
Abstract
Background/Purpose:
Many techniques have been described for the treatment of pediatric inguinal hernia (PIH). Some authors emphasized the importance of disconnecting the sac, to create a scar, and to close the peritoneum mimicking the open approach. Others stated that peritoneal disconnection alone is enough for treatment of PIH regardless of the size of the internal ring. In this study, we compare the short-term results of laparoscopic disconnection of PIH sac versus disconnection and peritoneal closure.
Patients and Methods:
The study was carried from March 2016 to March 2017, on 34 patients with 40 PIH. Patients were randomly divided into two groups: group A, subjected to laparoscopic hernia sac disconnection and group B, subjected to laparoscopic hernia sac disconnection with peritoneal closure. Both groups were compared regarding the operative details, including complications and conversion, postoperative complications and recurrence.
Results:
Group A included 20 hernias in 15 patients, whereas group B included 20 hernias in 19 patients. The age ranged from 1 to 23 months. In group A, the mean operative time (OT) was 34.6 and 39.4 minutes, for unilateral and bilateral cases, respectively, whereas in group B, it was 45.1 minutes for unilateral cases and 65 minutes for 1 bilateral case. The OT was significantly shorter in group A for unilateral cases. There was no conversion and no intraoperative complications. Three recurrences occurred in group A (15% of hernias/20% of cases) with no recurrences in group B; difference was statistically insignificant. All 3 recurrences occurred in hernias with an internal ring diameter (IRD) >10 mm. Hospital stay was statistically shorter in group B.
Conclusion:
Both laparoscopic sac disconnection with internal ring closure and sac disconnection only are safe and effective treatments of PIH. However, the latter technique is not recommended for cases with IRD >10 mm because of the unacceptable high recurrence with rings >10 mm.
Introduction
Pediatric inguinal hernia (PIH) is a common surgical problem; it represents ∼15% of pediatric surgical practice. 1 Conventional open repair of inguinal hernia has been accepted as the gold standard treatment of PIH because of its lower morbidity, good cosmesis, and lower rates of recurrence. 2 However over the last two decades with advances in pediatric minimal invasive surgery (MIS), laparoscopy has become more popular for the management of PIH.3,4 Laparoscopy offers many advantages over the open technique including magnification, detection of contralateral patent processus vaginalis (CPPV) and other various forms of hernia, best option for recurrent hernia, and minimal manipulation of vas deferens and testicular vessels. 5 Several techniques have been described including the use of extra or intracorporeal knotting and high ligation with or without disconnection of peritoneum at the internal ring. 6 Laparoscopic disconnection of the hernial sac with closure of the peritoneum over the internal ring was described to mimic the open technique and decrease the incidence of recurrence. 7 Some authors reported that disconnection of the hernial sac without peritoneal closure is an effective treatment, especially in hernias with small internal ring diameter (IRD) <10 mm.8–10 Others concluded that disconnection without closure is effective in larger rings up to 20 mm, 11 and even regardless of the size of the internal ring. 12 This study was designed to compare the short-term results of laparoscopic disconnection of the hernia sac versus disconnection and closure of peritoneum in children, as regards feasibility, operative details, recurrence rate, and postoperative complications.
Patients and Methods
This prospective randomized clinical study was carried out in the Pediatric Surgical Unit, Tanta University Hospitals, during the period from March 2016 to March 2017, on 34 patients with 40 PIHs. The study was approved by ethical committee of the Faculty of Medicine, Tanta University (Approval Code 30836/03/16). The study included infants and children with PIH with an age range from 1 month to 2 years. The intended primary outcome was recurrence within 6 months. We excluded incarcerated PIH, recurrent PIH, patients with undescended testis, patients with hydrocele, patients with chronic comorbidity—such as congenital heart disease and severe chest troubles—and patients with chronic cough or chronic constipation. Patients were randomly categorized into two groups. The randomization was carried out by the closed sealed envelope method. Group A included 15 infants and children with 20 hernias who were subjected to laparoscopic disconnection of the hernia sac without closure of peritoneum over internal ring. Group B included 19 infants and children with 20 hernias who were subjected to laparoscopic disconnection of the hernia sac with closure of peritoneum over internal ring. All patients were subjected to full clinical evaluation. Scrotal ultrasound (U/S) was carried out for all patients to evaluate the IRD and to examine the contralateral side. The initial intent was to include 80 hernias, 40 in each group. The study was designed to be carried out in 2 phases, with 40 hernias in each phase, with an interim analysis after phase 1. However, the authors decided to stop the study after phase 1 because of the unacceptable recurrence rate in group A.
Operative Techniques
Common steps for both groups
All patients received general anesthesia with endotracheal intubation. Children were placed in a supine position; the surgeon stood at the head of the table and the patient, with the anesthesia machine moved to the right side of the operating table, the cameraman to the left side of the surgeon, the scrub nurse to the left of the table, and the monitor at the feet of the patient (Fig. 1). This arrangement is very convenient especially if a contralateral hernia is present or found at exploration. In very small infants the cross-table position can be used with the surgeon at the head of the baby, the cameraman to the left, scrub nurse to the right of the surgeon, and the monitor at the feet of the baby across the table (Fig. 2). A mixture of lignocaine 2% (3 mg/kg) plus bupivacaine 0.25% (2 mg/kg) was injected at port sites.

Position of the surgeon and assistants in children.

The cross-table position in small infants.
In all patients, an open technique was used to establish pneumoperitoneum at the site of an umbilical port. The abdomen was insufflated with CO2, initially at a pressure of 6–8 mmHg, with a flow of 1.5 L/min. Pressure can be then raised to 8–10 mmHg, and flow to 2–3 L/min depending on the age. A 5 mm, 30° telescope was used. Two 3 or 5 mm trocars—or 3 mm portless instruments—were inserted at the lateral margin of the right and left rectus muscles, about the level of the umbilicus under vision. The head of the table was lowered in Trendlenburg's position and the table was turned to the contralateral side of the hernia to withdraw viscera away from hernial openings. Laparoscopic exploration was used to inspect peritoneal cavity and examine the hernial side and contralateral side as well. Size of the internal ring was measured with a thread stretched in a transverse manner between two laparoscopic graspers (Fig. 3).

Measuring the size of the internal ring.
The dissection was then started using a Maryland and fine scissors. A small rent is made just medial or lateral to the vas and vessels depending on the side of the hernia. The rent was then made wider by spreading the scissors inside it. The edge of the rent was then held up and using the closed scissors, any important structures (vas deferens, vessels, or lymphatics) were swept away leaving transparent peritoneum (Fig. 4). After assuring a safe denuded peritoneum, a cut was made. This was repeated in a circumferential 360° manner until the peritoneum at the internal ring was completely disconnected (Fig. 5).
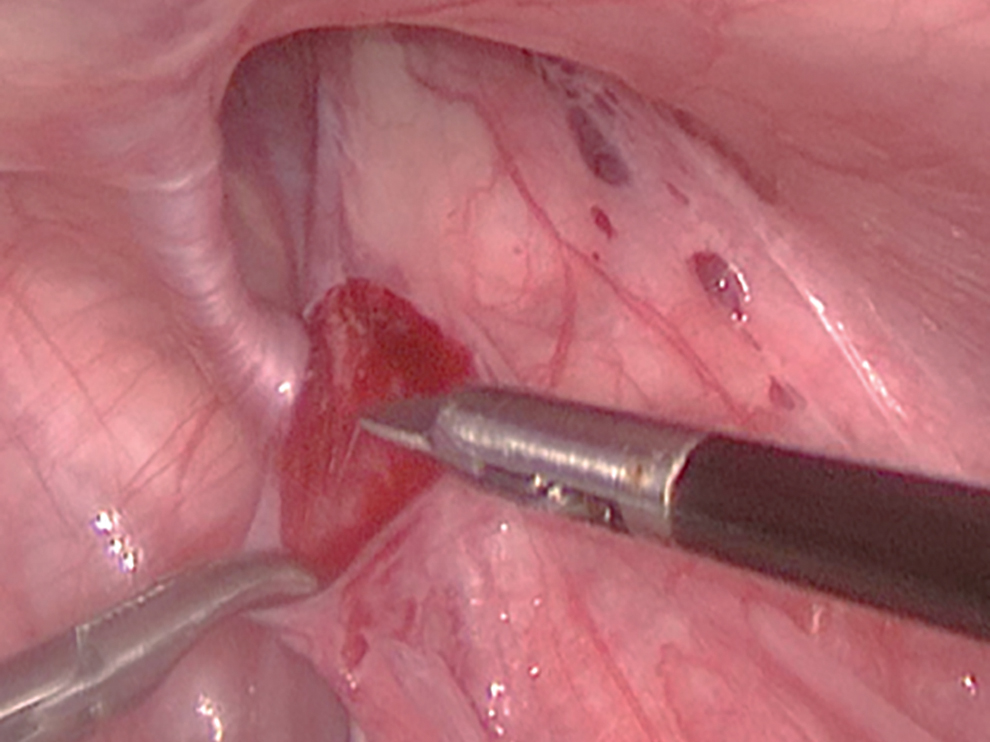
Hernia sac is held by a grasper and an incision is made in the peritoneum.

Complete disconnection of the hernia sac, left side. DSE, disconnected sac edge; IEV, inferior epigastric vessels; MUL, medial umbilical ligament; TV, testicular vessels; VD, vas deferens.
At this point management differs in each group. In group A the procedure was concluded. In group B a 3/0–4/0 suture (Vicryl) on a 20–22 mm round needle was used. The needle was passed percutaneously through the abdominal wall lateral to the inguinal canal and running simple sutures were used to close the peritoneal rent and ligated intracorporeally (Fig. 6). Great care was taken not to injure or strangulate the vas or vessels. The needle was retrieved under vision either through the abdominal wall, a 3 mm stab incision, or a 5 mm trocar. Fascia was closed with Vicryl sutures and skin was closed with steristrips.

Complete closure of peritoneum over the internal ring.
Postoperatively (PO), analgesics were given in the form of paracetamol and/or diclofenac suppositories depending on age. Oral feeding was started 6 hours after surgery. Patients were discharged the next morning.
Patients were followed-up in the outpatient clinic at 1 week, 1 month, 3 months, and 6 months PO (or contacted by phone for the late 3 or 6 months follow-ups). The follow-up was to look for recurrence and any other complications.
Statistical analysis
Qualitative data were described using number and percent. Quantitative data were described using range, mean, standard deviation, and median. Significance was judged at the 5% level. Chi-square (χ 2 ) and Fisher's exact test were used for comparing between the two groups, for example, demographic data, clinical data, recurrence, and postoperative complications. Mann–Whitney test was used to compare the two groups for operating time, hospital stay, and IRD.
Results
Preoperative data
This study included 34 patients who presented with clinical unilateral PIH. Their ages ranged from 1 month to 23 months (mean = 6.43 months). Our study included 30 male and 4 female children (male to female ratio was 7.5:1). Twenty-three cases (67.7%) were right-sided clinical hernias with 5 cases detected as having a latent left (subclinical) hernia by preoperative U/S examination, whereas 11 cases (32.4%) were left-sided clinical hernias with 1 case of U/S detected left latent (subclinical) hernia. The size of IRD, by preoperative U/S examination, ranged from 4.5 to 17 mm (mean = 7.68 mm ±3.11). There was no significant difference between both groups regarding all the preoperative parameters (Table 1).
Preoperative Data
Refers to (subclinical) CPPV detected by US.
CPPV, contralateral patent processus vaginalis; IRD, internal ring diameter; U/S, ultrasound scan.
Operative data
In this study, 40 hernias were repaired laparoscopically without conversion. Operative time (OT) was calculated from skin incision to skin closure including port insertion and port site closure. It ranged from 30 to 42 minutes (mean ± SD = 34.6 ± 3.71) for unilateral cases and from 35 to 50 minutes (mean ± SD = 39.4 ± 4.39) for bilateral cases in group A, whereas it ranged from 38 to 53 minutes (mean ± SD = 45.1 ± 4.87) for unilateral cases and 65 minutes for 1 bilateral case in group B. Regarding unilateral cases, the OT was shorter in group A than group B and the difference was statistically significant (P < .001). Although the OT for the bilateral case in group B was longer than the maximum OT for the bilateral cases in group A, statistical difference could not be calculated because it was only case. The mean IRD as measured by laparoscopy was 10.8 ± 3.26 mm (range = 6–23 mm), which is bigger than the U/S measurement (mean = 7.68 mm ±3.11). All cases diagnosed as latent contralateral hernia by U/S were found positive for PPV by laparoscopy and all cases that were diagnosed with no CPPV by US were found negative for PPV by laparoscopy. No intraoperative complications, bleeding, injury of the vas or vessels, or missed needles were encountered in both groups (Table 2).
Operative Data
IRD, internal ring diameter.
Postoperative data
Recurrence occurred in 3 of 20 (15%) hernias in 3 cases (that represents 3/15 cases; 20%) in group A, whereas no recurrences (0%) occurred in group B (P = .231); however, the difference was statistically insignificant. Although this difference is not statistically significant, this may be clinically significant and the small number of cases in this study weakens the statistical power. IRD of all these 3 recurrences measured >10 mm intraoperatively and all were on the right side. Recurrence rate for hernias that measured >10 mm intraoperatively was 3 of 11 (27%) for group A versus 0 of 9 (0%) for group B (P = .145), whereas recurrence rate for hernias ≤10 mm was 0 of 9 and 0 of 11 for group A versus B, respectively (P = 1.000). IRD in recurrent cases was 13, 15, and 19 mm. Recurrence occurred during the first 24 hours PO in 2 cases, whereas it appeared 1 week PO in 1 case. The 2 early recurrences were repaired laparoscopically the next day with peritoneal closure. The case presenting after 1 week was inspected laparoscopically then converted to open local tissue repair using conjoint tendon and inguinal ligament. The trial was stopped early because of this unacceptably high recurrence rate.
Transient scrotal edema developed in 3 cases (15%) in group A and in 2 cases (10%) in group B; all resolved by conservative treatment. The difference was statistically insignificant for these minor complications. No port site hernia or wound infection developed in any case.
All patients were discharged the morning of the next day of operation except in the 2 cases where recurrence occurred who were discharged on day 4 PO after repair of recurrence. The third recurrent case was readmitted on detection of recurrence at the first follow-up visit on day 7 PO. The mean hospital stay of all cases in group A, including the readmission hospital stay was 33.6 hours, whereas it was 24.7 hours in group B (P = .042) (Table 3). The mean follow-up of the cases in this study was 7.3 months (range = 6–11 months).
Postoperative Data
Discussion
Inguinal hernia repair remains the most common operation performed by pediatric surgeons. It occurs in 0.8%–4.4% of all children with higher incidence (up to 30%) in premature babies.13–15 Conventional herniotomy is considered the gold standard treatment method for PIH.16–19 With feasibility and safety of laparoscopy firmly established in pediatric surgical practice,20,21 there is a justified trend toward the use of MIS to manage PIH because of the advantages it offers over the conventional procedure.4,19,22 Many technical variations have been described for laparoscopic repair of PIH and can be categorized as either intracorporeal or extracorporeal/percutaneous approaches.6,22 Early reports of laparoscopic inguinal hernia repair described closure of an intact peritoneum at the internal ring, for example, purse-string suture, Z suture, or the flip-flap technique.16,23,24 However, they were associated with high recurrence rate especially when a skip area was left in males over the vas and vessels.18,23,25–30 For that reason, techniques that transect the peritoneum over the internal ring were introduced to make some trauma and scarring at the hernia orifice to help a more durable healing.7–12,31–34 The recurrence rate dropped from 3.7% in intact peritoneum closure to almost 0%–1% in series transecting the peritoneum.7,19,32,33
Involving some component of trauma to the peritoneum is essential for durability of inguinal hernia repair. This certainly occurs during the open repair, where the sac is transected after ligation. This was supported by an experimental study, in a rabbit model, which compared suture ligation alone with suture ligation plus peritoneal trauma in 28 rabbits. The repairs were tested using pneumoperitoneum at 35 mmHg after removal of the suture. The suture plus trauma group showed 12.5% and 0% failure rates at 2 and 4 weeks, respectively, even after removal of the suture, whereas all repairs with suture alone failed. 35
Ostlie and Ponsky cauterized the peritoneum from the 8-o'clock to the 5-o'clock position of the internal ring skipping the area over the vas and vessels before placing a double loop around the internal ring. This creates a scar, which leads to a better closure. 22 Esposito et al. modified their technique by sectioning three-fourth of the periorificial peritoneum around the internal ring using monpolar hook electrocautery before placing a nonresorbable purse string suture. With this modification they had a 0% recurrence in their last 950 cases. This modification was originally introduced to decrease tension on the suture but the authors stated that it also creates a scar that adds to the strength and durability of repair. 36 In fact, it has been reported that the actual sac ligation may not be needed during repair, rather, just the sac transection,8,37 even regardless of the IRD. 12 This opinion is also supported by the fact that despite a PPV is only disconnected and not closed, after laparoscopic orchidopexy, a hernia does not develop.38,39 Actually, laparoscopic PIH repair can be classified into repairs with an intact peritoneum and repairs with a disconnected sac.
A major criticism of the laparoscopic repair remains its relatively high recurrence rate.18,23,27,40,41 However, many studies reported that laparoscopic herniotomy or other techniques have no or minimal recurrences, ranging from 0% to 3%.7,8,19,31,34,42–45 In general, the recurrence rate in laparoscopic inguinal hernia repair could possibly be because of tension at the closure of the internal inguinal ring, broken purse string suture, large hernia, missed special types of hernia, and presence of a skip area of sac or suture especially over the vas and spermatic vessels. 29
In our study, recurrence occurred in 3 of 20 hernias (15%) representing 3 of 15 cases (20%) in group A, whereas no recurrences (0%) occurred in group B. All recurrences occurred with IRD >10 mm and on the right side. There was no statistically significant difference between both groups regarding recurrence rate. However, it should be noted that the numbers in the study were small as the study was stopped because of the unacceptable high recurrence and morbidity in group A. This fact weakens this statistical insignificance. Pant et al., in a similar study, reported that recurrence occurred in 3 of 72 hernias (4.2%); 2 of 38 hernias (5.3%) were in the disconnection group and 1 of 34 (2.9%) in the disconnection and closure group with no statistically significant difference. Like our study, they reported that all recurrences occurred with ring diameter >10 mm. 46 Van Batavia et al., using disconnection/closure technique, reported 1 of 39 (2.6%) recurrence. 15 Many authors reported a 0% recurrence rate using the sac disconnection and closure technique.7,9,10,34 Riquelme et al. had a 0% recurrence rate with sac disconnection technique over a period of 4 years of follow-up, however he closed internal rings >10 mm. 8 García-Hernández et al. also reported that recurrence occurred in 2 cases (0.53%), using the disconnection only technique regardless the IRD. They removed the whole sac and in cases of complete scrotal hernias removed the sac until the testis is seen. 12 Shehata et al. reported a 0% recurrence in 20.5 months follow-up using disconnection only; however, they closed/repaired rings >20 mm. 11
In this study, recurrence occurred during the first 24 hours after the operation in 2 cases, whereas it appeared 1 week after the operation in 1 case. The 2 early recurrences were repaired laparoscopically with peritoneal closure, whereas the 1-week recurrence case was repaired with local tissue repair using conjoint tendon and inguinal ligament after failure of a trial of laparoscopic repair. Pant et al. reported early recurrence in 2 of their cases (24–72 hours), and 1 recurrence after 5 months, all were repaired by the open technique. Similar to us they had 1 recurrence on the first PO day that was repaired the next day. 46 García-Hernández et al. had recurrences in the first week after surgery, which was repaired between 4 and 8 weeks after surgery. They thought that recurrence was because of incomplete sac resection, so repair was carried out using conventional approach. 12 Van Batavia et al. repaired their only recurrence by the open technique. 15 We opted for immediate repair of recurrent hernias, as possibility of incarceration might be increased by edema and fibrosis that might narrow the hernia course. We also started with laparoscopy, as herniotomy performed laparoscopically is assumed to make open herniotomy more difficult. In the 2 cases that were reoperated laparoscopically the next day, we found that the disconnection was complete and the peritoneal edges were identifiable and could be sutured to close the defect, although with difficulty. In the late recurrence, repair was not possible laparoscopically where we found peritonealization of the surfaces previously denuded by sac disconnection, with fibrosis and friability of tissues (Figure 7), also the vas and vessels were almost indistinguishable. So, dissection was judged as risky and conversion was safer. Review of the video of this case ensured complete sac resection in the first operation. These findings can be attributed to the theories of peritoneal healing that suggest peritoneal regeneration by metaplasia of subperitoneal connective tissue cells in the denuded areas rather than centripetal growth from the wound margins and that mesothelial healing is complete by 8 days.46–48
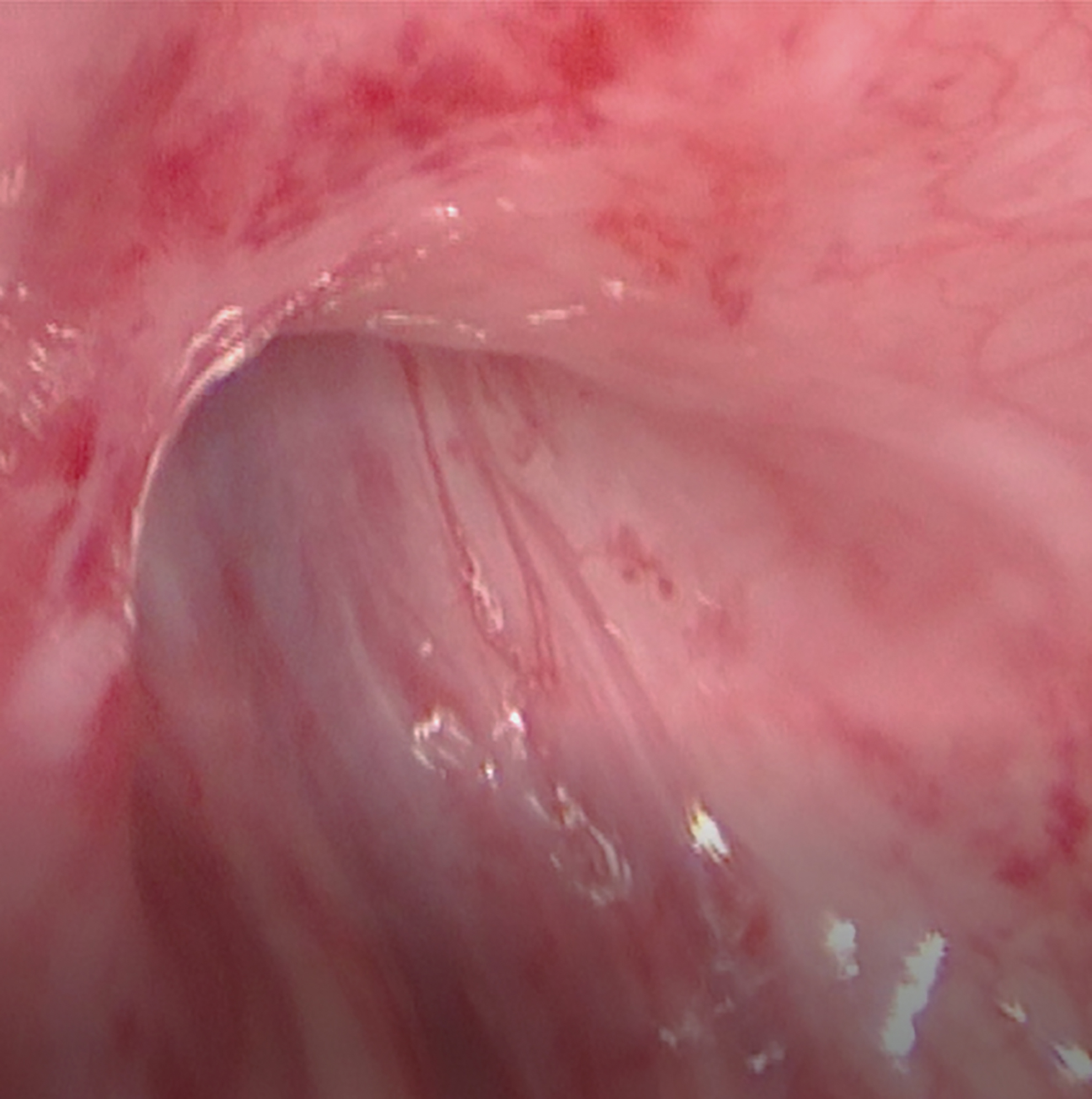
Appearance of recurrent inguinal hernia 1 week from operation.
In our study all recurrences occurred in defects >10 mm. This is supported by Riquelme et al. and Pant et al. who advocate closure of the peritoneum in defects larger than 10 mm.8,46 However, García-Hernández et al. performed resection of the hernia sac without sutures regardless of the sac's size during their study with only 0.53% recurrence, 12 and Shehata et al. closed only defects >20 mm and reported a 0% recurrence rate. 11 We also had 8 of 20 hernias (40%) in 7 of 15 cases (46.6%) with IRD >10 mm, which were repaired by sac disconnection only and yet no recurrence occurred. This suggests that IRD is not the only factor determining recurrence, and that other factors could be also involved; so further studies are required for this issue. However, referring to our results and others' we recommend using the sac resection only for hernias with IRD <10 mm.
In this study, the age ranged from 1 to 23 months. We excluded cases <1 month to avoid physiological insult of laparoscopic surgery in neonates. 49 We also excluded cases older than 24 months to avoid a wide variation in the IRD that may be bigger with older ages and that may affect the outcome. Many studies using similar techniques also excluded neonates8,9,12 and infants. 46
In this study, correlation between ultrasound (U/S) findings and laparoscopic view of inguinal hernia was performed. Despite confirmation of U/S results, regarding CPPV by laparoscopy, the number of cases in the study is small to draw a conclusion for U/S sensitivity and specificity for detection of CPPV. Ibrahim M also correlated between ultrasound findings and laparoscopic view of inguinal hernia; U/S failed to detect right CPPV in 5 cases (25%) that were diagnosed to have a contralateral hernia by laparoscopic exploration. 50 In our study, the IRD diameter measured by U/S was found to be significantly smaller than the IRD measured during laparoscopy, despite the fact that U/S was carried out by different operators. This difference can be explained by the fact that at laparoscopy, pressure of insufflation might increase the IRD. So operative plans should not be based on U/S measurements.
In this study, closure of the peritoneal defect was performed using Vicryl after disconnection of the sac in group B. Other studies also reported using Vicryl suture to close the peritoneum after disconnection of hernia sac.7,9,33,46 Others used nonabsorbable sutures including Polyester and V-Loc.8,15,51 Actually, as peritoneal trauma and subsequent scarring are supposed to be the main factors responsible for the durability of healing; use of absorbable sutures is justified.
The OT in this study was calculated from skin incision to skin closure. Comparing unilateral cases, it was shorter in group A than group B and the difference was statistically significant and the OT for the bilateral case in group B was longer than the maximum OT for the bilateral cases in group A. This can be considered an advantage of the disconnection only technique as it obviates the time taken to perform an intracorporeal suture. Pant et al. concluded that the difference in time taken between the two groups was significant for unilateral hernia repair, but was not found significant for bilateral hernia repair. 46
In this study, no intraoperative complications were recorded. Similar results were also reported in many other studies.8,9,11,12,15,19,33,34,50 By meticulous dissection using traction by a grasper to spread the peritoneum, which may be folded, and facilitate sweeping the vas and testicular vessels and lymphatics away by a closed scissors. This leaves a transparent peritoneum to be cut and thus, preventing injury of important structures. In addition, utmost care is taken to avoid including the vas or testicular vessels in the suture; the complete disconnection of the sac makes possible elevation of the peritoneum off the vas and vessels while suturing. We also make use of the excellent magnification and visualization of laparoscopy. In addition, at the level of the internal ring the vas and vessels are loosely attached to the peritoneum. which makes their dissection easier.9,10,52 Classic descriptions start the dissection in the lateral (safe) part of the internal ring.7,12 However, we start either just medial or lateral to the triangle of doom and free the vas and vessels first and then proceed to the lateral part of the internal ring. Shah et al. adopted the same principle. 34 Starting laterally will leave the area of the triangle of doom masked by hematoma, which makes visualization more difficult.
All cases were completed laparoscopically without conversion. Many reports also mentioned a 0% conversion.8,9,19,12,11,34,36,46,50 Becmeur et al. converted 4 patients (4.8%); 3 had direct and 1 had an incarcerated hernia. 7 Van Batavia et al., converted 1 patient (2%) owing to laxity of the inguinal canal floor and performed an open Bassini repair. 15 However, this reinforcement could also be carried out laparoscopically by the technique of muscular arch repair described by our group. 53
The overall mean hospital stay was significantly longer in group A. This difference is because of the days added for recurrent cases. The noncomplicated cases were discharged the next morning. Variable hospital stays were mentioned in different reports of laparoscopic hernia repair in children from 4 to 24 hours, depending on patient and local circumstances.7,9,10,11,34,46 In our study we had infants as young as 1 month and the maximum age was 23 months; also, some of the cases were from rural areas with difficult access to our hospital especially in late night hours, so we opted to keep them till the next morning. However, we shifted to same day discharge, for suitable cases, after we finished this study.
Limitations of the study
The small number of cases is the main limitation of this study. This study was an initial phase and the authors decided to stop at this phase because of the unacceptable morbidity and reoperations in group A. The results of this study need a larger number from multiple centers to assure the safety of only disconnecting (without closure) hernias with IRD of <10 mm.
Conclusion
Laparoscopy is a good tool for the repair of PIH. With enough experience the technique is safe, feasible, and has no major complications and a small incidence of minor complications. U/S measurement of the IRD is significantly lower than the measurement by laparoscopy. Both sac disconnection only and disconnection with peritoneal closure can be used as laparoscopic treatment of PIH; however, an unacceptable recurrence rate was associated with the disconnection only technique (15% of hernias/20% of cases) in comparison with 0% recurrence in the disconnection and peritoneal closure. Therefore, disconnection only technique should be reserved for cases with IRD <10 mm.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.