
Abstract
Abstract
Objective:
The aim of this study was to investigate the long-term efficacy of laparoscopic radiofrequency ablation (LRFA) in early hepatocellular carcinoma (HCC) compared with other surgical procedures.
Methods:
A literature search of Cochrane library, PubMed, and Embase through October 2018 was conducted by two investigators (J.-F.G. and F.Y.) independently. The quality of included studies was estimated by the Newcastle–Ottawa Scale. Review Manager 5.3 software was used for meta-analysis, and either fixed- or random-effects model was used according to the heterogeneity of included studies. The chi-square test was used for heterogeneity analysis of included studies, and subgroup analysis was conducted to estimate the heterogeneity between each study and also to estimate the efficacy of different studies.
Results:
A total of 11 studies involving 1691 patients were included in this analysis. Patients undergoing hepatic resection (HR) had higher 3-, 5-year overall survival rate, 3-year disease-free survival rate, and lower local recurrence rate than those undergoing LRFA. However, patients undergoing LRFA had higher 3-, 5-year overall survival rate than those undergoing other minimally invasive ablation, although there was no statistical difference in local recurrence rate or disease-free survival rate.
Conclusion:
HR is still an ideal choice for early HCC. If minimally invasive ablation is an alternative treatment, LRFA will be better than other minimally invasive options.
Introduction
Hepatocellular carcinoma (HCC) is a common malignant tumor and the second cause of cancer death around the world. 1 Treatment options for HCC currently include liver transplantation, hepatic resection (HR), local ablation, transarterial chemoembolization, and drug therapy. 2 Liver transplantation is regarded as an ideal choice for patients with early stages of HCC; yet, it is significantly limited by organ shortage. According to the Barcelona Clinic Liver Cancer (BCLC) system, early HCC (BCLC 0 or A) should be treated with resection or local ablation. 3 Several studies have compared the curative effects of radiofrequency ablation (RFA) and HR, but there are some controversies regarding which modality provides the best outcomes.4,5 Laparoscopic radiofrequency ablation (LRFA) has the advantages of direct controlling of operation and exposing the tumor lesions missed by surface ultrasound imaging.6,7 It may be regarded as an alternative ablation method to percutaneous RFA. There are some studies that observed the clinical effect of LRFA in early HCC compared with other surgical procedures.8,9 But the sample size of these studies was small, and its evaluation was controversial. Therefore, this meta-analysis aimed to evaluate the long-term efficacy of LRFA in early HCC.
Materials and Methods
Search strategy
This meta-analysis was conducted according to the Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA). 10 Two investigators (J.-F.G. and F.Y.) independently conducted a systematic literature searching of Cochrane library, PubMed, and Embase through October 2018. The keywords “hepatocellular carcinoma,” “liver cancer,” “hepatic cancer,” and “laparoscopic radiofrequency ablation” were used. Tracing the references included in the studies was done to obtain the relevant literature that was not found.
Inclusion and exclusion criteria
Inclusion criteria for this meta-analysis were as follows: (1) patients involved in studies were clearly diagnosed with very early or early HCC according to the BCLC criteria 3 ; (2) the major therapeutic option was LRFA or other surgery; (3) none of the patients had contraindication for LRFA and/or other surgery; (4) if multiple studies were reported by the same author, they can also be included in this meta-analysis as long as they were not at the same research; (5) prospective cohort studies or retrospective cohort studies.
Exclusion criteria were as follows: (1) animal studies, reviews, case reports, and incomplete studies; (2) incomplete or obvious defects in the test data.
Data extraction and quality assessment
The studies screening was independently conducted by two investigators (J.-F.G. and F.Y.) through reading and selecting the subject, then reading the abstract and the full text. The basic information including first author, publication date, country, mean duration of follow-up, general situations, disease characteristics, local recurrence, overall survival data, and disease-free survival data was collected. The quality of included studies was independently evaluated according to the Newcastle–Ottawa Scale by two investigators (J.-F.G. and F.Y.). 11 Each research could get a maximum of nine stars (six or more stars were considered as high quality) after the evaluation of three broad categories: selection, comparability, and outcome. If any disagreement in regard to data extraction and quality assessment was expressed, it was resolved through detailed discussion.
Statistical analysis
The meta-analysis was performed by Review Manager 5.3, provided by Cochrane Collaboration (The Nordic Cochrane Centre, Copenhagen, Denmark). Continuous data and dichotomous data were analyzed by calculating standard mean difference and risk ratio (RR) with 95% confidence interval (95% CI). Survival data were analyzed by calculating hazard ratio with 95% CI and standard error. The heterogeneity of included studies was evaluated by the chi-square (χ 2 ) and I2 statistic. If heterogeneity differences among these studies were not statistically significant (I2 ≤ 50%, P > .05), fixed-effects model was chosen; otherwise, random-effects model was chosen. Sensitivity analysis was performed to examine the influence of individual study with significant heterogeneity (I2 ≥ 75%) on the pooled estimates. There may be some differences in the results because of different surgical procedures (HR and minimally invasive ablation). Therefore, subgroup analysis was performed to identify the efficacy of “LRFA versus RFA” and “LRFA versus HR.” Probability value P < .05 was deemed to statistical significance.
Results
Literature search
A total of 343 studies were searched. After excluding duplicate studies and screening the title and abstract, 45 studies remained. After reviewing the full text, 11 studies12–22 were considered to meet the inclusion criteria (Fig. 1).
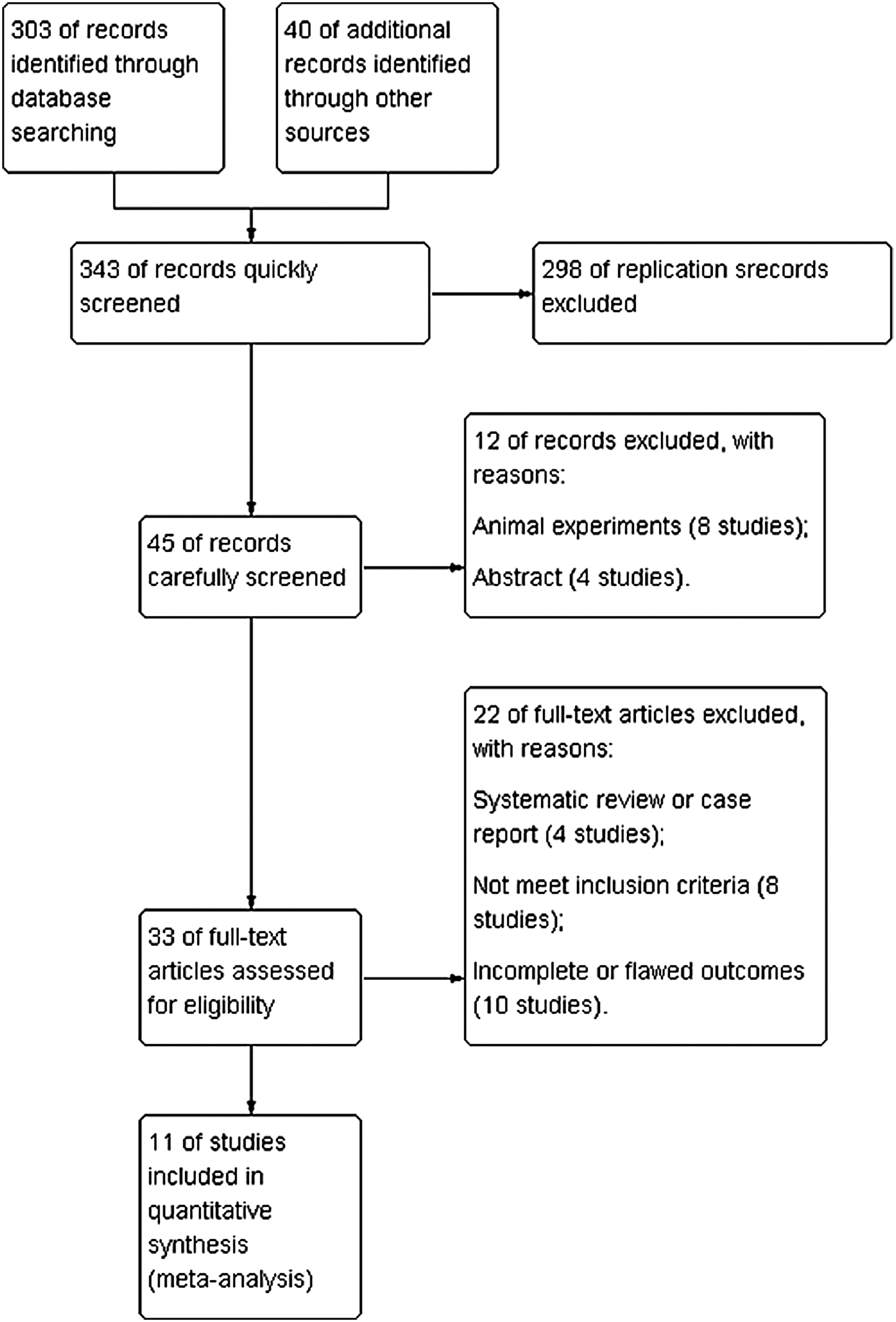
Flow chart of identified studies.
Study characteristics and quality
The basic characteristics of included studies are shown in Table 1. These studies were published from 2009 21 to 2018, 22 including 1691 patients (861 patients in the experimental groups and 830 patients in the control groups).
Baseline Characteristics of the Patients in the 11 Included Studies
CT-RFA, computed tomography-guided radiofrequency ablation; DFSR, disease-free survival rate; E/C, experimental/control group; HR, hepatic resection; LMWA, laparoscopic microwave ablation; LRFA, laparoscopic radiofrequency ablation; LRR, local recurrence rate; M/F, male/female; NR, not report; OSR, overall survival rate; PRFA, percutaneous radiofrequency ablation; TACE, transcatheter arterial chemoembolization.
Each research could get a maximum of nine stars (four stars of Selection, two stars of Comparability, and three stars of Outcome), and six or more stars were considered as high quality. The quality of included studies was generally fine, with 10 studies being of high quality. Details of these studies are shown in Table 2.
Quality Assessment of the 11 Included Studies Based on the Modified Newcastle-Ottawa Scale Criteria
Matched in: 1, demographic data; 2, size of primary tumor; 3, number of primary tumors; 4, HBs-Ag positive; 5, Childe-Pugh class; 6, Barcelona Clinic Liver Cancer stage; 7, cirrhosis; 8, serum AFP level.
AFP, alpha fetoprotein.
Meta-analysis results
Local recurrence rate
The meta-analysis on the local recurrence rate included 10 cohorts,12,14–22 involving 1515 patients (765 patients in experimental group and 750 patients in control group). The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” represented obvious heterogeneity (I2 = 63%, P = .07; I2 = 72%, P < .01), and random-effects model was used in analysis. Test for subgroup differences represented that different surgical procedures did not obviously affect the result (I2 = 24%, P = .25). The pooled results showed that the local recurrence rate of experimental group was higher than that of control group (RR = 1.32, 95% CI [1.01–1.73], P = .04). The subgroup analysis results showed that the difference of local recurrence rate in “LRFA versus HR” between experimental group and control group was not statistically significant (RR = 1.05, 95% CI [0.64–1.71], P = .85), and the local recurrence rate of experimental group was higher than that of control group in “LRFA versus HR” (RR = 1.48, 95% CI [1.06–2.08], P = .02) (Fig. 2).

Forest plot of local recurrence rate between the experimental group and control group.
Disease-free survival rate
All the eight included studies involving 982 patients (445 patients in experimental group and 537 patients in control group) reported 1-, 3-, and 5-year disease-free survival data.12–14,16–20
One-year disease-free survival rate
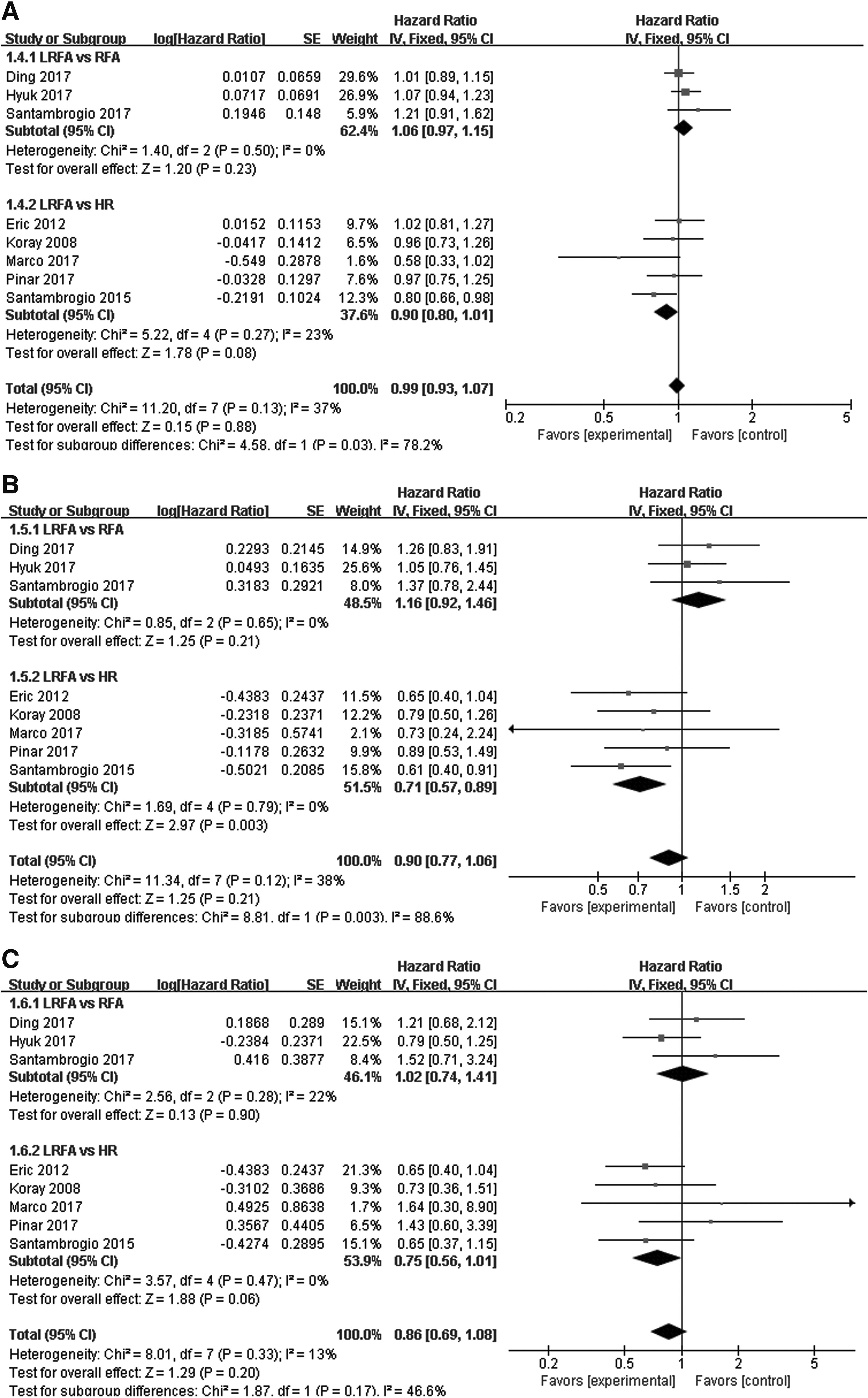
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 0%, P = .50; I2 = 23%, P = .27), and fixed-effects model was used in analysis. Test for subgroup differences represented that heterogeneity between subgroups may result from different surgical procedures (I2 = 78%, P = .03). The pooled results showed that the difference in 1-year disease-free survival rate between experimental group and control group was not statistically significant (hazard ratio = 0.99, 95% CI [0.93–1.07], P = .88). The subgroup analysis results showed that there was no statistical difference between experimental group and control group whether in “LRFA versus RFA” (hazard ratio = 1.06, 95% CI [0.97–1.15], P = .23) or “LRFA versus HR” (hazard ratio = 0.90, 95% CI [0.80–1.01], P = .08) (Fig. 3A).
Forest plot of
Three-year disease-free survival rate
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 0%, P = .65; I2 = 0%, P = .79), and fixed-effects model was used in analysis. Test for subgroup differences represented that heterogeneity between subgroups may result from different surgical procedures (I2 = 89%, P < .01). The pooled results showed that the difference in 3-year disease-free survival rate between experimental group and control group was not statistically significant (hazard ratio = 0.90, 95% CI [0.77–1.06], P = .21). The subgroup analysis results showed that there was no statistical difference between experimental group and control group in “LRFA versus RFA” (hazard ratio = 1.16, 95% CI [0.92–1.46], P = .21), but the 3-year disease-free survival rate of experimental group was lower than that of control group in “LRFA versus HR” (hazard ratio = 0.71, 95% CI [0.57–0.89], P < .01) (Fig. 3B).
Five-year disease-free survival rate
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 22%, P = .28; I2 = 0%, P = .47), and fixed-effects model was used in analysis. Test for subgroup differences represented that different surgical procedures did not obviously affect the result (I2 = 47%, P = .17). The pooled results showed that the difference in 5-year disease-free survival rate between experimental group and control group was not statistically significant (hazard ratio = 0.86, 95% CI [0.69–1.08], P = .17). The subgroup analysis results showed that there was no statistical difference between experimental group and control group whether in “LRFA versus RFA” (hazard ratio = 1.02, 95% CI [0.74–1.41], P = .90) or “LRFA versus HR” (hazard ratio = 0.75, 95% CI [0.56–1.01], P = .06) (Fig. 3C).
Overall survival rate
All the 10 included studies involving 1549 patients (780 patients in experimental group and 769 patients in control group) reported 1-, 3-, and 5-year overall survival data.12–17,19–22
One-year overall survival rate
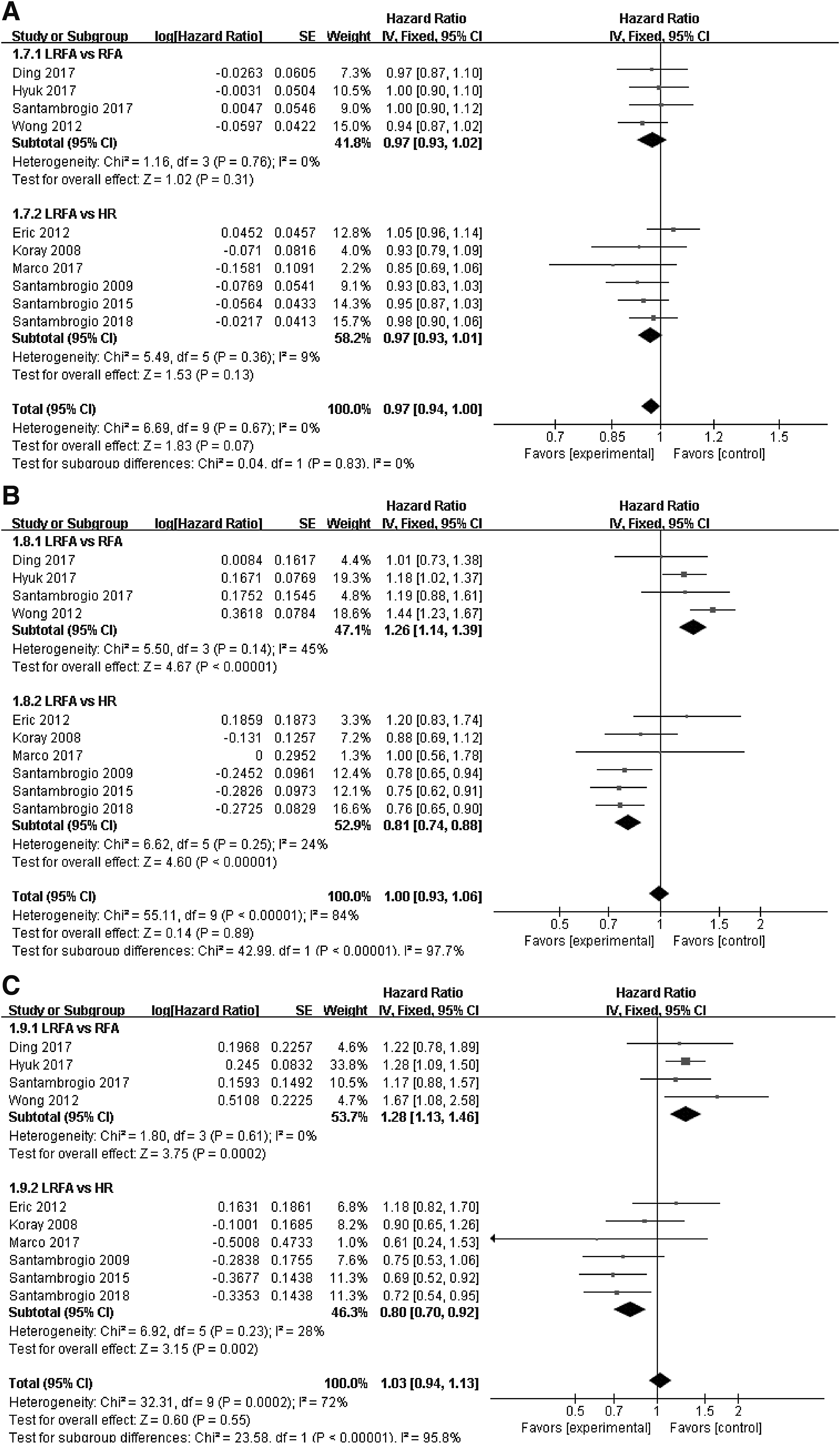
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 0%, P = .76; I2 = 9%, P = .36), and fixed-effects model was used in analysis. Test for subgroup differences represented that different surgical procedures did not obviously affect the result (I2 = 0%, P = .83). The pooled results showed that the difference in 1-year overall survival rate between experimental group and control group was not statistically significant (hazard ratio = 0.97, 95% CI [0.94–1.00], P = .07). The subgroup analysis results showed that there was no statistical difference between experimental group and control group whether in “LRFA versus RFA” (hazard ratio = 0.97, 95% CI [0.93–1.02], P = .31) or “LRFA versus HR” (hazard ratio = 0.97, 95% CI [0.93–1.01], P = .13) (Fig. 4A).
Forest plot of
Three-year overall survival rate
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 45%, P = .14; I2 = 24%, P = .25), and fixed-effects model was used in analysis. Test for subgroup differences represented that heterogeneity between subgroups may result from different surgical procedures (I2 = 98%, P < .01). The pooled results showed that the difference in 3-year overall survival rate between experimental group and control group was not statistically significant (hazard ratio = 1.00, 95% CI [0.93–1.06], P = .89). The subgroup analysis results showed that the 3-year overall survival rate of experimental group was higher than that of control group in “LRFA versus RFA” (hazard ratio = 1.26, 95% CI [1.14–1.39], P < .01), but the 3-year overall survival rate of experimental group was lower than that of control group in “LRFA versus HR” (hazard ratio = 0.81, 95% CI [0.74–0.88], P < .01) (Fig. 4B).
Five-year overall survival rate
The heterogeneity test in both “LRFA versus RFA” and “LRFA versus HR” showed that there was no statistical difference (I2 = 0%, P = .61; I2 = 28%, P = .23), and fixed-effects model was used in analysis. Test for subgroup differences represented that heterogeneity between subgroups may result from different surgical procedures (I2 = 96%, P < .01). The pooled results showed that the difference in 5-year overall survival rate between experimental group and control group was not statistically significant (hazard ratio = 1.03, 95% CI [0.94–1.13], P = .55). The subgroup analysis results showed that the 5-year overall survival rate of experimental group was higher than that of control group in “LRFA versus RFA” (hazard ratio = 1.28, 95% CI [1.13–1.46], P < .01), but the 5-year overall survival rate of experimental group was lower than that of control group in “LRFA versus HR” (hazard ratio = 0.80, 95% CI [0.70–0.92], P < .01) (Fig. 4C).
Publication bias
Because of the less number of included studies, publication bias analysis may result in low test efficiency, which had not been carried out. 23
Discussion
In recent studies, RFA was a valid alternative treatment for early HCC with comparable results with HR in selected patients.24,25 With the wide application of laparoscopic techniques and intraoperative ultrasound, LRFA had been a new approach to local ablation. It had other advantages such as real-time security monitoring of the ablation process and accurate detection of tiny lesions, compared with percutaneous RFA. Some studies had confirmed that LRFA had fewer complications and lower hospitalization mortality compared with percutaneous RFA.26,27 But little study has been reported on its long-term efficacy. Meanwhile, as a new therapeutic method, long-term effect of LRFA was not yet certain. Therefore, this study intends to use meta-analysis to evaluate the long-term efficacy of LRFA in early HCC.
The meta-analysis results showed that the local recurrence rate of LRFA was 32% higher than that of other surgical procedures (RR = 1.32, 95% CI [1.01–1.73], P = .04). At the same time, there was no statistical difference between LRFA and other surgical procedures of whether 1-year (hazard ratio = 0.99, 95% CI [0.93–1.07], P = .88), 3-year (hazard ratio = 0.90, 95% CI [0.77–1.06], P = .21), or 5-year disease-free survival rate (hazard ratio = 0.86, 95% CI [0.69–1.08], P = .17). Moreover, as for overall survival rate of whether 1-year (hazard ratio = 0.97, 95% CI [0.94–1.00], P = .07), 3-year (hazard ratio = 1.00, 95% CI [0.93–1.06], P = .89), or 5-year (hazard ratio = 1.03, 95% CI [0.94–1.13], P = .55), there was no statistical difference between LRFA and other surgical procedures. It was guessed that different surgical procedures may be the cause of heterogeneity. Therefore, subgroup analyses according to different surgical procedures were performed to accurately investigate the long-term efficacy of LRFA and other surgical procedures.
Subgroup analysis results showed that there was no statistical difference in the local recurrence rate between LRFA and other minimally invasive ablation, but the local recurrence rate of LRFA was 48% higher than that of HR. It indicated that HR was better than LRFA in prevention of local recurrence. As for disease-free survival rate of whether 1 year, 3 years, or 5 years, there was no statistical difference between LRFA and other minimally invasive ablation. However, 3-year disease-free survival rate of LRFA was 29% lower than that of HR, although there was no statistical difference in 1-year or 5-year disease-free survival rate. It indicated that there were more local recurrences after LRFA than HR during the period from 1 to 3 years. As for overall survival rate, there was no statistical difference between LRFA and other surgical procedures in 1-year overall survival rate. Compared with other minimally invasive ablation, 3-year overall survival rate of LRFA increased by 26% and 5-year overall survival rate of LRFA increased by 28%. It indicated that laparoscopy was better than other ablation approaches in improving overall survival rate. Compared with HR, 3-year overall survival rate of LRFA decreased by 19% and 5-year overall survival rate of LRFA decreased by 20%. It indicated that HR was better than LRFA in improving overall survival rate.
Some limitations of this meta-analysis should also be taken into account. Because all included studies were nonrandom control trials, there may be a negative impact on the quality of studies and evidence intensity of our results. We expect reliable evidence from high-quality, double-blind, randomized control trials. Few included studies had reported intraoperative and postoperative outcomes; it may be a problem worth of attention. Another limitation is the relatively small number of studies and patients. As a result, some of the hazard ratios had an upper range of 1.00 or 1.01 with P values of .06 or .07. With more data these borderline observations might become statistically significant.
Conclusion
In conclusion, our findings demonstrated that patients who underwent HR had higher 3-, 5-year overall survival rate, 3-year disease-free survival rate, and lower local recurrence rate than those who underwent LRFA. However, patients who underwent LRFA had higher 3-, 5-year overall survival rate than those who underwent other minimally invasive ablation, although there was no statistical difference in local recurrence rate or disease-free survival rate. It indicates that HR is still the first choice for the treatment of early HCC, and LRFA is better than other minimally invasive options.
Footnotes
Acknowledgment
The authors thank Mr. Zhong Guo-Chao for reviewing an early draft of this article and giving valuable comments.
Authors' Contributions
H.-Y.T. processed data, analyzed results, and wrote this article. J.-F.G. and F.Y. screened studies, extracted data, and evaluated quality. W.-H.T. analyzed results and polished the language. K.Y. designed this research and evaluated practicality.
Disclosure Statement
This study was not funded, and none of the authors have any conflicts of interests to disclose.