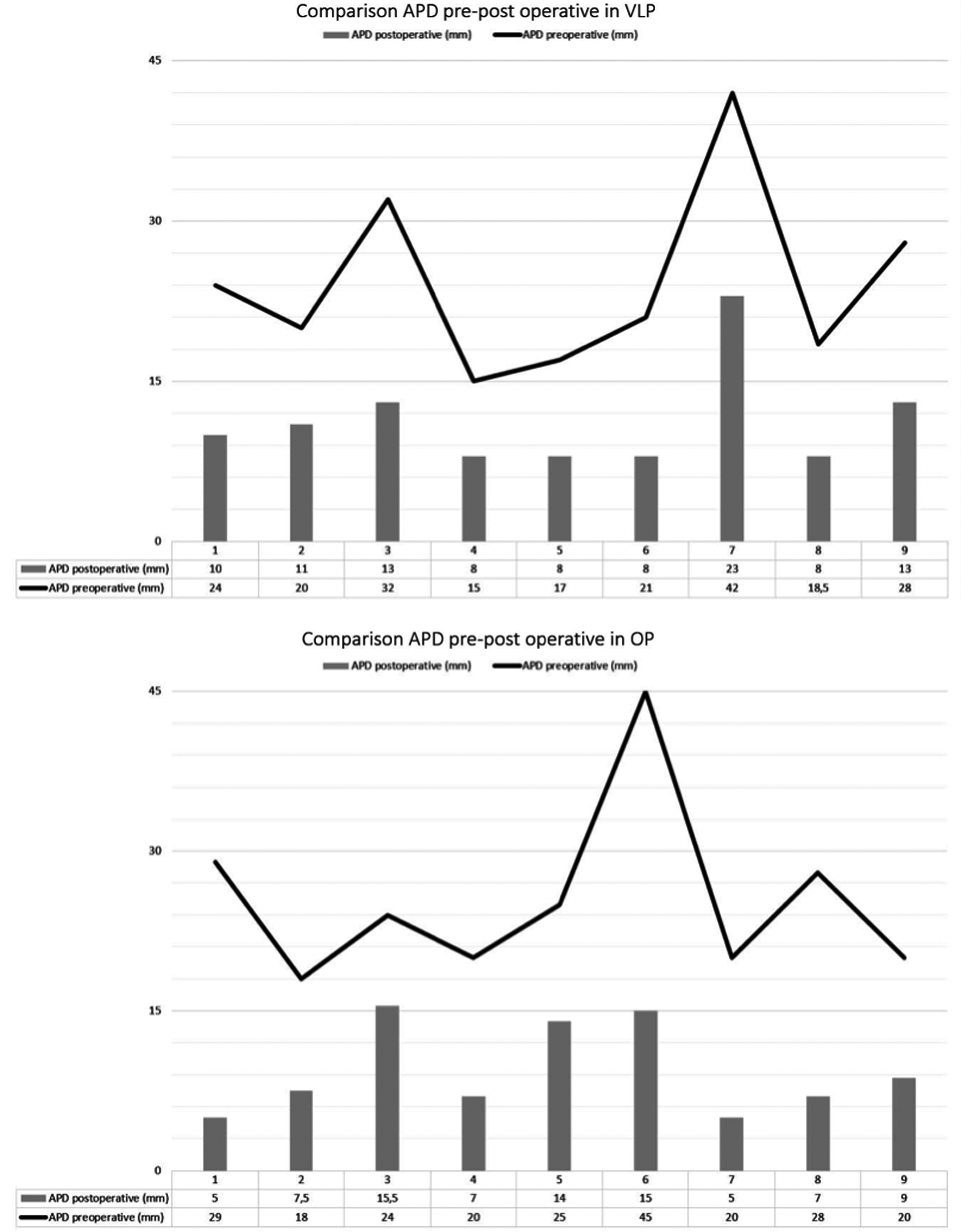
Comparison of pre- and postoperative APD in open and laparoscopic patients. APD, anterior-posterior pelvic diameter.
With regard to esthetic results, children who underwent MLS reported a significantly better average VSS score (1.3 [range 0–3]) compared with OP (3.4 [range 1–5]) (P = .04) (Table 1).
Discussion
Although most prenatally diagnosed hydronephrosis resolves spontaneously with observation, a subset of patients presents UPJO and requires surgical intervention in the first year of life. Since the initial report in 1995, laparoscopic Anderson-Hynes pyeloplasty in children has gained popularity, and in the last 10 years it has been established as a safe and efficacious alternative to the open procedure. More recently, some new modifications have been reported to be applied in infants and newborns.9,18 At the same time, the laparoscopic approach could explore the abdomen cavity, and also repair or correct something unplanned before the surgery plan. 19 Mini-invasive techniques require more expertise and a longer learning curve compared with the open approach. However, some authors showed advantages in children in terms of early recovery, better cosmetic outcomes, and less use of intraoperative and postoperative narcotics.20,21 According to these minimally invasive advantages, some authors proposed a hybrid technique of trocar assisted pyeloplasty: this allows isolation of the UPJ and combines the laparoscopic and OP approaches, which also avoids the need for intracorporeal laparoscopic suture.22,23 Nevertheless, the use of pure laparoscopic pyeloplasty remains controversial in very young children.
Tan in 1999 reported two failures in 3-month-old toddlers and suggested not to perform laparoscopic pyeloplasty in patients <6 months. 24 Conversely, in 2006, Metzelder stated that this procedure is feasible in children of all ages, despite the possible technical difficulties. 25 In 2006, Kutikov et al. reported a 100% success rate in 8 children <6 months who underwent transperitoneal laparoscopic pyeloplasty. 26
The development of advanced instruments and technical modifications has made mini-invasive pyeloplasty a feasible and safe surgery even in infants and newborns. Robotic pyeloplasty, as reported by many authors, is feasible in children of all ages, but a robotic system is often not available in all pediatric centers. 21
A disadvantage reported with laparoscopic approach is a longer operative time compared with open approach, especially in the infant population due to technical challenges. However, we did not report any significant difference between operative time of MLS and OP in our series (P = .14).
We suggest some tricks to easily perform the procedure: first of all, it is preferable to adopt 3-mm screw trocars or alternatively to fix smooth trocars to the skin with a sterile adhesive to avoid their dislodgment during the change of the instruments. In addition, before surgery it is advisable to perform a bowel preparation with simethicone and enemas to empty the intestinal loops that are commonly distended in infants. This bowel preparation allows us to obtain a larger working space and to accomplish the procedure, keeping the pneumoperitoneum pressure stable ∼8–10 mmHg. 27
While the advantages of laparoscopic surgery in children in terms of early recovery and less postoperative pain are well studied, the main advantage of minilaparoscopy in infants is cosmetic, since the 3-mm ports leave little visible scars.7,10 These data are confirmed in our series. We did not find any significant difference between the OP and MLS groups in terms of operative time, pain management exceeding the protocols, hospitalization, and reduction in APD. We then investigated the patients' esthetic results using the VSS, and we found a statistically significant difference between the two groups (Table 1). In our series, the score was 1.3 in videolaparoscopic and 3.4 in OP. All the scars appeared esthetically appreciable, but those of the MLS sample were of better appearance until hardly visible.
While the technique of laparoscopic pyeloplasty in children is well established, the search continues for the ideal method of stenting the anastomosis. Antegrade placement of a double-J stent has been shown to reduce operative time.15,26
Some authors prefer to perform unstented laparoscopic pyeloplasty in young children, to prevent pyelonephritis and avoid secondary anesthesia. In open repair a transanastomotic stent is usually preferred or alternatively some authors reported they left the anastomosis unstented.28–30
In both OP and MLS groups, we used the same antegrade technique without finding stent-related complications. We believe that antegrade insertion after the posterior pyeloureteral anastomosis precludes dislodgment.
Conclusions
MLS pyeloplasty is feasible and safe, and reported equivalent results as open procedure for management of UPJO with excellent functional outcomes also in toddlers and infants. 31 We found that the only significant difference between the two approaches in children <1 year was represented by the esthetic outcome in the short follow-up period. A larger randomized study with longer follow-up is necessary to evaluate if the difference in esthetic results persists lifelong and to verify the functional outcome of those different techniques. A surgeon and an expert team is obviously required in both laparoscopic and open procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.