
Abstract
Abstract
Purpose:
There is a lack of experience with stenting for benign pancreaticobiliary disorders in children.
Materials and Methods:
Fifteen children (9 male and 6 female) with a median age of 7.1 years (range 0.7–14.2 years) who underwent treatment with a plastic stent for a benign disorder of the pancreaticobiliary system between May 2003 and September 2017 were recruited to this retrospective study.
Results:
Biliary and/or pancreatic plastic stents were inserted into 5 patients with congenital, 4 with post-traumatic, and 6 with idiopathic pathologies. Median duration of individual stent placement was 111 days (range 14–1569 days). Eleven children (73%) were treated with one stent only. In 4 cases, up to 22 stents were successively placed over time. There were no complications during stent insertion or stent removal. Seven patients (47%) experienced adverse effects during stenting, including choledocholithiasis, pancreaticolithiasis, cholangitis, acute pancreatitis, stent obstruction, and stent fracture. At follow-up, in 11 cases (73%), the underlying condition was resolved. In 4 children, all of whom suffered from congenital pancreaticobiliary disorders, stent therapy was considered as a temporary treatment before definite surgery.
Conclusions:
Patients with congenital anomalies of the pancreaticobiliary tree often require surgery for definitive management. However, temporary stent placement can be accomplished safely and successfully and this serves as a bridge to temporize their obstructive process while awaiting surgical intervention. Children with post-traumatic or idiopathic disorders can frequently be managed definitively by stenting alone and many of these require only one single stent insertion.
Introduction
Over the past years, endoscopic retrograde cholangiopancreaticography (ERCP) has played increasing part in the management of benign pancreaticobiliary disorders in children.1–4 In contrast to adults, it is still considered both, a diagnostic and therapeutic tool in the pediatric population.4–6
The spectrum of ERCP in children is broad and includes a variety of congenital, post-traumatic, and idiopathic conditions. Therapeutic procedures consist of endoscopic sphincterotomy (EST), common bile duct (CBD) or pancreatic duct stone removal, transmural drainage of pancreatic fluid collections, as well as biliary and pancreatic stent insertion.1,5 However, there is still a lack of awareness regarding specific indications and limited local availability, including the expertise of experienced endoscopists to perform ERCP in this group of patients. 5
In 1989, Guelrud et al. were the first to report on endoscopic insertion of a biliary stent in a male infant for malignant obstructive jaundice before chemotherapy. 7 Subsequently, Brown and Goldschmiedt described their experience with therapeutic ERCP, including stent placement for benign biliary and pancreatic disorders in 9 patients under the age of 20 years. 8 In 1997, Tagge et al. 9 demonstrated the use of biliary stents in 3 children with complicated choledochal cysts. Since then, endoscopic stenting has been used as a minimally invasive technique and additional instrument in the management of various conditions within the alimentary tract in this group of patients.5,10–14
We report our interdisciplinary experience with plastic stents for the treatment of benign pancreaticobiliary disorders in children.
Materials and Methods
Fifteen children (9 male and 6 female) who underwent plastic stent placement for benign disorders of the pancreaticobiliary system between May 2003 and September 2017 were recruited to this retrospective study (Table 1). The primary outcome measure of success after ERCP and stent placement was correct diagnosis and/or adequate therapy with resolution of the pancreaticobiliary disease. The study was approved by the Research Ethics Committee of the Medical Faculty Mannheim, Heidelberg University, Germany (No. 2018-813R-MA).
Patients' Characteristics and Outcome
Two stents were applied simultaneously to the CBD and pancreatic duct.
First stent applied elsewhere and remained in situ for 88 days.
Patient developed pancreatic exocrine insufficiency not related to stent treatment.
Stent lost spontaneously.
During ERCP and stent placement, a simultaneous intrahepatic biliary stricture was detected, which was not resolved (see text).
Patient underwent subsequent LC after stent removal.
AP, acute pancreatitis; CBD, common bile duct; CCL, cholecystolithiasis; CDL, choledocholithiasis; CP, chronic pancreatitis; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreaticography; EST, endoscopic sphincterotomy; f, female; HS, hereditary spherocytosis; LC, laparoscopic cholecystectomy; m, male; MRCP, magnetic resonance cholangiopancreaticography; NA, not available; OC, open cholecystectomy; PBM, pancreaticobiliary maljunction; PL, pancreaticolithiasis; RHH, right hemihepatectomy; TS, transgastric stent; US, ultrasound.
The overall median age at stent placement was 7.1 years (range 0.7–14.2 years). Approximately half of the cohort (47%) had a variety of previous therapies before stenting, including percutaneous drainage of a dilated common hepatic duct or biloma, as well as ERCP with EST or dilatation, and stone extraction (Table 1).
Stent placement for congenital disorders
In 5 children (2 male and 3 female) with a median age of 5.5 years (range 0.7–14.2 years), a congenital abnormality of the pancreaticobiliary system was noted (Table 1). Of these, 2 patients suffered from a choledochal cyst associated with a biliary stricture (patients 2 and 15). One 8-year-old girl developed choledocholithiasis (CDL) caused by pancreaticobiliary maljunction (PBM) (patient 3). Another 14-year-old boy (patient 6) underwent stenting for chronic pancreatitis (CP). During ERCP, a pancreas divisum with a pancreatic stricture was detected. Finally, an 8-month-old male infant (patient 9) suffered from CDL with acute pancreatitis (AP) associated with a stricture of the papilla of Vater.
Stent placement for post-traumatic disorders
In 4 cases (2 male and 2 female), stent placement was performed after an injury to the biliary system that was caused either by a surgical complication (i.e. iatrogenic) or after trauma (Table 1). The median age in this subgroup was 5.8 years (range 2.3–7.1 years). On analysis, 1 boy (patient 1) suffered from a postoperative stricture after laparoscopic cholecystectomy (LC). Two children (patients 8 and 13) developed a biliary leakage after open cholecystectomy and right hemihepatectomy (RHH), respectively. Another 5-year-old boy (patient 11) who sustained a pedestrian versus car accident suffered from a blunt abdominal injury with an intrahepatic lesion to the bile duct within liver segment 4.
Stent placement for idiopathic disorders
Six patients (5 male and 1 female) with a median age of 10.7 years (range 3.4–12.7 years) were diagnosed with AP or CP and sequelae to the pancreaticobiliary system requiring stenting. In all cases the underlying condition was unknown (i.e. idiopathic). Of these, 4 children with biliary or pancreatic duct stones developed a stricture and/or obstruction either to the pancreatic (patients 4, 5, and 12) or to the common bile duct (patient 14). In 2 other patients (patients 7 and 10), a transgastric stent was inserted for drainage of a pancreatic pseudocyst.
In all cases but 1, straight biliary (Percuflex™ Duodenal Bend Biliary Stent) or pancreatic (Advanix™ Pancreatic Stent) plastic stents were used (Boston Scientific Corporation, Natick, MA). In 1 child (patient 11), a double pigtail stent (Double Pigtail Stent; ©Wieser GmbH Medizintechnik and Geräte, Egenhofen, Germany) was inserted. Depending on patient's disorder the stent diameter varied from 5F to 10F with a length between 5 and 16 cm (Table 1).
ERCP was carried out in all instances as an inpatient procedure with a postinterventional observation of at least 2 days. Depending on patient's age and the underlying condition, stents were inserted under general anesthesia or conscious sedation. Simultaneous fluoroscopy was performed in each case to confirm stent position. Perioperative complications were documented including post-ERCP pancreatitis that was graded according to the revised Atlanta classification. 15
Patients were discharged from hospital once they had recovered with the stent being in situ and were regularly followed up as outpatients. Finally, in April/May 2018 in 12 out of 15 cases (80%), a telephone interview regarding the actual medical condition was conducted. The median follow-up poststent removal was 22.3 months (range 2.8–154.4 months).
Results
The median duration of individual stent placement in 14 out 15 children was 111 days (range 14–1569 days). In 1 child (patient 10), the device was discharged spontaneously and, therefore, the exact time of stenting is unknown in this case. Eleven patients (73%) were treated with one stent only. In 4 children, up to 22 different plastic stents were successively placed. Therefore, the absolute stenting time increased up to a maximum of 3406 days in 1 case (patient 3). Of note, simultaneous EST was performed in 10 out of 15 cases (67%).
Stent placement for congenital disorders
Median stenting time within this subgroup was 124 days (range 40–274 days).
Three out of 5 children with congenital disorders experienced different problems such as CDL with cholangitis (patient 3), pancreaticolithiasis (PL) (patient 6), and AP (patient 15) after stenting.
In 3 cases (patients 2, 6, and 15), only one single plastic stent was inserted over time (Fig. 1). All of these patients required definite surgery in the course of treatment. Both children with choledochal cyst (patients 2 and 15) underwent resection and hepaticojejunostomy. In the boy with pancreas divisum (patient 6), the pancreatic duct was permanently drained by longitudinal pancreaticojejunostomy (Partington–Rochelle). The 8-year-old girl (patient 3) with PBM had numerous stents inserted over a period of >10 years. Of note, due to the underlying condition, stents were inserted simultaneously to the CBD and pancreatic duct. Despite strong recommendations for her to undergo surgery, the parents rejected this approach until she became of legal age. Finally, definite resection with hepaticojejunostomy was performed. All children who ultimately had undergone surgery remained well at last follow-up.
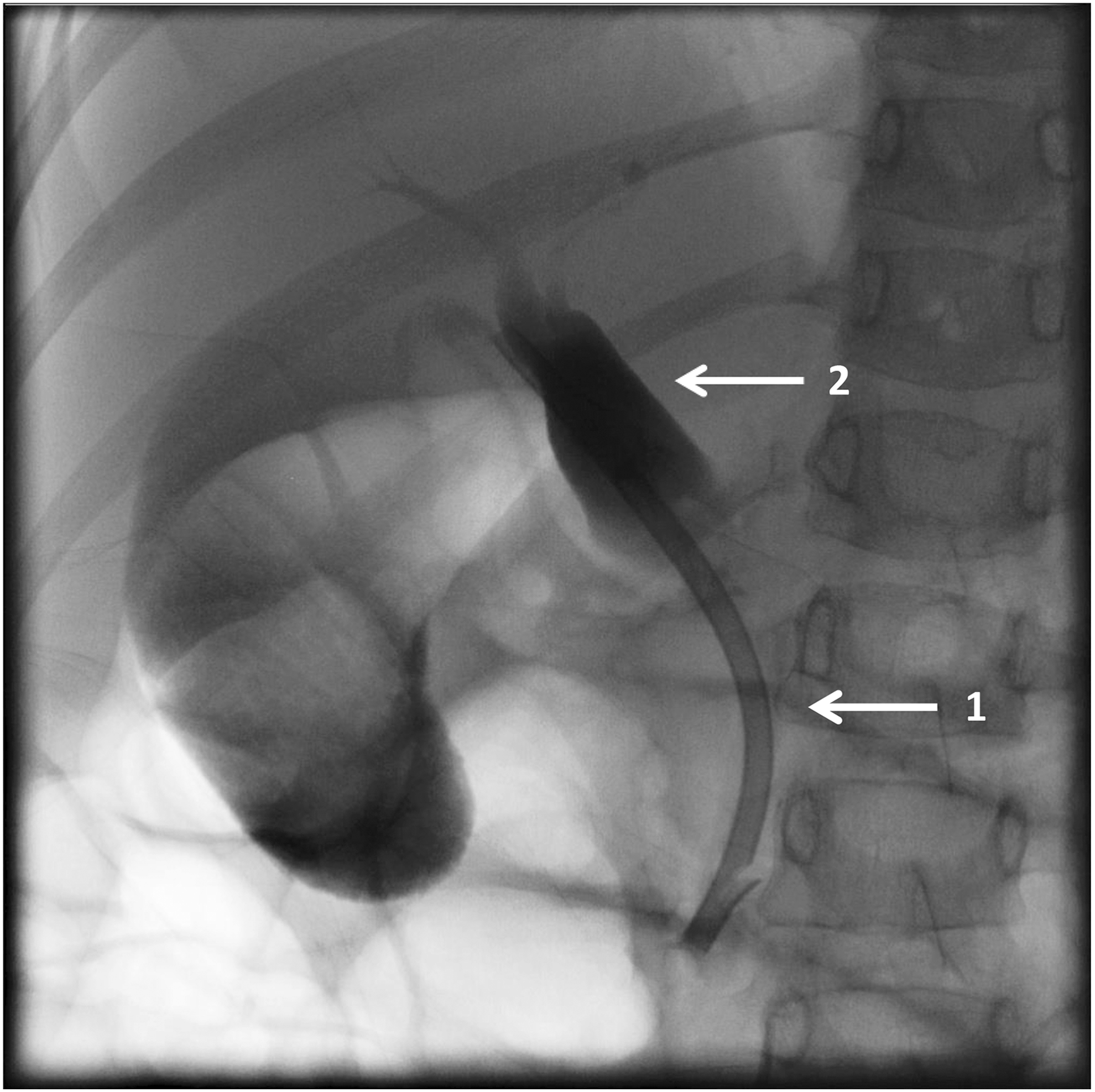
Stent placement (1) in a 5-year-old girl (patient 15) with choledochal cyst (2).
Lastly, the boy with a congenital problem to the papilla of Vater (patient 9) was treated with two stents that were placed successively due to a persistent stricture. At follow-up, he remained asymptomatic without the need for further intervention.
Stent placement for post-traumatic disorders
Median stenting time in patients with post-traumatic disorders was 69 days (range 14–91 days).
In 3 out of 4 cases (patients 1, 8, and 13), no complications were noted while the stents were in situ. However, in 1 girl (patient 13), a stent fracture occurred during stent removal. Another boy (patient 11) developed one episode of cholangitis after ERCP with EST and stent placement, which resolved after a course of antibiotics. Three children within this subgroup required only one single plastic stent. Of these, 2 girls (patients 8 and 13) had their biliary leakage successfully treated without further intervention. In another boy (patient 11), who sustained an abdominal trauma, an attempt to drain a biloma with an external drain for 24 days failed. Subsequently, ERCP with EST and stent insertion for 14 days resolved the problem (Fig. 2). However, during stent removal, a persistent intrahepatic stricture was detected and dilated once. This patient is currently under observation because of intermittent abdominal pain and diminished liver function on elastography.
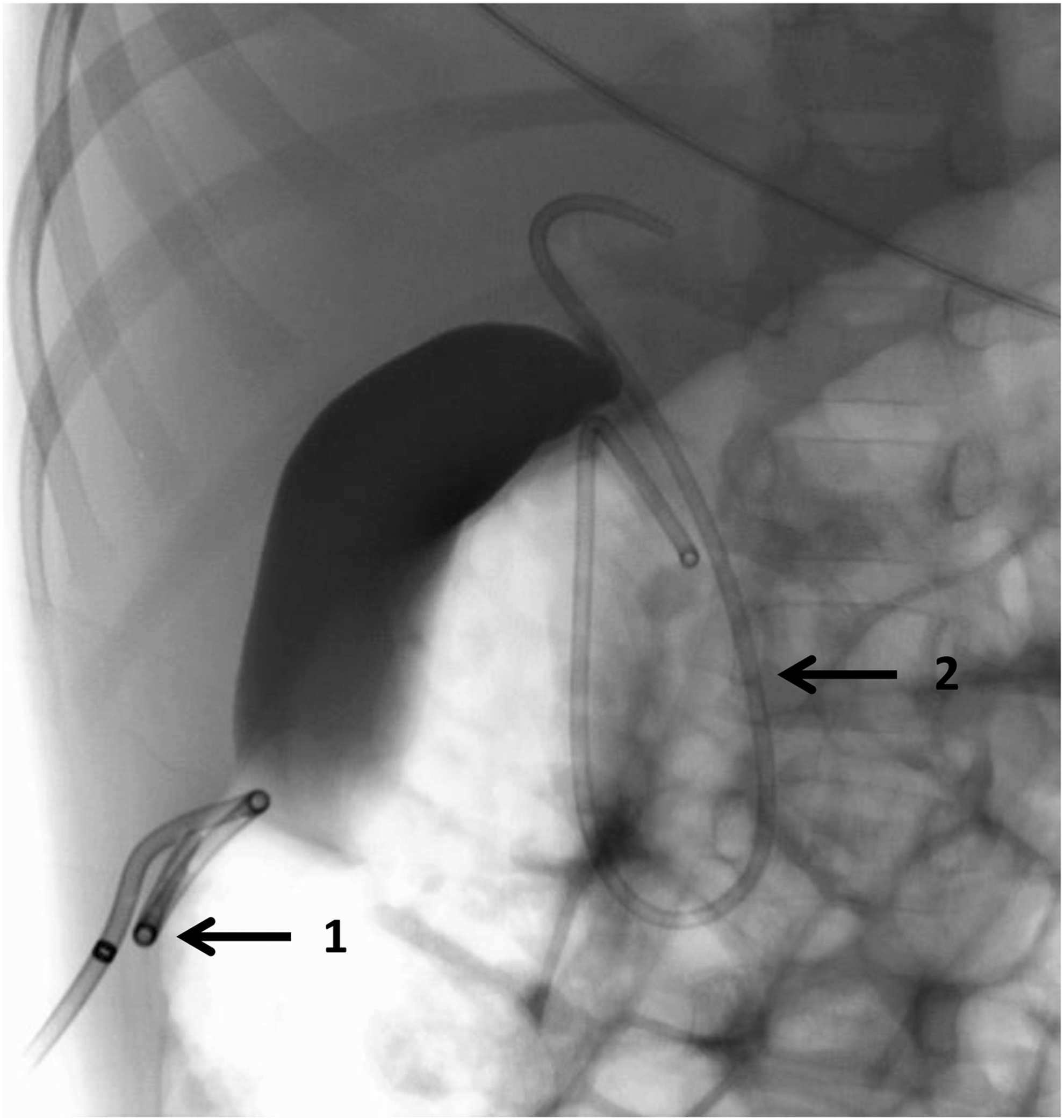
External percutaneous drainage of a biloma (1) and placement of a double pigtail stent (2) in a 5-year-old boy (patient 11) after blunt abdominal trauma.
The boy with a biliary stricture after LC (patient 1) had a total of four stents inserted before the problem resolved.
Stent placement for idiopathic disorders
Median stenting time within this cohort was 98 days (range 50–1569 days).
Two out of 6 cases with idiopathic disorders developed complications during stent therapy, including recurrent stent obstruction (patient 5) and mild AP (patient 14).
Five children (patients 4, 7, 10, 12, and 14) in this subgroup had only one stent inserted. All remained well at last follow-up. Of note, patient 14 underwent elective LC after stent removal. In addition, the boy with a pancreatic stricture (patient 5) had his first stent inserted elsewhere. As already mentioned, stent obstruction combined with persistent stricture resulted in a total of four stents before he improved. At follow-up, clinical signs of pancreatic exocrine insufficiency not related to stent therapy were observed.
Overall, 11 out of 15 children (73%) had their pancreaticobiliary disorder resolved after ERCP and stent placement.
Discussion
In this cohort, stent placement for congenital pancreaticobiliary disorders was mainly used as a temporary instrument in the course of treatment. In 80% of these patients, definite surgery was finally required to solve the problem. This is in accordance with other authors: Tagge et al. 9 reported on successful endoscopic decompression of complicated choledochal cysts in 3 children as an alternative to urgent surgery. Another group demonstrated stenting in 11 children with choledochal cysts as part of an effective preoperative management with pain relief soon after the procedure. 14 The rationale of this approach is to reduce the intraductal pressure within the pancreaticobiliary tract caused by protein plugs (protein plug theory). 16
In cases of pancreas divisum or PBM, the role of endoscopic therapy remains controversial and unproven.2,17 In this study, we applied stents as a preoperative instrument in 2 children with pancreas divisum and PBM, respectively. Both required definite surgery due to persistent strictures after stenting and remained well at follow-up after 6 and 36 months. In contrast, Agarwal et al. 17 were able to resolve symptoms in 7 children with pancreas divisum by stent placement only. However, in their study the exact follow-up time was not stated. 17
Part of the management for an abnormal papilla of Vater ERCP, EST, and subsequent stent placement have been described previously.4,18,19 In Paris et al.'s review, 19 6 out of 29 children suffered from papillary stenosis. Of these, 1 had a total of eight stents inserted in the course of treatment. Subsequently, 3 patients underwent definite surgery after ERCP. However, the rational decision-making regarding their endoscopic management remains unclear. 19 Another large retrospective series in 167 patients observed 11 cases with CP caused by sphincter of Oddi dysfunction. Although a total of 52 stents were inserted over time, precise assignment of the interventions and outcome is vague. 4 In cases of a papillary stenosis, it is often difficult to assess whether the disorder is the cause or rather the consequence of AP/CP. In our case, we assumed a true congenital stricture of the papilla of Vater because of the patients' young age, absence of inflammatory signs, and the fact that no other cause for CDL could be detected. Nevertheless, the child improved after EST and insertion of two successively placed stents.
Duration of stent placement in children is still being debated in the literature. In our series, the median stenting time in the subgroup with congenital disorders was 124 days. In accordance with other authors,14,17 most of our patients experienced an immediate improvement of symptoms, including pain relief after stent insertion. In the meantime, with the stent being in situ, preoperative diagnostics were completed and the nutritional status of the patients was optimized. These benefits after stent therapy were acknowledged by others.2,3 Tsuchiya et al. reported on a median period of only 12 days (range 5–47 days) in children with choledochal cysts until stent removal and excision of the extrahepatic bile duct. 14
The management of post-traumatic leakages and strictures of the pancreaticobiliary system consists of ERCP and temporary stent placement in children as well as in adults.10,11,20–22 This series included 3 cases of leakages to the biliary system, of which 2 occurred after surgery and 1 after blunt abdominal trauma. Another patient developed a postoperative biliary stricture. All cases were successfully treated with ERCP and stenting only.
In 2017, van As and Millar 22 reported on a well-established nonoperative management of pediatric liver trauma in >90% of their patients, including sphincterotomy and internal drainage in patients who developed persistent biliary leakage. 22 Similarly, in 1 of our cases, in which external drainage of a biloma had been unsuccessful, ERCP and stent placement were performed resulting in subsequent improvement within 14 days. Kulaylat et al. 10 reported on 11 children, who suffered from bile leaks after blunt abdominal trauma. Of note, none of their patients developed a stricture after stenting for a median of 60 days (range 12–438 days). 10 In our patient, a post-traumatic intrahepatic stricture is currently under regular observation and considered to undergo surgery to prevent cirrhosis and/or malignancy.11,22
Steen et al. 12 reported on the management of persistent bile leaks after partial liver resection in children. From their experience, they recommend a stenting time for the healing of a small leak of 6 weeks. If the leak is still present, the stent should be changed and left for another 6 weeks. 12 In our patient, a stenting time of 69 days with one stent only resolved the problem of a postoperative leakage after RHH.
In one case with a biliary stricture formation following LC, four different stents were inserted successively over a cumulative stenting time of 266 days before the problem was resolved. With regard to literature, Steen et al. 12 evaluated the value of ERCP and stenting in the management of postoperative biliary strictures in children equivocally. In their series, only 1 out of 3 children with an isolated bile duct stricture was treated with ERCP and stent placement, whereas the other 2 received hepaticojejunostomy or liver transplantation, which makes it hard to draw any conclusion. 12
In this study, all but one idiopathic disorders were successfully managed with one single plastic stent only. In the boy with a pancreatic stricture and CP, four different stents were required. Of note, the median age in this subgroup was 10.7 years, and the patients were generally older than those with congenital or post-traumatic pancreaticobiliary disorders.
Keane et al. 5 demonstrated successful endoscopic transmural drainage of pancreatic pseudocysts through stent placement. Similarly, Jazrawi et al. 23 found that transmural stent placement was effective and safe in 8 out of 10 children with symptomatic pseudocysts. 23 Likewise, most recently another group stated a high clinical success in endoscopic drainage of pancreatic fluid collections with plastic stents in 28 out of 30 children (93.3%), in whom the stents were removed after 3 months. 24 Two patients with pancreatic pseudocysts had their plastic stents lost spontaneously or removed after 1569 days, respectively.
In cases of pancreatic strictures, Krishnamoorthi et al. 25 postulated plastic stents as the stent of choice for endoscopic treatment. In this cohort, 3 children were successfully managed for a pancreatic stricture associated with AP/CP with pancreatic plastic stents. Most recently, Jeong et al. 26 reported on their experience with fully covered self-expandable metal stents for the management of refractory benign strictures of the main pancreatic duct in 8 children. Similarly to our patients, the median age in their cohort was 12 years. They observed a significant improvement of the mean diameter of the stricture from 1.1 to 2.8 mm after a median indwelling time of 6 months. 26
Lately, the use of metal stents has been demonstrated to be more cost-intensive without offering advantages to plastic stents.13,27
This study is limited by its retrospective approach and the small number of patients. Moreover, the variety of different pancreaticobiliary disorders makes this cohort inhomogeneous. Finally, we did not formally compare our results with a control group that was treated differently. Nevertheless, because prospective studies about these rare conditions cannot be expected, retrospective analyses are helpful to scrutinize the existing experience.
Conclusion
In conclusion, patients with congenital anomalies of the pancreaticobiliary tree often require surgery for definitive management. However, temporary stents placement can be accomplished safely and successfully and this serves as a bridge to temporize their obstructive process while awaiting surgical intervention. Children with post-traumatic or idiopathic disorders can frequently be managed definitively by stenting alone and many of these patients require only one single stent insertion. Physicians dealing with this group of patients should be aware of the inhomogeneous pathologies and consider stent placement as an enrichment of the armamentarium for these disorders.
Footnotes
Disclosure Statement
No competing financial interests exist.