
Abstract
Abstract
Background:
Few studies have assessed the short- and long-term outcomes of laparoscopically assisted natural orifice specimen extraction (NOSE) in patients with sigmoid colon and rectal tumors. We investigated the short- and long-term outcomes of patients undergoing laparoscopic-assisted NOSE for tumors of the sigmoid colon and rectum.
Methods:
Ninety-eight patients with sigmoid colon and rectal tumors undergoing laparoscopic-assisted NOSE were included. The tumor was classified according to its distance from the anal verge: Group 1 (15–30 cm), Group 2 (5–15 cm), and Group 3 (≤5 cm). In Group 1 patients, a laparoscopic surgical specimen collection bag was used as a special transrectal device. In Group 2 patients, transanal endoscopic microsurgery device and specimen collection bag were used. In Group 3 patients, a Lone-Star retractor was used. The demographic characteristics and intra- and postoperative outcomes were measured.
Results:
In Group 1, 1 patient had respiratory disease and 1 had enterocolitis as short-term postoperative complications. One patient showed intestinal obstruction as a long-term postoperative complication. In Group 2, 2 patients had an ileus, 1 had an anastomotic leak, 2 had urinary retention, and 1 had respiratory disease as short-term complications. Only one patient had a long-term complication: anastomotic stenosis. In Group 3, short-term complications were present in 3 patients: 1 had hemorrhage, 1 had urinary retention, and 1 had respiratory disease. Long-term complications included one case of anastomotic stenosis and one of intestinal obstruction.
Conclusions:
NOSE is safe and cosmetically and theoretically superior to conventional laparoscopy when different devices are used according to the tumor's location.
Introduction
Although several reports1,2 have described the results of pure colon resection (natural orifice transluminal endoscopic [NOTE] surgery), currently, a hybrid technique using laparoscopic surgery with a transvaginal 3 or transanal approach4,5 to excise the specimen seems to be more accepted than other techniques in the field of colorectal surgery.
The first description of a completely laparoscopic total mesorectal excision (TME) with transanal extraction of the specimen, combined with the creation of a colonic J-pouch and coloanal anastomosis, was reported in 2006 by Person et al. 6 Currently, different colorectal surgery surgeons have used the natural orifice specimen extraction (NOSE) approach assisted by laparoscopy through the anus to treat sigmoid and rectal cancer.7,8 Compared with transvaginal and transgastric approaches, NOSE, which incorporates the abdominal and transanal approaches, is a more suitable route than others. Transrectal NOSE has been accepted as a laparoscopy-assisted hybrid procedure that allows for pure access to resect rectal and colonic specimens without using a special abdominal incision. Reports9,10 demonstrated that NOSE is a safe and reproducible procedure and does not negatively impact the oncological dissection or functional outcomes. Our group 11 has also found that transanal NOSE rectosigmoid resection that is assisted by laparoscopy has good outcomes.
In this series, we evaluated the safety and feasibility of NOSE using different methods according to the location of tumors of the sigmoid colon and rectum. We also retrospectively investigated the short- and long-term outcomes of patients who underwent laparoscopy with NOSE for these tumors in our surgical center.
Materials and Methods
Inclusion and exclusion criteria
The inclusion criteria were simplified in this study as follows: (1) tumor in the rectum or sigmoid colon with a diameter ≥1 cm, but ≤4 cm; (2) local spread that was restricted to the sigmoid or rectal wall (T1–T3), as determined with preoperative computed tomography, magnetic resonance imaging, or endorectal ultrasonography for cancer in the sigmoid colon and upper rectum, and local spread that was restricted to the internal sphincter (T1/T2) in patients with lower rectal cancer. The exclusion criteria were as follows: (1) patients with a history of pelvic operation; (2) tumor diameter >4 cm, which is the diameter of the transanal endoscopic microsurgery (TEM) resectoscope shaft and is difficult for sample extraction; and (3) tumors located ≥30 cm from the anal verge, which are difficult for achieving a transanal end-to-end anastomosis using a circular stapler.
Patients
This retrospective study involved 98 patients who underwent laparoscopy-assisted NOSE for sigmoid or rectal tumors between January 2012 and December 2017. All of the patients provided written informed consent. The study was approved by the ethics committees of our institutions (SHSY-IEC-pap-18-2). Data on the patients' demographic and clinical characteristics, surgical outcomes, and postoperative outcomes were obtained from the databases of the hospitals (Shanghai Ruijin Hospital and Shanghai Tenth People's Hospital). The demographic characteristics included patient age, sex, American Society of Anesthesiologists physical status score, and history of abdominal surgery. The tumor characteristics included the number of tumors and location (distance from the anal verge). Patients were classified according to the location of their tumors: Group 1 (15–30 cm), Group 2 (5–15 cm), and Group 3 (≤5 cm).
Procedures
All patients first underwent laparoscopy. Laparoscopy for sigmoid colon and rectal tumors involved four ports and included laparoscopic tumor-specific mesorectal excision and TME. The level of ligation of the inferior mesenteric artery was based on preoperative diagnostic images. Surgical resection was proposed to all of the patients with clinically resectable liver metastases.
We used an anastomosis with special transrectal and transanal devices during reconstruction to treat the tumors based on their location. These methods were as follows: in patients in Group 1, for tumors in the sigmoid colon and upper rectum, the proximal and distal bowel was resected transversely about 10 cm from the tumor using a Harmonic Scalpel, and a specimen was directly extracted through the rectum in a specimen bag (Type HSD 100; Guangzhou T.K. Medical Instrument Co. Ltd., Guangzhou, China) (Fig. 1A, B). The anvil of a circular stapler was then inserted into the abdominal cavity through the stump of the rectum, and purse string sutures were made circumferentially at the proximal end of the bowel. The anvil was inserted into it laparoscopically. The distal stump was clamped using an Endo GIA stapler, after which a circular stapler was inserted transanally, and an end-to-end anastomosis was created.

The procedure of specimen extraction after laparoscopic tumor-specific mesorectal excision and TME.
In patients in Group 2, for tumors in the middle rectum, the proximal bowel was resected transversely about 10 cm from the tumor using a Harmonic Scalpel. The distal rectum was resected at least 2 cm from the tumor using a TEM device. The sample was carefully packed into a specimen bag and extracted through the TEM resectoscope's shaft. The anvil of a circular stapler was then inserted into the abdominal cavity, and the distal stump was closed using an Endo GIA stapler. Afterward, an end-to-end anastomosis was performed, as in patients in Group 1.
In patients in Group 3, for tumors in the lower rectum, the anal canal was adequately exposed using a Lone-Star retractor. The distal rectum was resected at least 2 cm from the tumor using an electrotome. Then, the mobilized rectum was delivered through the anal canal. The mesentery was further transected at the level of the upper lymphadenectomy. The proximal rectum was transected about 10 cm from the tumor using the electrotome. Afterward, the rectum was gently reduced back into the pelvis, and a hand-sewn end-to-end anastomosis was created (Fig. 2). In patients with ultralow rectal cancer that was ∼2 cm within the dentate line, a circumferential, hand-sewn end-to-end anastomosis was created after the partial intersphincteric resection technique was performed. After all procedures, every patient in three groups was placed with a tube through anus across the anastomosis and an intraoperative air leak test was taken to make sure that there was no leakage.
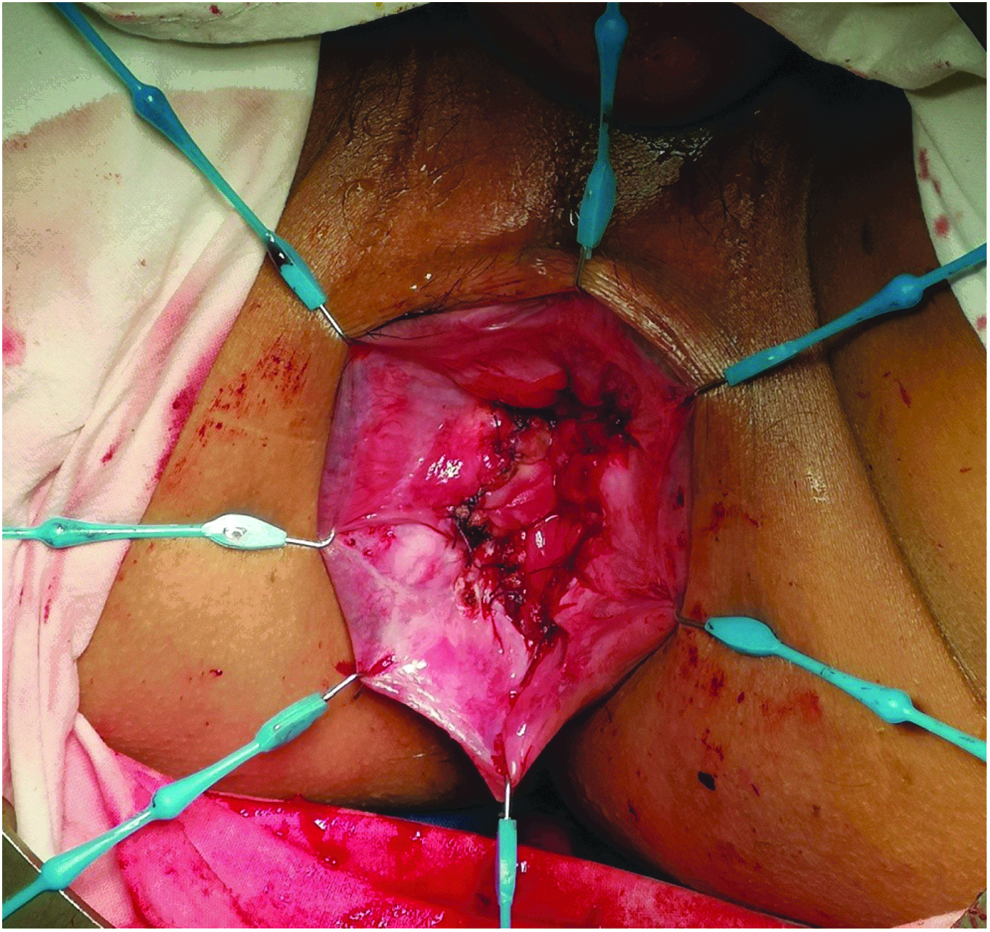
A hand-sewn end-to-end anastomosis was created.
Data collection
The tumors were classified by their location, and the surgical outcomes included the operating time, estimated blood loss, splenic flexure mobilization, combined surgery, distal resection margin, radicality, performance of diverting ileostomy, and intraoperative complications. The clinicopathological features included histology, differentiation, the maximum tumor diameter, number of retrieved lymph nodes, neurovascular invasion, and pathological stage according to the Union for International Cancer Control guideline, 7th edition. The postoperative outcomes included the time to first flatus, time to solid diet, postoperative hospital stay, readmission after discharge, and postoperative complications. Long-term outcomes, including the complication and 3-year overall survival rates, were determined at follow-up in the patients who underwent surgery between 2012 and 2017.
Statistical analysis
Quantitative data are expressed as mean or median (range). Survival outcomes were determined using the Kaplan–Meier method and compared using the log-rank test. The data were assessed using the SPSS 22 statistical analysis program (SPSS, Inc., Chicago, IL).
Results
The patients' overall demographic
The overall demographic information and operative characteristics of the patients in this study are presented in Table 1. The median age of the 98 included sigmoid and rectal tumor patients was 58 years (range, 42–81 years), and 61 (62.2%) were men. Sixteen patients (16.3%) have history of abdominal surgery. Thirty-six tumors (36.7%) were located in sigmoid colon, and distance from anal edge was 15–30 cm (Group 1). Forty-three (43.9%) tumors located in rectum were 5–15 cm (Group 2) from the anal verge. Nineteen (19.4%) tumors located in rectum were <5 cm (Group 3) from the anal verge. Ninety-two patients (93.9%) were single tumor, and 6 (6.1%) patients were more than two (range two to six) tumors.
Demographic and Preoperative Information of All Patients
BMI, body mass index.
Patients' operative characteristics
The operative characteristics of these patients are presented in Table 2. Group 1 used laparoscopic surgical specimen collection bag as transrectal special device, Group 2 used TEM system, and Group 3 used Lone-Star Retractor system. Anal preservation was achieved in all. Compared between groups, operative time and estimated blood loss of Group 1 were significantly shorter and less than other Groups (P < .01). All of Group 1 and 2 patients underwent circular stapler anastomosis, then all Group 3 patients hand-sewn anastomosis. Overall, 5 patients performed simultaneous part liver resection because of hepatic metastasis. No distal resection margin was positive. Compared between groups, the length of the distal resection margin in Group 3 was significantly shorter than the other two groups (P < .01). The length of the distal resection margin in Group 2 was longer than Group 3, but shorter than Group 1 (P < .01). There are 5 patients who performed R1 resection because of the metastases to liver or lung. Compared with other groups, Group 3 has more patients who performed ileostomy (P < .01), and we closed the diverting stoma in 3–6 months after the surgery. Only 1 patient (2.3%) in Group 2 conversed to open surgery because of intraoperative bleeding.
Operative Characteristics of the Patients in This Study
P < .01 compared with Groups 2 and 3.
P < .01 compared with Groups 1 and 3.
P < .01 compared with Groups 1 and 2.
TEM, transanal endoscopic microsurgery.
Pathological features
The pathological characteristics of the patients in this study appear in Table 3. In Group 1, histology of all patients was adenocarcinoma. Differentiation well was present in 6 (16.7%) patients, moderate was 18 (50%), and poor was 12 (33.3%). Median maximum tumor diameter was 1.7 cm (range from 1.0 to 4.2). Median number of retrieved lymph nodes was 12.8 (range from 8 to 21). Neurovascular invasion was present in 4 (11.1%) patients. TNM stage I was shown in 3 (8.3%) patients, IIa/IIb was 8 (22.2%)/5 (13.8%), IIIa/IIIb was 9 (25.0%)/7 (19.4%), IV was 2 (5.6%), and Tis was 2 (5.6%).
Pathological Characteristics of the Patients in This Study
GIST, gastrointestinal stromal tumor.
In Group 2, 41 (95.3%) patients were adenocarcinoma, and 2 (4.7%) patients were gastrointestinal stromal tumor (GIST). Differentiation well was present in 5 (11.6%) patients, moderate was 24 (55.8%), and poor was 14 (32.6%). Median maximum tumor diameter was 2.01 cm (range from 0.5 to 4.5). Median number of retrieved lymph nodes was 15.1 (range from 10 to 26). Neurovascular invasion was present in 5 (12.2%) patients. Adenocarcinoma TNM stage I was shown in 4 (9.8%) patients, IIa/IIb was 6 (14.6%)/8 (19.5%), IIIa/IIIb was 8 (19.5%)/10 (23.3%), IV was 4 (9.8%), and Tis was 1 (2.3%).
In Group 3, 16 (84.2%) patients were adenocarcinoma, 2 (10.5%) patients were GIST, and 1 (5.3%) patient was neuroendocrine tumor. Differentiation well was present in 4 (21.1%) patients, moderate was 8 (42.1%), and poor was 7 (36.8%). Median maximum tumor diameter was 1.43 cm (range from 1.0 to 4.0). Median number of retrieved lymph nodes was 13.4 (range from 7 to 32). Neurovascular invasion was present in 3 (15.8%) patients. Adenocarcinoma TNM stage I was shown in 2 (12.5%) patients, IIa/IIb was 3 (18.8%)/2 (12.5%), IIIa/IIIb was 4 (25.0%)/2 (12.5%), IV was 2 (12.5%), and Tis was 1 (6.3%).
Postoperative short- and long-term outcomes
The postoperative outcomes of the patients in this study are present in Table 4. Compared with other groups, all short-term postoperative complications in Group 1 were significantly less than other groups (P < .01). In this study, no patient had occurrence of postoperative pelvic abscess and mortality. For cumulative survival of patients in three groups, there were no differences among them (P = .607) (Fig. 3). In Group 1, the median follow-up period of the 27 patients who underwent surgery between 2012 and 2017 was 33 months (range: 3–64 months). Their 3- and 5-year overall survival rate was 96.3% and 77.4%. Two patients died in the follow-up period. One patient died of primary lung cancer; the other died of liver metastasis. In Group 2, the median follow-up period of the 33 patients was 28 months (range: 1–64 months). Their 3- and 5-year overall survival rate was 93.9% and 73.6%. Four patients died in the follow-up period. One patient died of heart disease, 2 died of a liver or lung metastasis, and 1 died accidentally. In Group 3, the median follow-up period of the 14 patients was 31.5 months (range: 6–62 months). Their 3- and 5-year overall survival rate was 92.9% and 66.7%. Two patients died in the follow-up period. One patient died of liver and lung metastases, and the other died of cerebral infarction.

The cumulative survival of patients in three groups.
Postoperative Outcomes
P < .01 compared with the other groups.
Discussion
Laparoscopic surgery has become widely accepted as a minimally invasive surgery. To maintain the advantages of laparoscopy and reduce wound-related complications, the NOSE method was developed. This technique does not involve an abdominal incision, and it is expected to be developed in the future. 12 Recently, multiple researchers have reported removing colorectal specimens transvaginally and transanally.13–15 NOSE for mid- and upper rectal cancer had safe and acceptable long-term oncologic outcomes comparable to those of conventional minimal invasive surgery and seems to be an alternative to reduce access trauma. 16 In this study, we have successfully performed complete laparoscopic resection using the NOSE method to extract specimens from the sigmoid colon and rectal tumor transrectally and transanally. Based on our experience, we believe that the best indication for surgery is a tumor with a volume around 4 cm that is located in the rectosigmoid segment, and the length of the sigmoid colon should have sufficient margins. However, if the tumor is not large enough to be detected with laparoscopy intracorporeally, fibro-colonoscopy should be used to mark the tumor's location. As shown in a previous study, 17 the NOSE technique does not require an additional incision in the abdomen, has excellent cosmetic properties, and is associated with a significantly lower frequency of postoperative analgesic usage and shorter postoperative pain period than other techniques.
For NOSE, few studies have described the transvaginal technique regarding its potential to decrease the incidence of surgical wound-related complications, particularly those associated with a gynecological procedure.7,18 Currently, many reports have evaluated the transrectal and transanal methods, including procedures to transanally remove specimens and achieve a colorectal anastomosis.19,20 However, none of these techniques has been standardized. Simultaneously, various techniques exist mostly for preventing intraoperative infections and tumor implantation after laparoscopic anterior resection. 21
Depending on the location of the tumor, we used three different experiential methods to resect the colon and rectum, remove the specimen, and perform colorectal and coloanal anastomosis. Wolthuis et al. 22 similarly reported that in patients with a tumor located more than 15 cm from the anal edge, a specimen bag was inserted transrectally to withdraw the sigmoid colon tumor. However, the resected specimen may become folded in the bag. If the diameter of the specimen is larger compared with the rectum, the residual rectum or the anus may be damaged. To solve this problem, all of the tumors' diameters were measured preoperatively at our center. Afterward, the anal sphincter function was not negatively impacted by transanal extraction. We also used 1-0 thread to close the tumor toward the anal side, as reported before. 23 After all of the specimens were put into the bag, except for the thread, we drew the bag's head out of the anus. Thereby, with the help of the thread, the specimen was removed longitudinally against the rectal stump, leading to easy extraction. Subsequently, the anvil of a circular stapler is inserted into the abdominal cavity transrectally. Purse string suturing of the proximal end of the bowel is performed to fix the anvil under laparoscopic guidance. 24 Then, an end-to-end anastomosis is created, after stapling the distal stump of the rectum with an Endo GIA stapler.
In 2013, our surgical group described a technique for rectal surgery combined with TEM to extract the specimen and achieve an anastomosis. 11 After more practice, we created a standard technique for NOSE that is combined with TEM when tumors are located within 5–15 cm of the anal edge. We found that TEM transection of the distal margin is better under direct vision, improving our ability to find and access tumors that are located in the middle of the rectum with superior visualization. Furthermore, the rates of negative margins are increased, fragmentation of specimens is decreased, and recurrence rates are lower. 25 In this study, after the specimen was extracted through the shaft of the TEM resectoscope in a specimen bag, the anvil was fixed intraperitoneally. Then, the distal rectal stump was closed using an Endo GIA stapler, as described. Finally, an end-to-end anastomosis was created.
Transanal extraction of the specimen and creation of an intracorporeal anastomosis using a double stapling technique have been described. 23 However, this procedure has some limitations for tumors located in the ultralow rectum, because it is difficult to determine the distal surgical margin during laparoscopy and transect the rectum too close to the anal sphincter. To eliminate those drawbacks, in our center, if the tumor is located within 5 cm of the anal edge, a Lone-Star retractor is applied to enlarge the anus. Afterward, the distal resection margin (usually at least 2 cm distal to the tumor) was identified clearly. We believe that it is the most suitable technique for tumors that are close to the dentate line. With complete mobilization of the sigmoid colon and rectum, the transected rectum transanally was pulled out continuously, and the proximal tumor margin was divided, with an adequate colonic and mesenteric length. Finally, the proximal rectal stump was hand-sewn to achieve an anastomosis to the rectal stalk or directly to the anal dentate line. The advantage of this technique is that it guarantees coloanal anastomosis with transection of the negative margin of rectal cancer and that it allows for removal of the specimen through the anus without using an abdominal incision.
A previous study 26 confirmed that the infection rates following transanal NOSE and transabdominal colorectal resection were equivalent. Others stated that rectal irrigation of the anus with normal saline containing povidone-iodine reduced the risk of infection. 27 A prospective study 28 found that there were no infectious complications such as diverticulitis after the extraction of transanal specimens. To prevent intraoperative infections and tumor cell implantation, we believe the bowel should be irrigated with normal saline before opening it, and the intraperitoneal space should be flushed with distilled water before and after the anastomosis is created. This may effectively decrease the risk of infection and implantation. In fact, pathogenic bacteria were not detected in the intraperitoneum in our patients after they underwent irrigation with 2000 mL of fluid. Moreover, similar to other reports,29,30 we covered the resected bowel with a specimen bag intraperitoneally to further reduce the risk of tumor implantation or local recurrence. Another study 9 reported that the early bacteriological, oncological, and functional results indicated that NOSE is safe and feasible in patients with colorectal cancer. However, follow-up is required to establish the long-term oncological outcome.
Another study 31 found that regarding the operation time, bleeding volume, postoperative wound pain, postoperative hospital stay, the number of totally dissected lymph nodes, and postoperative complications, there were no significant differences between the NOSE method and conventional laparoscopic surgery, indicating that NOSE has a similar result as conventional laparoscopic surgery. 14 Furthermore, a significant improvement was shown in the patient's quality of life at the 6-month follow-up interval, based on the patients'self-report. 25 In this study, the short-term postoperative complications included urinary retention, respiratory problems, and enterocolitis, which were conservatively mitigated. Regarding the long-term postoperative complications, 2 patients had intestinal obstruction and recovered with conservative management, and 2 other patients had anastomotic stenosis close to the anus that was cured with finger enlargement. The 3-year overall survival rates in our patients were 96.3% in Group 1, 93.9% in Group 2, and 92.9% in Group 3; none of these patients experienced locoregional recurrence. These findings indicate that the safety and short- and long-term outcomes of laparoscopy-assisted NOSE for sigmoid colon and rectal tumor resection are comparable or superior to those of conventional laparoscopic surgery in these patients.
Therefore, different NOSE techniques should be accepted as novel, minimally invasive techniques for treating rectosigmoid tumors in several conditions. 32 Overall based on these NOSE studies, transrectal and transanal extractions of colorectal resection specimens appear to be safe, are associated with reduced pain and a shorter length of hospital stay, and offer at least the cosmetic benefit of eliminating the incision at the extraction site. Therefore, this is an alternative treatment option for selected patients to facilitate colorectal resection and anvil placement, avoiding additional abdominal incisions.
However, the limitation of this study is that we did not assess specimen damage after extraction and not perform a comparative analysis of laparoscopy-assisted NOSE and laparoscopic outcomes. Moreover, a further study may enable more patients to benefit from this laparoscopy-assisted NOSE technique. We concluded that treating these selected rectosigmoid tumors is safe and feasible, without a notable increase in inoperative difficulty when using NOSE technique.
Conclusion
Different NOSE techniques according to the location of the rectosigmoid tumor appear to be safe and theoretically superior to conventional laparoscopy regarding reduced wound complications and postoperative pain, yielding favorable short- and long-term outcomes. It is a new surgical strategy to bridge conventional laparoscopic surgery with pure human NOTE procedures. However, this technique should only be performed in selected patients and should be further evaluated in large, prospective controlled trials.
Footnotes
Acknowledgments
The authors thank Dr. Shukun Fu and Ms. Yu Ruan for their participation in the operation. Sources of funding: (1) Supported by 350 clinical research support fund of Shanghai Tenth People's Hospital. (2) Shanghai Municipal Planning Commission of Science and Research Fund (201540382).
Disclosure Statement
All authors have no competing financial interests that exist.