
Abstract
Abstract
Background:
Short-term outcomes after laparoscopic pancreaticoduodenectomy (LPD) seem promising, but long-term outcomes of LPD for pancreatic cancer (PC) warrant further investigation.
Methods:
A systematic research of various databases was performed to identify studies analyzing long-term outcomes in LPD versus open pancreaticoduodenectomy (OPD) for PC. Survival parameters of overall survival (OS) and disease-free survival (DFS) were extracted. The search was last conducted before May 23, 2018.
Results:
A total of 10 studies involving 11,180 patients (1437 in LPD and 9743 in OPD) met the final inclusion criteria. Pooled analyses showed that LPD was associated with longer DFS compared with OPD (hazard ratio [HR]: 0.77, 95% confidence interval [CI]: 0.61 to 0.98, P = .033). No significant difference in OS was found between LPD and OPD (HR: 0.98, 95% CI: 0.90 to 1.07, P = .672). In addition, patients of LPD had much shorter time to receive postoperative adjuvant chemotherapy compared with OPD (weighted mean difference: −10.17, 95% CI: −17.90 to −2.45, P = .010).
Discussion:
With regard to long-term survival, LPD is comparable with OPD for PC. Furthermore, LPD is associated with longer DFS compared with OPD. Future well-designed, randomized controlled trials with longer follow-up are still essential to further demonstrate the advantages of LPD for PC.
Introduction
Pancreatic cancer (PC) is one of the most aggressive tumors in the digestive system, which is the fourth leading cause of cancer-related mortality in the United States. 1 Although several kinds of neoadjuvant and adjuvant therapies have been recommended, pancreaticoduodenectomy (PD) is the only potentially curative treatment approach for patients with pancreatic head or periampullary tumors. Because of the complex intra-abdominal dissection and the risk of perioperative morbidity, especially postoperative pancreatic fistula and delayed gastric emptying, PD is still challenging for surgeons ever since Whipple performed the first PD in 1935. 2 In 1994, Gagner and Pomp described the first laparoscopic PD (LPD) in the world. 3 Since then, LPD has become increasingly popular.4–6
In comparison with open PD (OPD), LPD has several advantages in short-term outcomes such as lower intraoperative blood loss and transfusion, fewer postoperative morbidities, faster recovery, and shortened hospital stay.7–9 Although some single studies reported the long-term oncological outcomes of LPD for PC, the conclusions are still inconsistent.10–19 Until now, no meta-analysis has been performed to analyze long-term oncological outcomes of LPD for PC. In this work, we conduct a comparison of long-term oncological outcomes between LPD and OPD. The results indicate that LPD is comparable with OPD for PC with respect to long-term survival. In addition, LPD is associated with longer disease-free survival (DFS) compared with OPD.
Methods
Study selection
Several databases, including Web of Science, PubMed, The Cochrane Library, and Ovid, were retrieved with the following combinations of search terms: “Whipple procedure,” “pancreat*,” “pancreatoduodenectomy,” “pancreaticoduodenectomy,” “PD,” “minimally invasive,” “laparoscopic assisted,” “laparoscopic,” “long-term,” and “survival.” The search was updated to May 23, 2018. References of the obtained studies were manually retrieved to gain additional studies.
Inclusion and exclusion criteria
Each acquired study in this meta-analysis must satisfy the following standards: (1) comparative studies of LPD versus OPD involving observational clinical studies or randomized controlled trials (RCTs); (2) the median follow-up time of the included studies should be more than 12 months, and the studies should have 60 months of follow-up since the first patient; (3) at least one prognostic data item, including overall survival (OS), DFS, or recurrence free survival, should be reported; and (4) if the same authors and/or institutions published more than one publication of the same databases, the study quality, publication year, and sample size were considered, and only one article with high quality was selected. Exclusion criteria were as follows: (1) editorials, expert opinions, abstracts, letters, case reports, and reviews without original data; (2) studies in non-English languages; and (3) studies without available data.
Data extraction and quality assessment
All candidate articles were independently assessed and extracted by 2 reviewers and the following data were used: first author; year of publication; study region; age of patients; months of follow-up; prognostic data; and a hazard ratio (HR) with 95% confidence interval (CI). Inconsistencies were resolved through discussion or an agreement was reached with a third reviewer. For survival data extraction, the HR with 95% CI was directly obtained from the acquired article or estimated using the data, relying on the method reported by Parmar et al. 20 If means and standard deviations of continuous variable data were not provided by the selected study in this meta-analysis, the means and standard deviations were imputed from medians and ranges relying on the method reported by Hozo et al. 21
The quality of nonrandomized studies was independently assessed by 2 reviewers using the Newcastle–Ottawa Scale (NOS). 22 The total scaled scores (0–9 scores) contained three parts, including selection (0–4 scores), outcome assessment (0–3 scores), and comparability (0–2 scores), and high-quality studies were those with scores higher than six.
Statistical analyses
Data analyses were performed using Stata SE 12.0 software. I2 statistics and chi-square Q test were used to identify the heterogeneity of acquired data. A Ph (P value of heterogeneity) <.10 or I2 > 50% indicated significant heterogeneity among the acquired data, and the random-effects model was adopted.22,23 Otherwise, a fixed-effects model was used. To assess the effects of any single study, sensitivity analysis was conducted. Begg's funnel plot and Egger's test were used to assess the publication bias of the article. A P value less than .05 was considered statistically significant.
Results
Eligible studies
A total of 1027 studies were found in the primary literature search. Among the 1027 articles, 228 were duplicate studies. After carefully reviewing the title and abstract, there were 38 articles that compared LPD with OPD for PC. Of the above 38 studies, 28 studies were further excluded due to omission of long-term survival data. Finally, only 10 studies were included in the present meta-analysis, which were published from 2014 to 2018.10–19 The flow diagram is listed in Figure 1.

Flow diagram depicting the process of identifying and selecting studies for inclusion.
There were 7 retrospective design studies and 3 prospective design studies, and 2 matched retrospective design studies were found among the 10 studies. These studies were derived from different countries, including America, China, Korea, and Italy. The NOS was used to assess the quality of nonrandomized studies, and all of the included studies were considered as high-quality studies (higher than six scores). In addition, main characteristics of all the included studies are summarized in Table 1.
Main Characteristics of All the Studies Included in the Meta-Analysis
Statistically significant results are shown in bold.
Mean (SE).
“M” means the HR is calculated using multivariate analysis, “U” means the HR is calculated using univariate analysis.
DFS, disease-free survival; F, female; HR, hazard ratio, obtained by reporting in text (R); LPD, laparoscopic pancreaticoduodenectomy; M, male; NOS score, Newcastle–Ottawa Quality Assessment Scale; OPD, open pancreaticoduodenectomy; NR, not reported; OS, overall survival.
Patient and pathological characteristics
The studies included a total of 11,180 patients, among which 1437 (12.9%) patients were grouped in LPD and 9743 (87.1%) were grouped in OPD. One study 18 showed that patients in the LPD group were older than that of OPD group, but no significant difference was found between LPD and OPD for age in the pooled data (weighted mean difference [WMD] = 0.48, 95% CI: −0.20 to 1.16, P = .167; Table 2). With regard to gender, no significant difference was found (odds ratio [OR] = 1.05, 95% CI: 0.86 to 1.27, P = .636; Table 2). The follow-up time of the included articles ranged from 0.3 to 154.5 months. The study by Chapman et al. 10 showed that LPD had a significantly longer follow-up time compared with OPD, but no significant difference was found in the other studies (Table 1).
Results of the Meta-Analysis
Statistically significant results are shown in bold.
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; M, moderate differentiation; OR, odds ratio; OS, overall survival; P, poor differentiation; Ph, P value of heterogeneity; TNM, tumor–node–metastasis; W, well differentiated; WMD, weighted mean difference.
As shown in Table 3, six studies only have pancreatic ductal adenocarcinoma (PDAC) patients, and the rest four reported periampullary malignancies (PMs). Six studies13,15–19 provided the tumor–node–metastasis (TNM) stage of tumors, and a meta-analysis comparing I, II versus III, IV between LPD and OPD was performed. The results showed that no significant difference was found (OR = 1.21, 95% CI: 0.72 to 2.03, P = .476; Table 2 and Table 3). In addition, no significant difference was found in pathological characteristics of tumor sizes (WMD = −0.12, 95% CI: −0.43 to 0.20, P = .467), histological grade (W, M versus P) (OR = 0.99, 95% CI: 0.58 to 1.69, P = .969), vascular resection (OR = 0.95, 95% CI: 0.66 to 1.37, P = .796), and the number of positive lymph nodes (OR = 0.90, 95% CI: 0.80 to 1.02, P = .097) among the included patients (Table 2 and Table 3).
Pathological Characteristics of Patients Included in the Meta-Analysis
Statistically significant results are shown in bold.
Mean (SE).
The results are shown in different ways.
LPD, laparoscopic pancreaticoduodenectomy; M, moderate differentiation; N, no or negative; NR, not reported; OPD, open pancreaticoduodenectomy; P, poor differentiation; P, positive; PDAC, pancreatic ductal adenocarcinoma; PM, periampullary malignancy; TNM, tumor–node–metastasis; W, well differentiated; Y, yes.
However, LPD was associated with a higher R0 resection rate compared with OPD (OR = 1.21, 95% CI: 1.05 to 1.40, P = .008; Table 2 and Table 3). Furthermore, LPD was also associated with a larger number of harvested lymph nodes in comparison with that of OPD (WMD = 1.17, 95% CI: 0.26 to 2.08, P = .012; Table 2 and Table 3), with significant heterogeneity (I2 = 70.9%; Ph = .001). Then, sensitivity analysis was conducted to assess the effect of any single study. We found two studies reported by Stauffer et al. and Song et al.18,19 with great effects on the result of conversion rate. After excluding studies by Stauffer et al. and Song et al., no obvious heterogeneity was found (I2 = 47.0%; Ph = .093).
Chemotherapy parameters
Five studies10,12–14,16 of the included articles reported neoadjuvant chemotherapy before surgery. A meta-analysis was performed and results revealed that no significant difference was observed between LPD and OPD (OR = 1.06, 95% CI: 0.86 to 1.25, P = .715; Table 2 and Table 3). In addition, six studies10,11,13,15,16,19 provided adjuvant chemotherapy (ACT) after surgery, and results of the meta-analysis showed that no obvious difference was found between LPD and OPD (OR = 1.05, 95% CI: 0.93 to 1.19, P = .421; Table 2 and Table 3).
However, a significantly shorter time to ACT after surgery was found in the group of LPD when compared with the group of OPD (WMD = −10.17, 95% CI: −17.90 to 2.45, P = .010; Fig. 2), with significant heterogeneity (I2 = 94.8%; Ph < .001). Then, sensitivity analysis was conducted. The result revealed one study reported by Croome et al. 13 with great effects on the result. After excluding the study by Croome et al., no obvious heterogeneity was found (I2 = 0.0%; Ph = .455). LPD also had a significantly shorter time to ACT than OPD (WMD = −1.45, 95% CI: −2.91 to 0.00, P = .050).
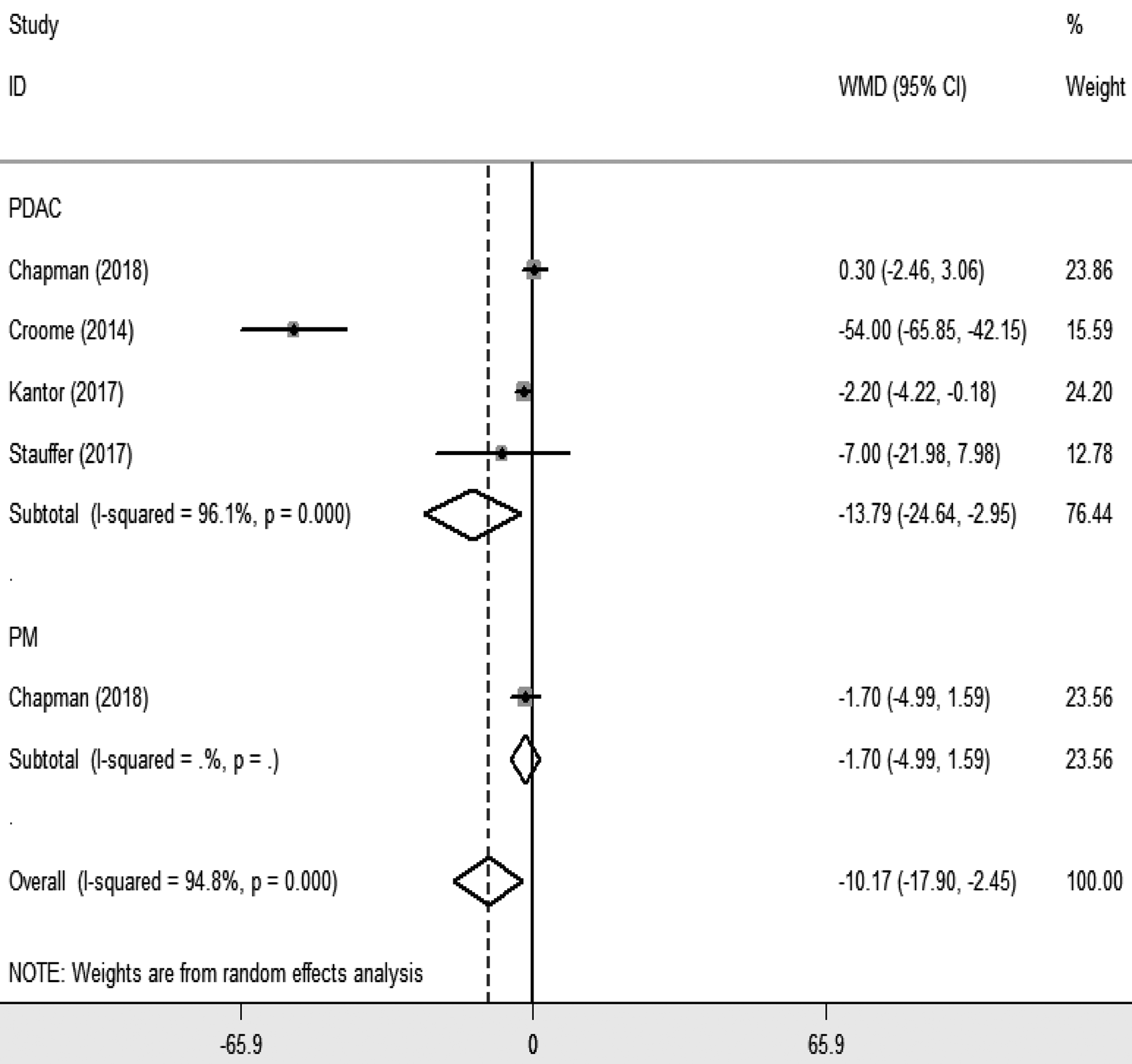
Forest plot illustrating time to ACT after surgery. ACT, adjuvant chemotherapy.
Long-term survival outcomes
There were five studies10,13,14,16,19 that provided data of OS with HRs and 95% CI, and Song et al. 18 provided the raw data. The remaining studies at least provided Kaplan–Meier survival curves. Then, the HR with 95% CI was directly obtained from the acquired articles or the data of HRs with 95% CI acquired from the Kaplan–Meier survival curves were estimated relying on the method reported by Parmar et al. 20 However, the Kaplan–Meier survival curve by Hakeem et al. 15 was not of sufficient quality to allow for generating data of OS. Then, a meta-analysis of data of the remaining nine studies was performed and results showed that no significant difference was found between LPD and OPD (HR = 0.98, 95% CI: 0.90 to 1.07, P = .672; Fig. 3A). Results of the subgroup analysis also showed no significant difference between LPD and OPD in the subgroup of pathology of PDAC and PM.
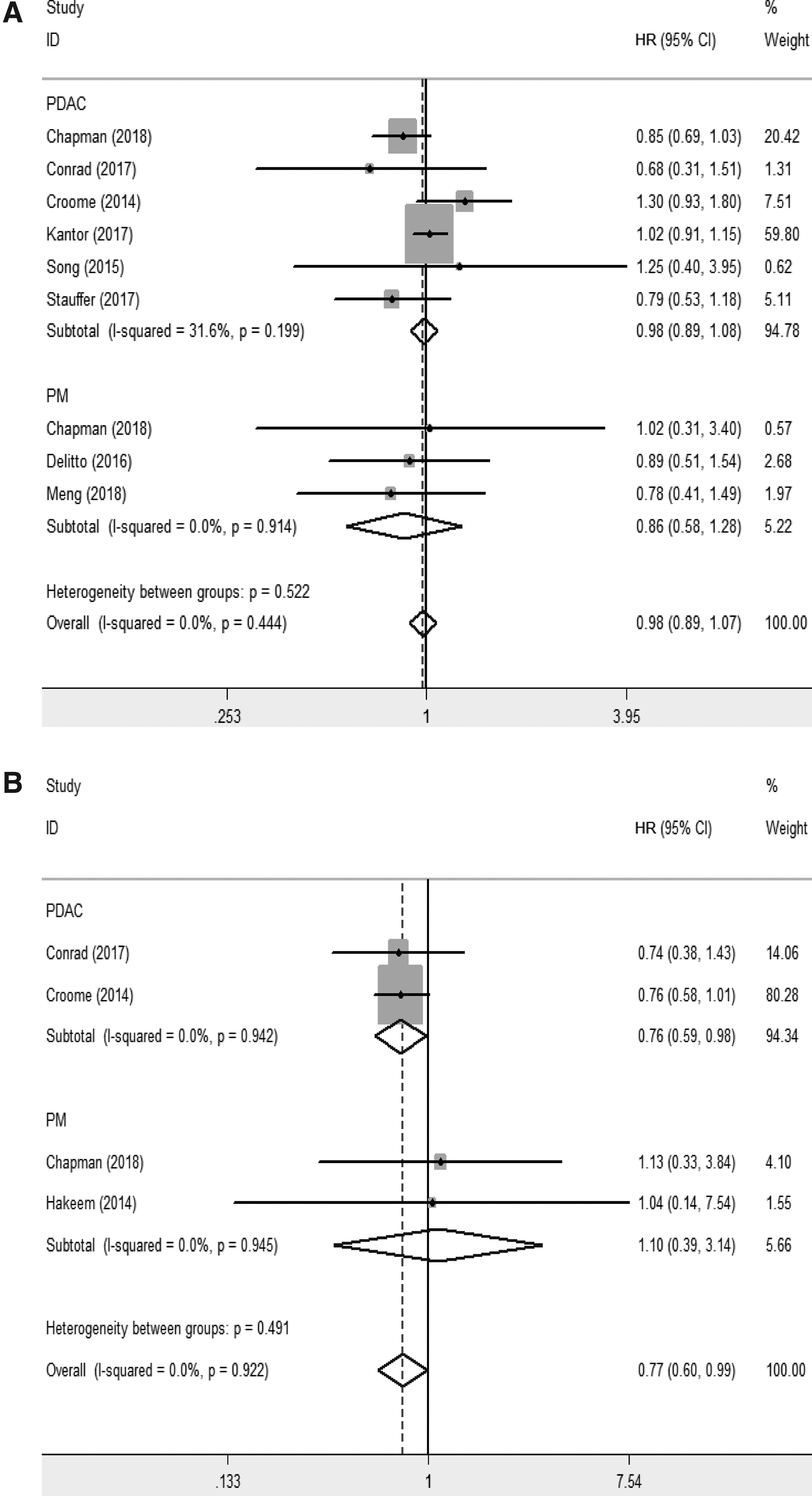
Forest plots illustrating long-term survival outcomes:
Four studies11–13,15 provided the Kaplan–Meier survival curves of DFS. Data of HRs with 95% CI also acquired from the Kaplan–Meier survival curves were estimated, and results showed that LPD was associated with better DFS compared with OPD (HR = 0.77, 95% CI: 0.60 to 1.00, P = .043; Fig. 3B). Results of the subgroup analysis also showed that LPD was associated with longer DFS in the subgroup of the pathology of PDAC (HR = 0.76, 95% CI: 0.59 to 0.98, P = .033; Fig. 3B); however, no significant difference was found between LPD and OPD in the subgroup of the pathology of PM (HR = 1.10, 95% CI: 0.39 to 3.14, P = .852; Fig. 3B). In addition, the data of long-term survival were summarized in Table 4.
Data of Long-Term Survival in the Meta-Analysis
Chapman et al. 11 and Croome et al. 13 provided data of long-term survival with months; the others provided data with years.
DFS, disease-free survival; LPD, laparoscopic pancreaticoduodenectomy; NR, not reported; OPD, open pancreaticoduodenectomy; OS, overall survival.
Publication bias
Begg's funnel plot and Egger's test were used to assess the publication bias of the articles. As shown in the funnel plot of OS (Fig. 4), no evidence of significant publication bias was found.

Funnel plots of OS. OS, overall survival.
Discussion
With continuous technical advances and improvement in laparoscopic training, laparoscopic pancreatoduodenectomy (LPD) has been adopted by expert surgeons in selected patients.3–19,24–26 Compared with open pancreatoduodenectomy (OPD), the short-term surgical outcomes of LPD presented comparable results. Some meta-analyses even showed that minimally invasive pancreatoduodenectomy was associated with lower estimated blood loss, more harvested lymph nodes, more R0 resections, fewer postoperative complications of delayed gastric emptying, and shorter time of hospital stay.7,9 In addition, one recent randomized clinical trial (RCT) of LPD versus OPD for periampullary tumors revealed that LPD was beneficial in terms of intraoperative blood loss, blood transfusion, surgical site infection, and postoperative duration of hospital stay. 27
Due to the limited number of patients included in the single studies and no meta-analysis performed on long-term survival with LPD for PC until now, long-term survival with LPD for PC, which is a major factor to assess the benefits of LPD, is still uncertain. To provide a reliable conclusion that LPD is comparable with OPD with respect to long-term oncological outcomes, this meta-analysis was performed.
The aim of the present meta-analysis is to investigate OS and DFS with LPD versus OPD for PC. Studies without the two factors are excluded in this meta-analysis. The median follow-up time of the included studies should be longer than 12 months. Furthermore, to find whether LPD was better for long-term survival and DFS compared with OPD, we pooled all the data of the included studies to perform a meta-analysis (Table 2). Results revealed that although no significant difference is found between LPD and OPD in OS, LPD is associated with longer DFS compared with OPD. This is the first study to confirm that LPD has comparable long-term survival effectiveness for PC in comparison with OPD.
Long-term survival is one of the important factors to assess the benefits of LPD. Apart from surgical factors such as lymph node resections (LNR), negative margin rate, and postoperative complications, several other factors also affect long-term survival for patients treated by surgery, including demographics of patients, characteristics of the tumor, and adjuvant therapy. For example, Seppänen et al. analyzed 306 PDAC patients treated by surgery, and the overall 1-, 3-, 5-, and 10-year survival rates were 74%, 36%, 22%, and 14%, respectively. 28 Univariate analysis showed that tumor size, histological differentiation grade, LNR, perivascular invasion, and adjuvant therapy significantly affected OS of patients. In the present meta-analysis, all the data were pooled from the included studies in order to find whether LPD could improve long-term survival (Table 2). Although LPD is associated with more harvested lymph nodes and R0 resections in this study, no significant difference is found between LPD and OPD in OS.
Recently, several researches have revealed that R0 resection determined by the 1-mm rule (R01-mm rule) was an independent determinant for postoperative survival. Delpero et al. found that R01-mm rule resection for PDAC was an independent determinant for postoperative survival. 29 In addition, Nitta et al. found that R01-mm rule resection correlated with better OS than R11-mm rule resection, but R0 resection determined by TNM classification (no malignancy infiltrating at any of the resection margins) had no impact on OS when analyzing the impact of margin status on PDAC recurrence and survival following PD. They concluded that R01-mm rule resection might be an independent variable for predicting long-term survival. 30 In the present study, however, most included articles define R0 resection determined by TNM classification. R0 resection, similar to blood loss, transfusion, lymph node harvest, complication rate, and adjuvant treatment, is just one factor affecting long-term survival of PC patients treated by laparoscopic surgery. No significant difference is found between LPD and OPD in OS in the present meta-analysis. In the future, carefully case-matched or RCT studies relying on R01-mm rule resection are required to analyze long-term survival with LPD versus OPD for the treatment of PDAC.
Interestingly, our study reveals that LPD is associated with better DFS compared with OPD. Potential reasons may be reduced physiologic and immunologic effects of LPD and the enhanced ability of patients treated with LPD to receive timely and complete postoperative adjuvant therapy.13,31 In patients with colon cancer, Biagi et al. revealed that the increasing time to ACT correlated with a decrease in survival. 32 Similarly, the increasing time interval to ACT is significantly associated with decreased survival in patients with ovarian cancer. 33 Recently, the European Study Group for Pancreatic Cancer-3 (ESPAC-3) found that completion of all six cycles of ACT was predictive of OS after surgery for PDAC. They also observed that if patients could not complete six cycles of therapy, chemotherapy started within 12 weeks was an important factor for long-term survival. 34 In the present study, LPD had a significantly shorter time to ATC after surgery compared with OPD, which was associated with fewer complications and faster recovery in patients of LPD. Therefore, it can be assumed that LPD can significantly shorten the time to ATC, which may prolong DFS of patients treated with surgery. However, all the data of DFS were estimated from Kaplan–Meier survival curves in our meta-analysis, and the follow-up time of the included studies was not equal. Reporting bias may exist in the data of DFS. The data of DFS just provided some reference values in the present meta-analysis. Therefore, carefully case-matched or RCT studies are required to prove the above hypothesis in the future.
A number of limitations in the present meta-analysis of nonrandomized studies existed, which should be acknowledged and carefully considered when interpreting the results. First, all studies included in the meta-analysis are non-RCTs (NRCTs) in design, which may be liable to cause selection bias and exaggerate the effect of the approaches. Pooling data from NRCTs is a debated topic in the field of meta-analysis. Nevertheless, several studies proved that results derived from studies of well-designed NRCTs may be reliable.35,36 In this meta-analysis, all of the 10 included studies are well-designed NRCTs, according to the NOS. Second, characteristics of the populations as well as tumors, R0 resection, transaction devices in laparoscopic surgery, the learning curve of surgeons, and definitions of outcomes vary considerably among the included studies, which may cause heterogeneity and impact the reliability of our results. For example, Park et al. found that the 5-year DFS rate of stage III disease in the expert period (85%) was better than that of the learning curve period (53.3%; P = .046) in laparoscopic right hemicolectomy. 37 In laparoscopy-assisted distal gastrectomy for gastric cancer, however, Hu et al. revealed that long-term outcomes were not sacrificed during the learning stage. 38 Therefore, these factors should be included in the analysis of long-term survival in future, which certainly plays a role in the findings of this analysis. Finally, due to the limited or nonexistent descriptive statistics of the included studies, it is impossible to generate more in-depth comparative results, such as the longer follow-up and recurrence rate.
In conclusion, results of our meta-analysis indicate that LPD for PC is comparable with OPD with respect to long-term survival. In addition, LPD is associated with better DFS compared with OPD. However, evidence is still limited due to the lack of high-quality RCTs. Additional prospective and multicenter RCTs with longer follow-up are needed for further investigation in the future.
Footnotes
Acknowledgments
The authors thank all colleagues of the department of general surgery in The Second Affiliated Hospital of Nanchang University. The authors also thank the professors from The First Affiliated Hospital of Nanchang University for reading and commenting on the manuscript. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' Contributions
J.C. conceived the study; L.P. collected data, performed the data analysis, and wrote the article; Z.Z. and Z.C. edited the article; and all authors read and approved the final manuscript.
Disclosure Statement
No competing financial interests exist.