
Abstract
Abstract
The management of the obstructed hemivagina and ipsilateral renal anomaly, or OHVIRA syndrome, requires vaginal access compromising sometimes the hymenal integrity. A vaginoplasty is the most commonly performed procedure in such scenarios. However, the necessity to maintain the hymen integrity may limit this technique. In this case report, we describe a safe and successful laparoscopy-assisted resection for the management of a high vaginal septum while maintaining an intact hymen.
Introduction
Congenital müllerian anomalies have been reported with a variety of forms in 2%–3% of women.1,2 The müllerian duct defects include agenesis and hypoplasia, lateral fusion defects, and vertical fusion defects with obstructed and nonobstructed variants.3,4 These anomalies are commonly concomitant to urinary tract anomalies in view of the close development of the urinary and reproductive tracts during embryogenesis. The Herlyn–Werner–Wunderlich syndrome, more recently called obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome, is a rare müllerian anomaly comprising uterine didelphys, obstructed hemivagina, and ipsilateral renal anomaly.5,6 It is a rare entity accounting for 0.16%–10% of all müllerian duct abnormalities that affects simultaneously the müllerian and metanephric ducts in the eighth gestation week. 7 The consequent female genital tract outflow obstruction leads to a retrograde tubal reflux that leads to an increased risk of endometriosis along with pelvic adhesions, pelvic inflammatory disease, and infertility.7,8 Based on the comprehensive new classification of the European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy, it is classified as U3b C2V2. 9 The surgical approach in the OHVIRA syndrome requires a two-step vaginoplasty particularly when the obstructed hemivagina reaches the hymeneal ring. The initial surgery drains the hematocolpos through a limited resection/marsupialization of the septum and insertion of a Foley's catheter. The second step requires the resection of the remaining septum after a period of wound healing and vaginal remodeling.10,11 A single-stage vaginoplasty is also supported by the contemporary literature. 11
The described techniques are usually done through the natural vaginal orifice, which often limit their implications in conservative societies where the anatomic integrity of the hymen is considered of social value.12,13 The ultrasound-guided hysteroscopic resection of the septum has been suggested to preserve the hymenal integrity. 14 However, the use of the vaginal orifice as a route for surgical procedures in virgin patients remains unacceptable. In this article we report a new hymen sparing surgical management of a vaginal septum that respects the hymen integrity.
The Surgical Technique
A 16-year-old girl was referred to our clinic for chronic pelvic pain and cyclic painful distension of the lower abdomen. Otherwise, her previous medical and surgical histories were unremarkable. Pubarche, thelarche, and menarche started, respectively, at 10, 11, and 12 years of age. Her family history was negative. Physical examination showed a normal stature lady with normal breasts, axillary and pubic hair development. No hirsutism, acne, or galactorrhea. Inspection of genital area showed normal external genitalia. The patient and her family insisted on respecting her virginity and refused the speculum examination and the bimanual pelvic examination as it would disrupt the hymen integrity. A digital rectal examination revealed a palpable soft mass occupying the vagina. The transabdominal ultrasound showed two uterine cavities, with fluid collection seen in the right one, a vaginal collection of 6 × 4 × 4 cm, and the absence of the right kidney. A pelvic magnetic resonance imaging showed anatomical features compatible with OHVIRA syndrome were found: a didelphic uterus along with a dilated right endometrial cavity contiguous with a right obstructed hemivagina. A normal left endometrial cavity and a left cervix were noticed. An exploratory laparoscopy and hysteroscopic resection of the septum through vaginal approach were offered to the patient. She was informed that her hymen integrity can be harmed during the procedure and a hymenal repair can be done directly after the termination of the intervention. She and her family absolutely refused the vaginal approach. We proposed thereafter a laparoscopy-assisted vaginal resection of the septum. The surgical inspection confirmed the presence of a didelphys uterus with a dilated right cavity along with normal adnexa and pelvic surfaces. A small posterior colpotomy was performed through which the obstructed hematocolpos was drained and washed. A fenestrated grasping atraumatic forceps was introduced to gently push the high vaginal septum downward reaching the hymenal ring from inside and making it accessible for a classical resection/marsupialization and insertion of a Foley's catheter without harming the hymen (Figs. 1 and 2). The vaginal defect was repaired with absorbable laparoscopic simple sutures. The postoperative course was uneventful and the patient was discharged without any complications 48 hours after the surgery.
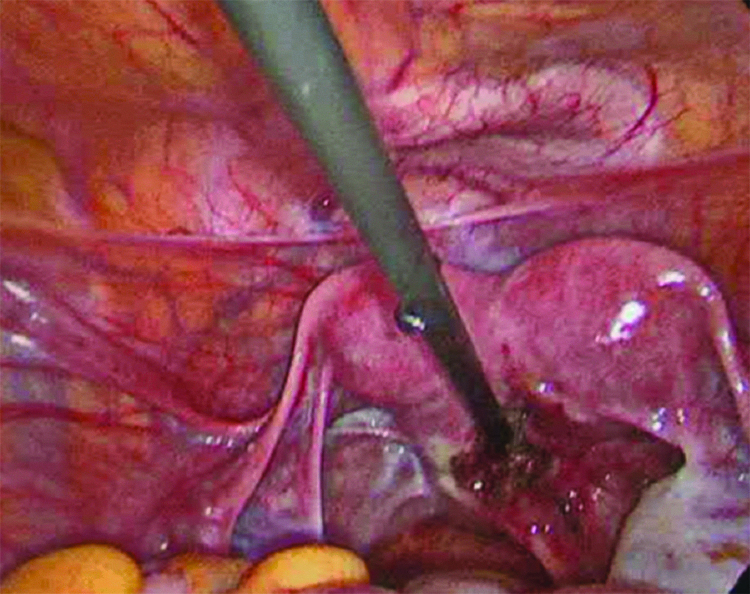
Fenestrated laparoscopic grasper introduced through posterior colpotomy.
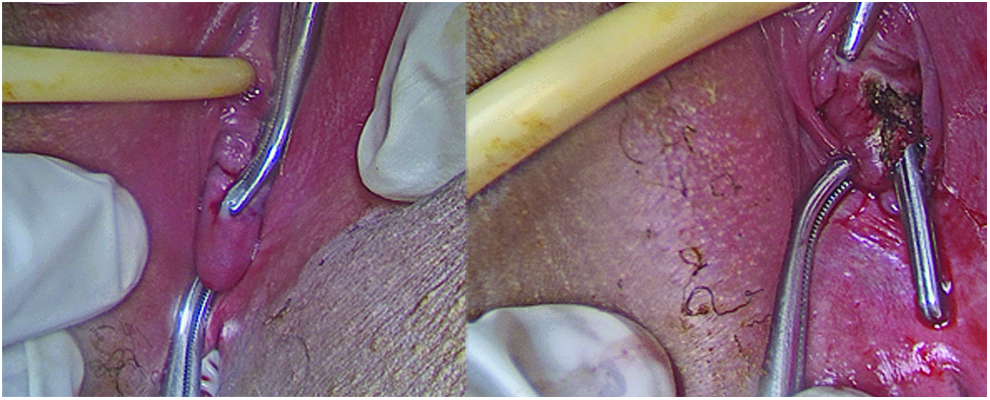
Laparoscopic grasper exposing the vaginal septum outside the hymenal ring (left side), excision of the septum taking the grasper as a landmark (right side).
Discussion
The conservation of an intact hymen has an undeniable social value in the conservative societies. The inability to confirm virginity on the wedding night may have serious social impact on women. 13 Consequently, surgical techniques requiring the use of medical instrument through the hymen in virgin women are unacceptable although the low risk of harming the hymenal integrity. It is a limiting and challenging factor for gynecologists in diagnosing and treating several illnesses. Other safe surgical alternatives, taking into consideration the patient desire and informed consent, should be considered. That is why we thought of “bringing” the high vaginal septum, to just behind the hymenal ring with a laparoscopic assistance. This made a classical resection/marsupialization, as an initial surgical procedure, possible without harming the hymenal integrity. Thus, symptoms are controlled, complications are prevented, and the remaining septum can be resected later on, after marriage, using a resectoscope through a vaginal access.
Classically, an exploratory laparotomy during which a probe passed through the uterine fundus to tent out a high transverse vaginal septum has been described. 2 It enables the surgeon to excise the septum from below and resect it safely. Nevertheless, a skilled laparoscopic surgeon can use a minimal invasive approach as a safe alternative to laparotomy with better outcomes such as a reduction in the postoperative pain and cosmetic injury, early ambulation, shorter hospital stay, and a rapid return to normal activities. 15 Social and cultural considerations can extend the indications of laparoscopy to profit from its benefits in treating vaginal pathologies. We reported the laparoscopic myomectomy through a posterior colpotomy for a cervicovaginal leiomyoma as a hymen conservative technique. 16 In this study, we describe a laparoscopy-assisted resection of a high vaginal septum in OHVIRA syndrome in a virgin lady.
In conclusion, the vaginal access remains the “gold standard” route in the management of vaginal septum. However, different factors such as septum position, anatomic obstacles, or patient's consideration regarding their hymenal integrity limit this approach. In the traditional conservative culture, the hymen ring injury during surgery should be prevented in any kind of intervention. As an alternative, our described procedure seems feasible when hymenal integrity matters. However, this approach requires adequate equipment and advanced laparoscopic surgical skills.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Disclosure Statement
Z.S. is a consultant for Karl Storz endoscope. He declares that his relation with the aforementioned company has no impact upon the scientific value and the content of the submitted. Remaining authors state no conflict of interest.