
Abstract
Abstract
Background/Purpose:
During laparoscopic excision of choledochal cysts (CDCs), if duodenum injury is encountered, conversion to open repair of duodenal injury is often the standard approach. This study evaluates if it is safe to repair the duodenal injury laparoscopically in CDC children.
Materials and Methods:
CDC children who underwent single-incision laparoscopic repair for iatrogenic duodenal injury between October 2013 and September 2018 were reviewed. According to the pathophysiology, duodenal injuries were categorized into two subtypes: Type 1: injury caused by severe adhesions between perforation site at distal CDC and the duodenum; Type 2: anatomical variation, that is, distal CDC shared the common wall with the duodenum. A transabdominal wall suture was placed through distal end of CDC. Relying on the adhesion between distal CDC and duodenum, the injured duodenum can be clearly exposed when the assistant pulled on the retraction suture. The duodenal injury was repaired by a two-layer 5-0 polydioxanone running suture. The distal CDC was transected after repair was accomplished.
Results:
Five children were reviewed (Type 1: n = 4, Type 2: n = 1). Median age at surgery was 1.2 years. Median operative time was 4.0 hours. Median postoperative hospital stay was 7 days. Median duration of full diet resumption and drainage were 5 days, respectively. Median follow-up period was 31 months. Liver function tests and serum amylase levels were normalized within 1 year. None of patients had intestinal leak, anastomotic stenosis, bile leak, cholangitis, pancreatic leak, pancreatitis, or adhesive intestinal obstruction.
Conclusions:
Single-incision laparoscopic repair for iatrogenic duodenal injury in CDC children is safe and effective.
Introduction
In children with choledochal cysts (CDCs), the distal CDC and duodenum occasionally shares a common wall as a result of dense adhesion 1 at distal perforated site or variation of anatomy. Localized submucosal dissection cannot be carried out. Thus, it leads to almost inevitable duodenal injury. 1 Because the injury site is adjacent to the dissection area of distal pancreatic segment of CDC, it is difficult to expose and repair under the same laparoscopic exposure. Conventionally, it is often converted to open approach to repair duodenal injury in laparoscopic bile tract surgery. 2
We herewith designed a retraction technique and repaired duodenal injury in the same laparoscopic setting. This study is to evaluate the efficacy of single-incision laparoscopic repair for iatrogenic duodenal injury in CDC children.
Materials and Methods
CDC children who successfully underwent single-incision laparoscopic repair for iatrogenic duodenal injury between October 2013 and September 2018 were reviewed. The procedures were carried out by the surgical team. Ethics approval from the Ethics Committee of Capital Institute of Pediatrics was obtained. Written informed consents were obtained from the parents of the CDC patients before surgeries.
The patient was placed in supine anti-Trendelenburg position. A vertical umbilical incision was made. An extra-long 5-mm 30° laparoscope (26046BA; Karl Storz GmbH & Co. KG, Tuttlingen, Germany) was inserted through the camera port, which was placed in the midline fascial incisions. Carbon dioxide pneumoperitoneum was established with the pressure at 8–12 mmHg. Two 3-mm conventional laparoscopic instruments were inserted through working ports that were placed lateral to the camera port on either side, at the horizontal ends of the umbilical incision (Fig. 1). The CDC excision and Roux-Y hepaticojejunostomy was carried out as described in the previous report. 3
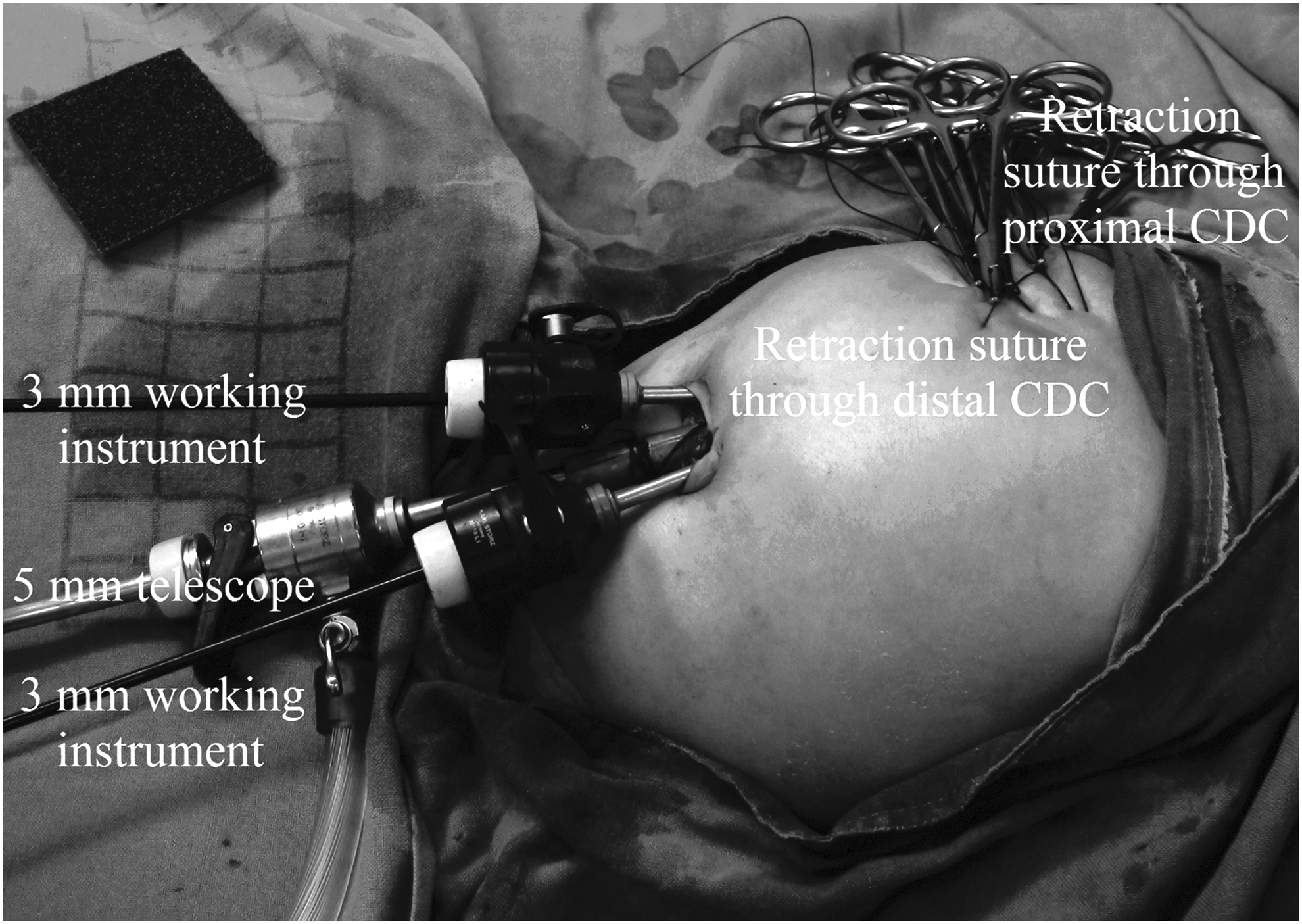
Retraction suture placements and instrument arrangements. CDC, choledochal cyst.
According to the pathophysiologies, the duodenal injuries were categorized into two subtypes: Type 1: injury caused by severe adhesions between perforation site at distal CDC and the duodenum (Fig. 2a, 2b); Type 2: distal CDC shared the common wall with the duodenum (Fig. 2c, 2d).
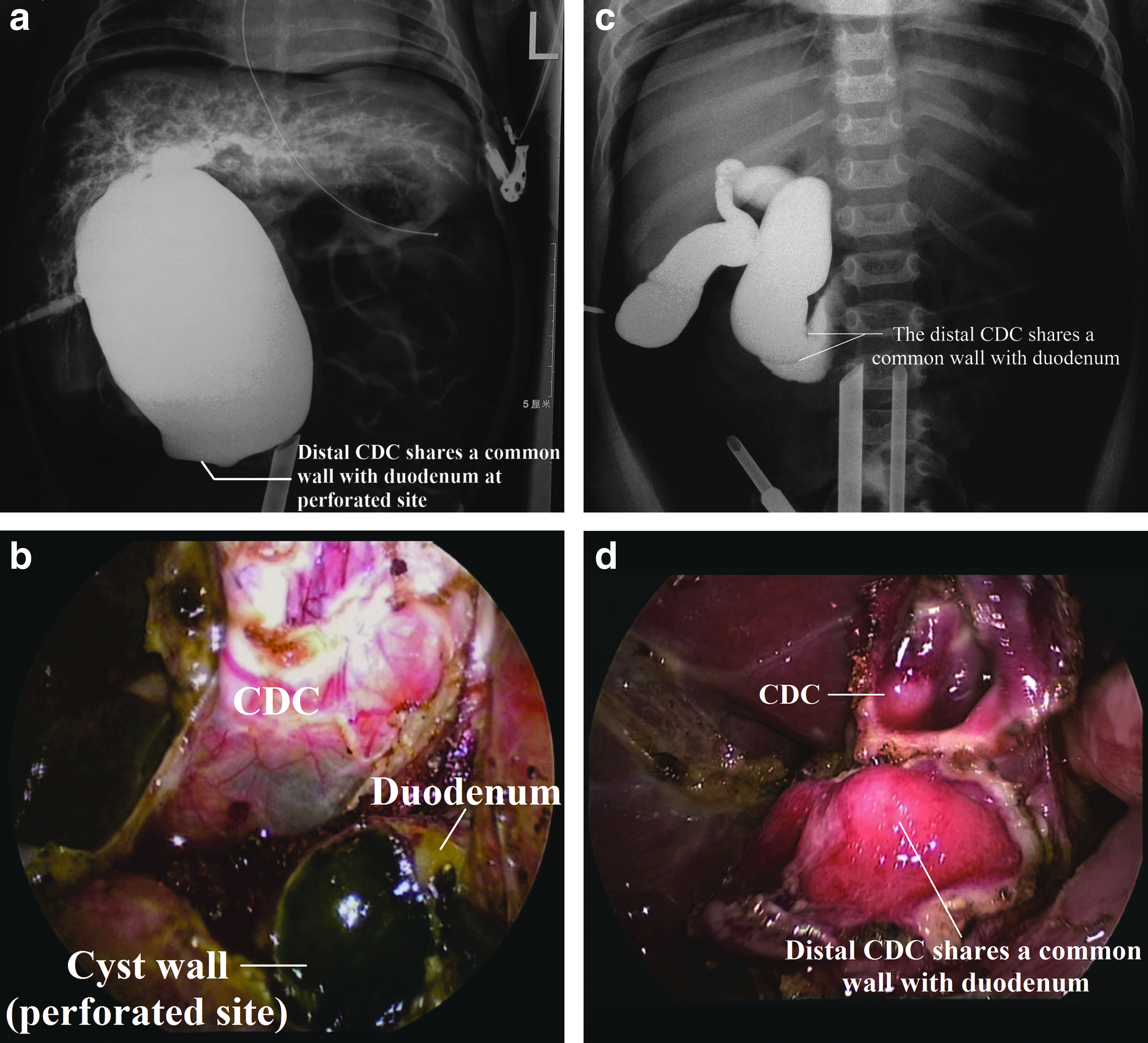
Intraoperative cholangiograms of CDCs.
A transabdominal wall suture was placed through distal CDC (Fig. 3a). Relying on the adhesion between distal CDC and duodenum, the injured duodenum could be adequately exposed when the assistant pulled on the retraction suture (Fig. 3a). The duodenal injury was repaired by a two-layer 5-0 polydioxanone (PDS) running suture (Fig. 3b-1, 3b-2, 3c). The distal CDC was transected after the repair was accomplished (Fig. 3d).
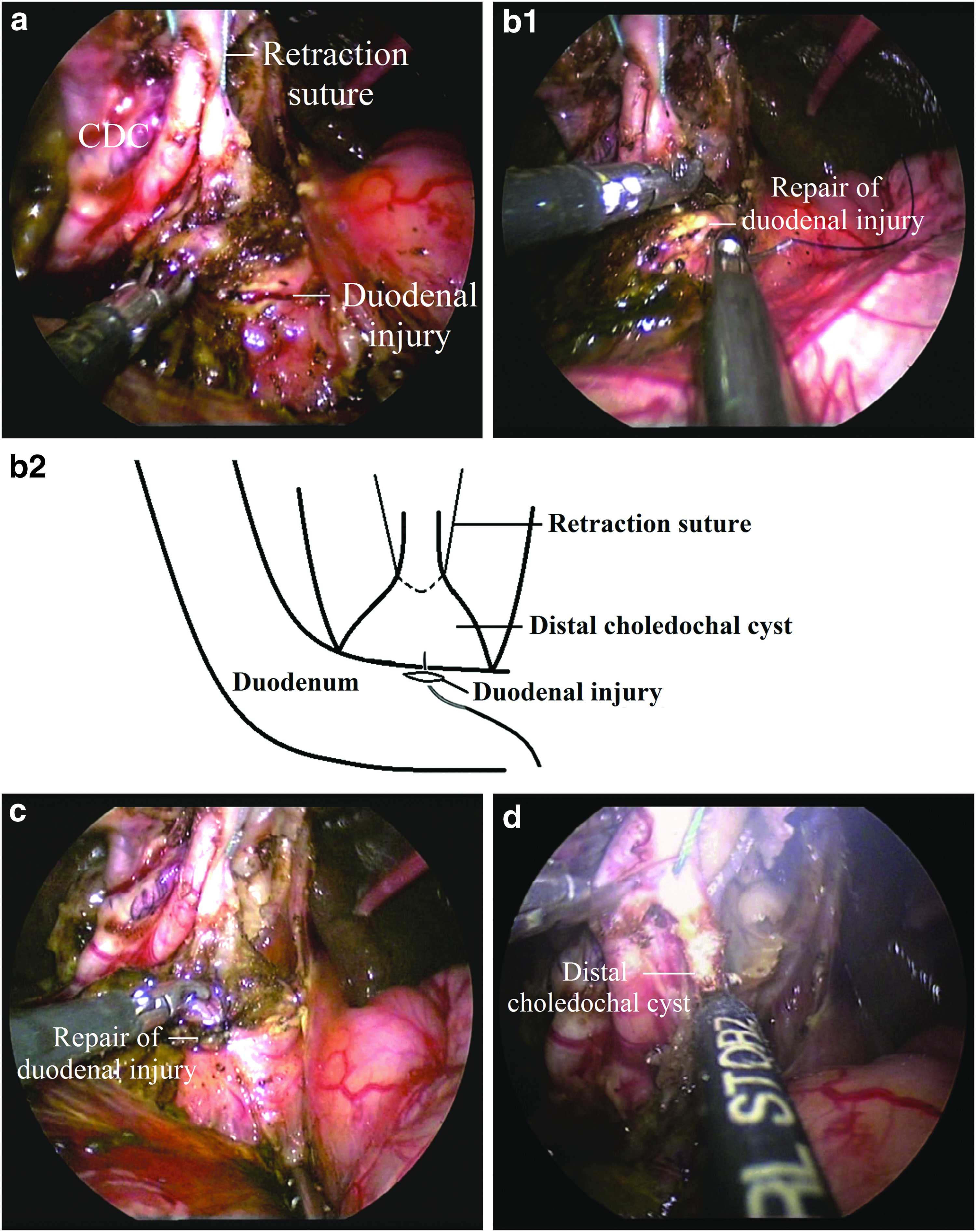
Single-incision laparoscopic repair of iatrogenic duodenal injury in children with CDCs.
Patients were followed up in our clinic postoperatively at 1, 2, 3, and 6 months and every 6 months thereafter. The laboratory results and ultrasonographic findings were reviewed. The upper gastrointestinal studies were conducted to detect whether patients had Roux loop reflux.
Results
Between October 2001 and September 2018, 1808 CDC children successfully underwent laparoscopic cyst excision and Roux-Y hepaticojejunostomies in our center. Of them, 5 (0.2%) encountered intraoperative duodenal injuries. The first injury was caused by anatomical variation in 2013, that is, Type 2, the distal CDC shared the common wall with duodenum. The remaining four injuries occurred in perforated CDCs, that is, Type 1, after we extended laparoscopic technique into treatment of perforated CDCs. The perforation site was sealed by the duodenum. They formed a common wall. All injuries located in the horizontal portion of the duodenum. Hence, the papilla of Vater remained intact. Because we started single-incision laparoscopic cyst excision and hepaticojejunostomy since 2011, all duodenal injuries were repaired by single-incision laparoscopic techniques.
The median age at surgery was 1.20 years (range: 4.3 months–5.05 years). The median operative time was 4.0 hours (range: 3.75–5.33 hours). The median postoperative hospital stay was 7.0 days (range: 6–8 days). The median duration of full diet resumption was 5.0 days (range: 3–6 days). The median duration of drainage was 5.0 days (range: 3–6 days).
The median follow-up period was 31 months (range: 12–60 months). Postoperative liver function tests and serum amylase levels were normalized within 1 year. None of the patients had intestinal leak, anastomotic stenosis, bile leak, cholangitis, intrahepatic reflux, pancreatic leak, pancreatitis, Roux-loop obstruction, or adhesive intestinal obstruction.
Discussion
Incidental injury of duodenum is a rare morbidity in definitive surgery of CDC. It is usually attributed to dense adhesion 1 at perforated site or anatomical variation. We demonstrated for the first time that in experienced hands, the duodenal injury could be repaired without conversion to open surgery.
Investigations
Preoperative computed tomography scans and intraoperative cholangiograms are very helpful to detect the defect. The images with a sign of “straight line” between distal CDC wall and the duodenum indicated that they shared a common wall (Fig. 2a, 2c). Careful inspection is necessary in the surgery.
Surgical strategy
Prevention of injury
In case that the dense adhesion obscured the border between cyst wall and duodenum, the cyst wall was incised immediately proximal to the dissection area with indistinct border. The margin between cyst wall and duodenum can be identified in direct vision. The dissection was carried out along the direction from incised site to obscure site, and as close as possible to the cyst wall to prevent duodenal injury;
Localized submucosal dissection was carried out at the perforated site that was sealed by duodenum to minimize the injury. The severe inflammatory cyst wall can be bitten by forceps along submucosal layer gradually.
Management of inevitable injury
In case that the common wall between distal CDC and duodenum cannot be dissected along submucosal layer, the duodenal injury was inevitable. It is difficult to expose and precisely repair using the same setting with umbilicus-to-hepatic hilum direction telescope in laparoscopic definitive surgery because the injured site (1) located at adjacent area between duodenum and the CDC, that is, the posterior wall of duodenum. The overlap of anterior and posterior duodenal wall was an obstacle for posterior wall repair; (2) the injury is located deep and close to distal pancreatic segment of CDC.
According to conventional surgical logistics, the distal CDC was transected when distal dissection was accomplished. The duodenum wall collapsed without suspension by inflammatory adhesions. Conventionally, it is often converted to open approach to repair duodenal injury in laparoscopic bile tract surgery. 2 We herewith modified the procedure and refrained from transecting the distal CDC before duodenal injury repair. Relying on the dense adhesion between distal CDC and duodenum, we placed a retraction suture through the distal CDC, opposite to duodenal injured area. The injured area was exposed when assistant pulled on the retraction suture. Hence, the duodenal injury can be repaired precisely by laparoscopic approach.
Our results demonstrated that single-incision laparoscopic repair for iatrogenic duodenal injury in CDC children is safe and effective in experienced hands.
Footnotes
Disclosure Statement
No competing financial interests exist.