
Abstract
Abstract
Background:
Laparoscopic hepatectomy (LH) has been reported as a safe and efficacious treatment for hepatocellular carcinoma (HCC) patients. However, in cirrhosis patients, LH may be more complex and challenging. So, the short- and long-term outcomes should be well evaluated between LH and open hepatectomy (OH) in HCC patients with cirrhosis.
Objectives:
To compare the short- and long-term outcomes of LH with OH in HCC patients with cirrhosis.
Materials and Methods:
The PubMed, EMBASE, and Web of Science were systematically searched to identify the clinical trials published until July 2018 on the comparison of LH and OH in HCC patients with cirrhosis. The statistical analysis was conducted by the Review Manager 5.3 (Cochrane Collaboration, Oxford, United Kingdom). Short-term outcomes included blood loss, operation time, blood transfusion, postoperative complications, mortality, postoperative hospital stay, tumor size, and surgical margin. Long-term outcomes included 1-, 3-, 5-year overall survival (OS) and 1-, 3-, 5-year disease-free survival (DFS).
Results:
Seventeen studies with 2004 patients were included in this meta-analysis. For short-term outcomes, LH suggested less blood loss, lower blood transfusion rates, reduced occurrence of postoperative complications, wider surgical margin, shorter postoperative hospital stay, and declined rate of mortality (all P < .05). However, there was no significant difference in operation time (P = .67) between the two groups, whereas tumor size was larger in OH (P = .004). As to long-term outcomes, 1-, 3-, 5-year OS and 1-year DFS were higher in LH group (all P < .05). Nevertheless, there were no significant differences in 3- and 5-year DFS (P = .23 and .83, respectively).
Conclusions:
For the HCC patients with cirrhosis, current evidence suggests that LH shows not only better outcomes in short term, but also a comparable and even improved long-term prognosis.
Introduction
Hepatocellular carcinoma (HCC) is ranked the fifth in the most common neoplasm in the world, and is also the third leading cause of cancer-related death, 1 about one million people died each year, 2 and more than 80% of HCC patients have the background of cirrhosis. 3 The mortality is on the rising in these HCC patients with cirrhosis in developed countries, however, it is declining or stabilizing in noncirrhotic patients. 4 At present, surgical resection, liver transplantation, percutaneous ethanol injection, sorafenib, transarterial embolization, or chemoembolization are widely accepted as the main therapeutic approaches to HCC. 5 Although liver transplantation may be curative for these patients potentially, but in consideration of the waiting time, selection criteria, and the shortage of donors, it could not be large scale applied currently. 6 Due to the advances in technology and postoperative management, hepatectomy is still the first-line treatment of the HCC patients with compensated cirrhosis. 7
After the first applied to cholecystectomy in 1985, 8 laparoscopic technique has gone through a substantial development, and having a huge impact on the development of surgery on its own advantages. The first International Conference on Laparoscopic Liver Surgery was held in America in 2008 and going through the Louisville Statement, the laparoscopic hepatectomy (LH) was recommended to the patents with solitary lesions, and tumor in the location of segments 2 to 6, 5 cm or less. 9 After that, the number of the LH that was reported all over the world have been increasing gradually. Despite these great developments of LH, it is still not welcomed widely due to the controversies of surgical margin, the spread of tumor and the long-term survival. 10 Some studies have proven the safety and efficacy of LH in normal HCC patients.11–15 But for these cirrhotic patients, liver resection may lead to significant intraoperative bleeding and postoperative ascites, even the liver failure in some patients. 16 So the safety and efficacy of LH in HCC patients with cirrhosis may be different from previous studies. In addition, oncological outcome of the LH has not been widely supported by the literature. So the approaches of hepatectomy should be selected carefully for these patients.
There were two meta-analyses that compared the safety and efficacy of LH and open hepatectomy (OH).17,18 However, they only included 4 and 7 studies in their meta-analyses, respectively, and many relevant studies were omitted. Furthermore, some new literature has been published in the last 2 years. Herein, we conducted this meta-analysis to review and update the outcomes of LH and OH in HCC patients with cirrhosis more comprehensively with 17 studies included and 2004 patients enrolled totally. In contrast, our meta-analysis included more matched studies and patients, which may provide a high-quality evidence of short- and long-term outcomes in HCC patients with cirrhosis undergoing LH and OH.
Materials and Methods
Search strategy and identification of studies
The PubMed, EMBASE, and Web of Science were systematically searched, the last time of the searching was set to July 2018. The searching terms included: “laparoscopic hepatectomy,” “laparoscopic liver resection,” “open hepatectomy,” “open liver resection,” “traditional hepatectomy,” “traditional liver resection,” “hepatocellular carcinoma,” “liver cancer,” “hepatic tumor,” “cirrhosis,” and “hepatocirrhosis.” References of the relevant studies were also assessed to improve the rates of detection.
Inclusion and exclusion criteria
Inclusion criteria: (1) The study should be involved with the comparison between the LH and OH in HCC patients with cirrhosis. (2) Data reported on the short- and/or long-term outcomes should be adequate enough. (3) The language was restricted to English.
Exclusion criteria: (1) The study was only involved with one of the treatments of hepatectomy and with no comparison. (2) Reviews, letters, and case reports. (3) Data were unextractable.
Data extraction and quality assessment
Two authors (S.J.and Z.W.) identified and reviewed the studies independently. The data extraction included: the first author, region, publication form, study design, period, number of patients, age, Child-Pugh, and short- and long- term outcomes. Discrepancies were resolved through discussion. If this failed, a third author participated in the discussion until consensus was reached. The Newcastle–Ottawa Scale (NOS) was adopted to assess the quality of nonrandomized studies, which was with a maximum of 9 scores. If the cumulative scores were <7, it was regarded as low quality, if the scores were ≥7, high quality was endowed. The Jadad standards were used to assess the quality of randomized controlled studies, which with a total of 5 scores, if the cumulative scores were ≥3 and <3, were considered of high quality and low quality, respectively.
Outcomes of interest
For the short-term outcomes, we extracted the data of blood loss, operation time, tumor size, surgical margin, the occurrence of postoperative complications, transfusion rate, mortality, and postoperative hospital stay. For the long-term outcomes, data of 1-, 3-, and 5-year overall survival (OS) and 1-, 3-, and 5-year disease-free survival (DFS) were collected.
Statistical analysis
The short-term outcomes included: blood loss, operation time, blood transfusion, postoperative complications, mortality, postoperative hospital stay, tumor size, and surgical margin. The long-term outcomes included: 1-, 3-, and 5-year OS and 1-, 3-, and 5-year DFS. Review Manager 5.3 (Cochrane Collaboration, Oxford, United Kingdom) was used to pool the data in this meta-analysis. Odds risk (OR) for dichotomous variables and weighted mean difference (WMD) for continuous variables were used. Heterogeneity was examined using the χ2 and the value of I2. If I2 > 50%, the heterogeneity was deemed to exist between the studies, and the random-effects model was adopted to the data analysis, and when I2 ≤ 50%, the fixed-effects model was used. Pooled estimates were presented with 95% confidence intervals (CIs). In all the studies, a P value of less than .05 was considered to be statistically significant. Subgroup analysis was based on the matched and unmatched studies. Sensitivity analysis was performed by removing individual study in each step to assess the influence of a single study on the overall pooled results. Funnel chart was used to evaluate the publication bias.
Results
Search results and study characteristics
The searching results were represented in Figure 1. A total of 1022 studies were initially identified. After removing the duplicates, 648 articles were screened. Then, 619 articles were excluded from reading the title and/or abstract. For the reasons of review, letter, case report, and unextractable data, 12 studies were removed. Finally, 17 studies16,19–34 met the inclusion criteria we set, in which 10 of them were matched studies25–34 and other 7 studies were unmatched.16,19–24 There were 2004 patients totally, 798 patients were in the laparoscopic group, and 1206 patients in the open group. The studies we included were from different regions of the world (China n = 5, Japan n = 3, France n = 3, Italy n = 3, America n = 1, Korea n = 1, and Egypt n = 1). The characteristics and quality assessment scores of included studies are presented in Table 1 and Supplementary Tables S1 and S2.

Flowchart of study inclusion.
The Characteristics of Included Studies
Median (range).
NOS score.
Mean ± SD.
Mean.
Jadad score.
Mean (95% CI).
CIs, confidence intervals; LH, laparoscopic hepatectomy; MR, matched retrospective; NA, not available; NOS, Newcastle–Ottawa Scale; OH, open hepatectomy; R, retrospective; RCT, randomized controlled trial; SD, standard deviation.
Short-term outcomes
Thirteen studies16,19–21,25–29,31–34 reported blood loss, which suggested that there was less blood loss in the LH group when compared with OH group (1650 patients, WMD = −252.00, 95% CI = −397.08 to −106.92, P = .0007, Fig. 2A), and the same result was also reflected in the subgroup analysis although there was a significant degree of heterogeneity between the studies (I2 = 97%, P < .00001).
Forest plots and subgroup meta-analyses of the blood loss
The operation time was reported in 15 studies.16,19–21,23–29,31–34 The pooled data suggested that there was no statistically significant difference between the two groups (1856 patients, WMD = 5.85, 95% CI = −20.65 to 32.35, P = .67, Fig. 2B); similar results can be observed in both matched and unmatched group. In addition, there also remained a significant degree of heterogeneity (I2 = 95%, P < .00001).
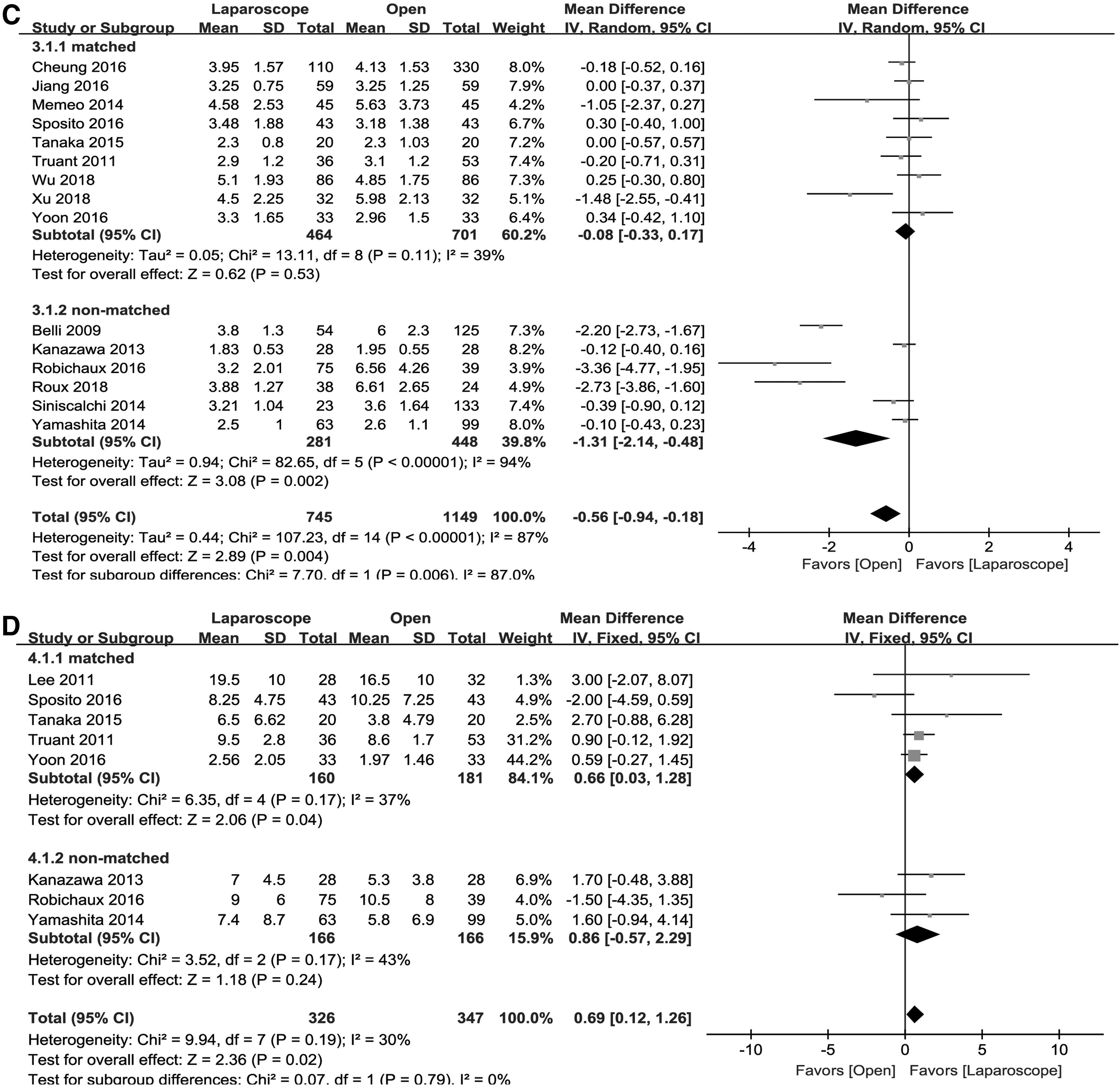
Fifteen studies16,19–23,25–31,33,34 described the tumor size. The pooled data suggested that the size was larger in the OH group (1894 patients, WMD = −0.56, 95% CI = −0.94 to −0.18, P = .004, Fig. 2C). The heterogeneity also existed between the studies. But after subgroup analysis, no significant difference was found in tumor size and the heterogeneity was also decreased in the matched group.
The surgical margin was evaluated in eight studies.16,20,21,26,30–33 The laparoscopic group was subjected to a wider surgical margin in our meta-analysis (673 patients, WMD = 0.69, 95% CI = 0.12–1.26, P = .02, Fig. 2D). Although no significant difference was found in the unmatched group, the studies in matched group also suggested a wider surgical margin.
Thirteen studies21–31,33,34 reported postoperative complications. The result showed that the postoperative complications were less in the LH group (1595 patients, OR = 0.36, 95% CI = 0.27–0.49, P < .00001, Fig. 3A), and the subgroup analysis also presented a similar result.

Forest plots and subgroup meta-analyses of the postoperative complications
There were eight studies16,19,21,25,27,29,32,33, which reported blood transfusion. Patients in the laparoscopic group had a lower rate of blood transfusion (1222 patients, OR = 0.52, 95% CI = 0.32–0.83, P = .006, Fig. 3B).
Total mortality was reported in eight studies.19,22,23,25,27–29,33 The outcome demonstrated that patients in the laparoscopic group showed a decreased rate of mortality (1252 patients, OR = 0.26, 95% CI = 0.09–0.72, P = .009, Fig. 3C) although it was not found in the unmatched group.
The length of postoperative hospital stay was provided in 17 studies.16,19–34 The patients in laparoscopic group had a shorter postoperative hospital stay (2004 patients, WMD = −3.83, 95% CI = −5.09 to −2.56, P < .00001, Fig. 3D); a similar result was also observed in the case of subgroup analysis. Yet, there was a significant degree of heterogeneity between the studies as well (I 2 = 89%, P < .00001).
Long-term outcomes
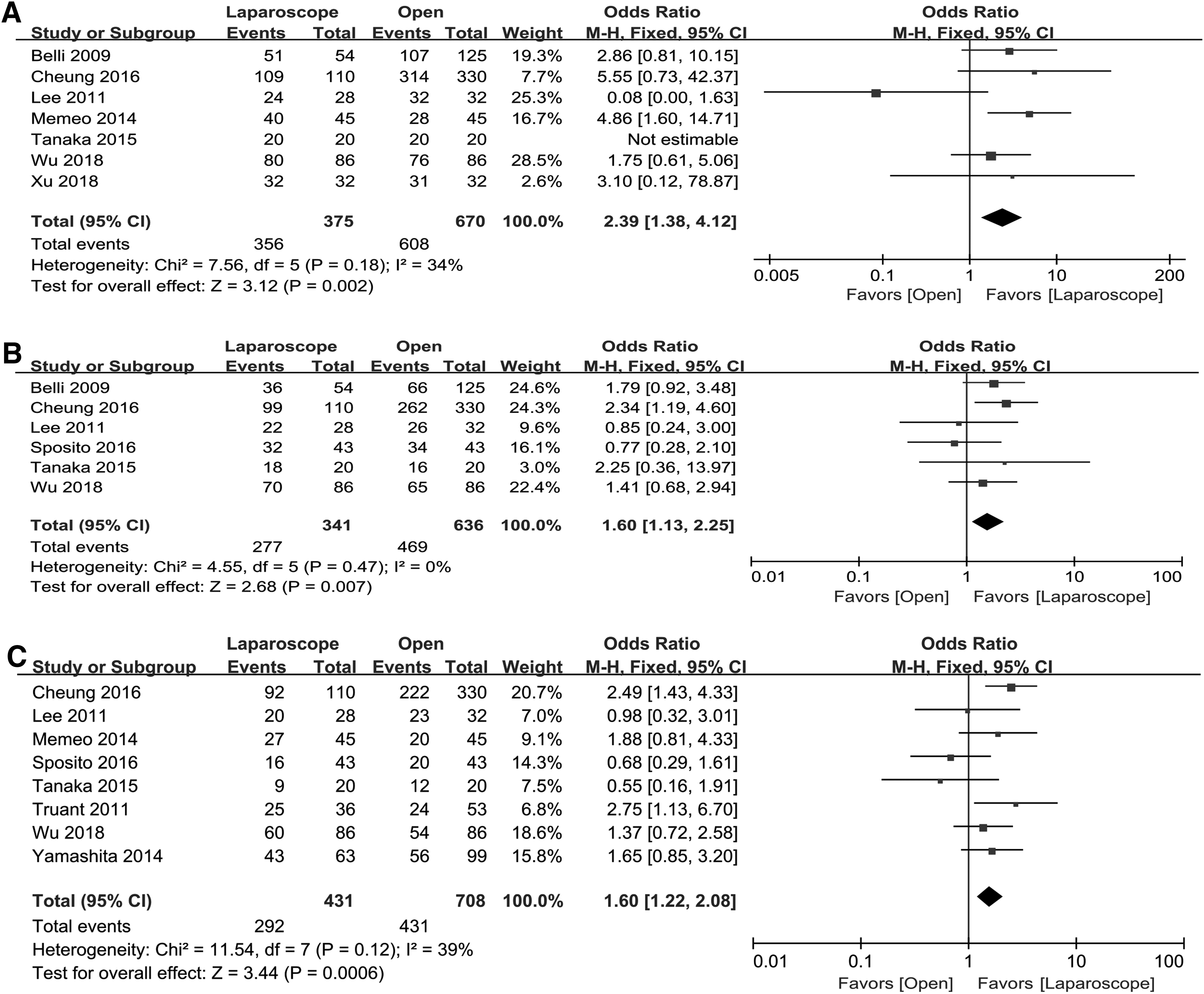
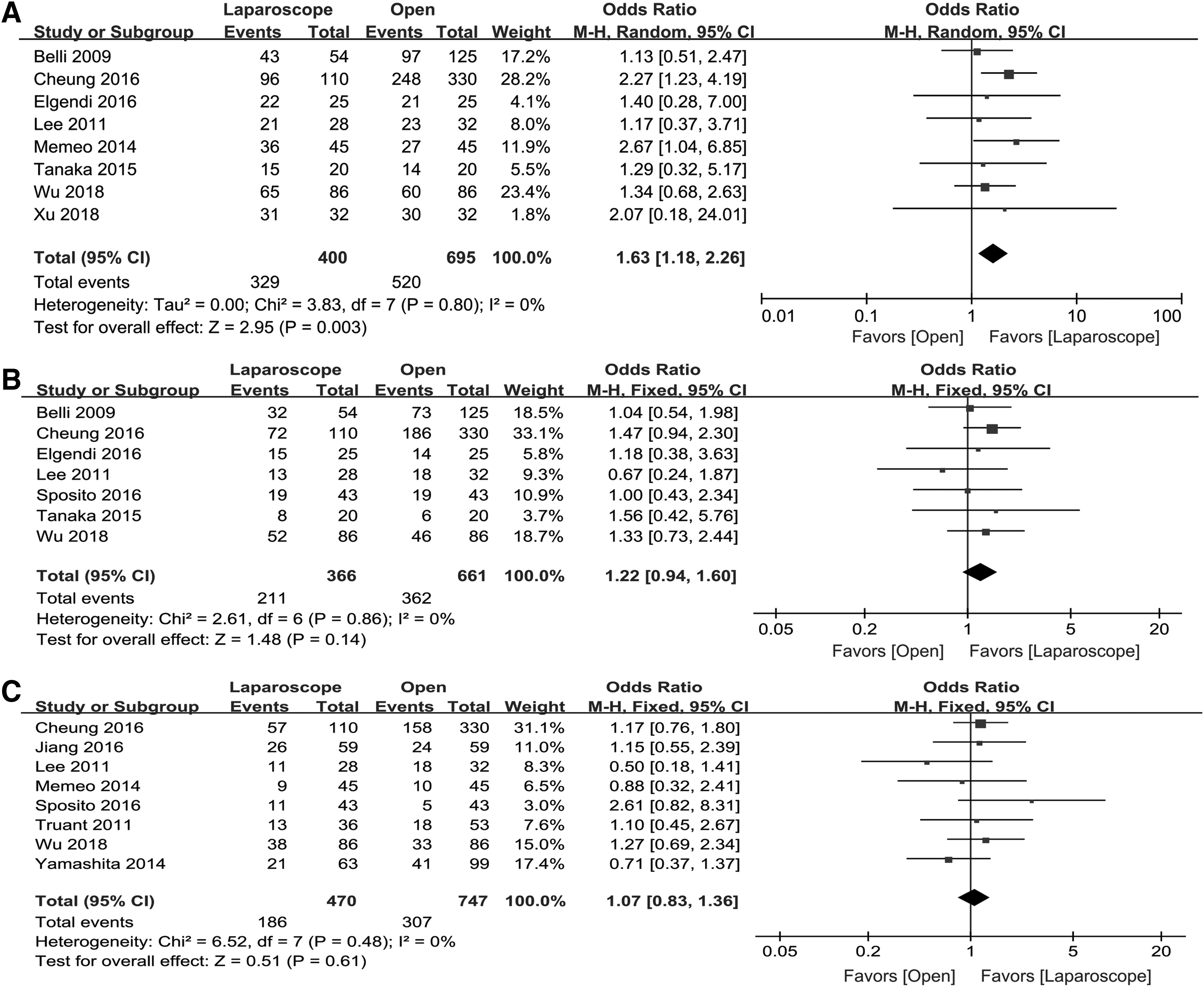
For the long-term outcomes, pooled data revealed that LH suggested the favorable 1-year OS19,25–29,32 (1045 patients, OR = 2.39, 95% CI = 1.38–4.12, P = .002, Fig. 4A), 3-year OS19,25–27,30,32 (977 patients, OR = 1.60, 95% CI = 1.13–2.25, P = .007, Fig. 4B), 5-year OS21,25–28,30,32,33 (1139 patients, OR = 1.60, 95% CI = 1.22–2.08, P = .0006, Fig. 4C), and 1-year DFS19,24–29,32 (1095 patients, OR = 1.63, 95% CI = 1.18–2.26, P = .003, Fig. 5A) when compared with OH. But there were no significant difference in 3-year DFS19,24–27,30,32 (1027 patients, OR = 1.22, 95% CI = 0.94–1.60, P = .14, Fig. 5B) and 5-year DFS21,25,27,28,30,32–34 (1217 patients, OR = 1.07, 95% CI = 0.83–1.36, P = .61, Fig. 5C) between the LH and OH groups.
Forest plots of the 1-year OS
Forest plots of the 1-year DFS
Subgroup analysis
Through subgroup analysis we found that although the tumor size was larger in OH, in the matched group, there was no significant difference between LH and OH (Fig. 2C). What is more, the matched group showed wider surgical margin, lower rates of blood transfusion, and mortality, which were different from the unmatched group (Figs. 2D and 3B, C).
Sensitivity analysis and publication bias
From removing individual study in each step to assess the influence of a single study on the overall pooled results, however, the heterogeneity was not reduced essentially. The funnel plot of the postoperative hospital stay is presented in Figure 6, and there was no significant unsymmetrical distribution around the center line generally, showing no evidence of publication bias.

The funnel plot of postoperative hospital stay.
Discussion
Laparoscopic technique is now widely applied to the abdominal surgery, and its intraoperative and postoperative benefits have been proved in the resection of gallbladder, appendix, and even tumor of the gastrointestinal tract. However, it is still a highly skill-demanded operation when it is applied to liver resection, particularly in cirrhotic patients. On the one hand, the concealed location and special anatomical features of the liver bring many challenges and difficulties to surgeons during the operation. 10 On the other hand, the control of bleeding and parenchymal transection of liver may be much more difficult under the background of cirrhosis, especially in the circumstance of hypertension of the portal vein and coagulation dysfunction. 35 Furthermore, the achievement of a negative surgical margin in the condition of laparoscope still remains a concern. 36 Although, many studies have already shown the advantages of LH in the management of normal HCC patients, for these HCC patients with cirrhosis, the results of LH may be different from previous studies.
The difficulty of keeping hemostasis at the transection surface during the LH is highly concerning, for hemorrhage is still one of the main reasons of conversion especially in those HCC patients with cirrhosis. 37 However, the high clarity and enlarged effect of the laparoscope provide the operation a better vision of the intrahepatic blood vessels actually. 38 With the development of the devices in stanching bleeding, such as microwave coagulators and ultrasonic dissection, the bleeding has been controlled to a great extent. Additionally, the high intraperitoneal pressure caused by CO2 is considered one of the reasons for decreased blood loss in LH. 39 Less blood loss would reduce the requirements of blood transfusion and fluid infusion. In traditional hepatectomy, long operation incision would be needed for the special location of the liver. Abdominal collateral vein and ligamentum teres hepatis would be destroyed at the same time. Nevertheless, LH might be less invasive than OH. It minimizes the operation and damage to the liver during the resection. In LH, long incision is avoided and the ligamentum teres hepatis is reserved, which would protect the abdominal collateral vein circulation. Under these conditions, the occurrence of portal hypertension, refractory ascites, electrolyte disorder, and hypoalbuminemia would be decreased postoperatively.16,40–42 Consequently, the incidences of postoperative complications and mortality would be lower at the advantages of LH. Some studies have showed that patients in laparoscopic group got less pain, earlier recovery of gastrointestinal function, and oral intake in the postoperation.11,43 All these aspects would enhance the recovery of patients and shorten the length of hospital stay.
However, there was no significant difference in operation time between the two groups in our meta-analysis. Previous studies suggested that LH took longer time than OH.41,42 However, studies tended to show that there were no significant differences in operation time between laparoscopy and laparotomy in recent years. Kim et al. 44 even revealed a shorter operation time in laparoscopic approach in their study. This may be owing to the development of surgical instruments. Moreover, the accumulation of experiences and techniques of surgeons may also play an important role. 45 However, most of the studies we included were concerned with minor resection of the liver. As far as major resection, due to the higher demand of technique, LH may consume more time than OH. 31 Therefore, we think more laparoscopic institutions should be established to provide the formal training to surgeons and more technological innovations of LH should be introduced in the following time.
Interestingly, there seems to be emerging data revealing that LH may be comparable to OH oncologically. Comparing with OH, LH achieved a wider surgical margin in our study. Inadequate surgical margin is about a concern when the laparoscope is applied for the resection of the liver. 11 However, owing to the high definition and magnification of laparoscope, microinvasion of blood vessel and tissue can be found. Additionally, the laparoscopic ultrasound may improve the effectiveness in orientation and resection of tumor during the operation. 46 But due to the different formats of data reporting, there were only eight studies that were included into the statistical analysis, and selection bias may have existed. However, Mirnezami et al. 11 and Xiong et al. 40 suggested that there were no significant differences in surgical margin between laparoscopic and open groups in their meta-analyses. Twaij et al. 17 also showed a wider surgical margin in the laparoscopic group. Therefore, we think that the LH can also provide a safe surgical margin.
In our study, the pooled data showed that 1-, 3-, and 5-year OS and 1-year DFS were favorable for the laparoscopic group, but 3- and 5-year DFS were of no significant difference between the two groups. LH may be attributed to the following survival advantages. First of all, LH is associated with less touch and manipulation to the tumor, but during the OH, compression to tumor may occur frequently. This would increase the spread of malignant cells. Moreover, the laparoscopic approach is involved with less blood loss. The study reported by Katz et al. 47 suggested that the increase of blood loss during the resection of HCC is an independent prognostic predictor for tumor recurrence and survival. Additionally, the study showed that the minimal invasion caused by laparoscopic approach appear to induce a decreasing perioperative stress and immune system activation, which may reduce the risk of tumor dissemination and growth. 48 Finally, the wider surgical margin may also provide a better prognosis in the laparoscopic group. Shi et al. 49 suggested that the 2 cm resection range provided a better long-term prognosis for HCC than the conventional 1 cm in their study. Taken together, all these aspects may tend to show the advantages of the LH in improved long-term outcomes potentially. But considering the absence of original data to calculate the hazard ratio, and the studies included were retrospective mostly, more high-quality studies are needed to confirm the results.
There are some limitations to be considered. First, the degree of statistical heterogeneity between the studies in several parameters may lead to overinterpretation of our results. Although subgroup and sensitivity analysis were conducted, the fixed or random-effects model were used appropriately, it is still unlikely to reduce or find the source of the heterogeneity. However, high heterogeneity also can be observed in this series of studies.11–15,18 We think that the high heterogeneity may be due to the different level of skills in surgeons and the differentials of laparoscopic devices among hospitals. Second, the studies we included were involved with different locations and sizes of tumor, which may be related to different level of difficulties to the operation and may affect surgeons' selection of operation approaches preoperatively. Hence, the selection bias may exist, and this may be one of the reasons for the generation of heterogeneity in this meta-analysis. Third, we only compare the overall occurrence of postoperative complications between the two groups, to get more information about the comparison of these two surgical procedures, and further classification of different grades of complications are necessary. Fourth, the studies we included were retrospective mostly, only one study is prospective randomized, but we just found the abstract. So more prospective, randomized controlled studies should be made to confirm the outcomes of this comparison.
In conclusion, the currently available data suggest that compared with the OH, LH shows better outcomes in short term. What is more, the LH is comparable to OH at 3- and 5-year DFS and favorable at 1-, 3-, 5-year OS and 1-year DFS, but this may need more high-quality studies to confirm. Lastly, we think LH is also safe and efficacious for the HCC patients with cirrhosis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.