
Abstract
Abstract
Enterobius vermicularis associated appendiceal colic and acute appendicitis are rarely encountered in the United States. The 9-year-old patient described in this case presented with right lower quadrant abdominal pain, nausea, and vomiting consistent with acute appendicitis and was brought to the operating room for an appendectomy. Intraoperatively a pinworm, E. vermicularis, was visualized and the presumptive diagnosis of acute appendicitis was revised to E. vermicularis associated appendiceal colic. Retrospective review of the preoperative imaging demonstrates the first reported ultrasonographic image of pinworm inhabitance within the appendiceal lumen. The patient was treated postoperatively with a course of albendazole and recovered appropriately. This article reviews the geographic epidemiology, pathophysiology, surgical, and medical treatment recommendations in the management of E. vermicularis diseases of the appendix. Through dissemination of this ultrasonographic imaging, the authors hope to inform other providers about E. vermicularis associated appendiceal colic and reduce the incidence of avoidable surgeries.
Introduction
E
Case Report
A 9-year-old girl was transferred from an outside hospital to Children's National Medical Center with 2 days of periumbilical pain migrating to the right lower quadrant of the abdomen. She had low-grade fevers, multiple episodes of emesis, and endorsed anorexia. She denied perianal itching and recent sick contacts. Physical examination demonstrated focal right lower quadrant tenderness to palpation consistent with focal peritonitis. Laboratory data were normal, white blood cell count (8.7 × 10 3 cells/mL) was with normal differentiation, devoid of eosinophilia. Abdominal ultrasonography showed wall hyperemia, edema, and was interpreted as presence of an obstructive appendicolith consistent with acute appendicitis. She received intravenous antibiotics and underwent a laparoscopic appendectomy. Intraoperatively, the appendix appeared inflamed at the tip and body with a healthy appearing appendiceal base consistent with uncomplicated acute appendicitis. The appendix was sharply divided after an endoscopic looped suture was secured at the appendiceal base. A helminth was then visualized moving within the intraluminal appendiceal stump (Fig. 1) and was subsequently retrieved intact. Gross evaluation of the appendix revealed another helminth within the lumen. Pathological evaluation of the appendix demonstrated a normal appendix without any eosinophilic inflammation. Retrospective review of the original radiographic imaging demonstrated a serpiginous hyperechoic streak, consistent with helminth inhabitation (Fig. 2). The patient was subsequently treated with albendazole for E. vermicularis (pinworm) infection with resolution of abdominal symptoms.
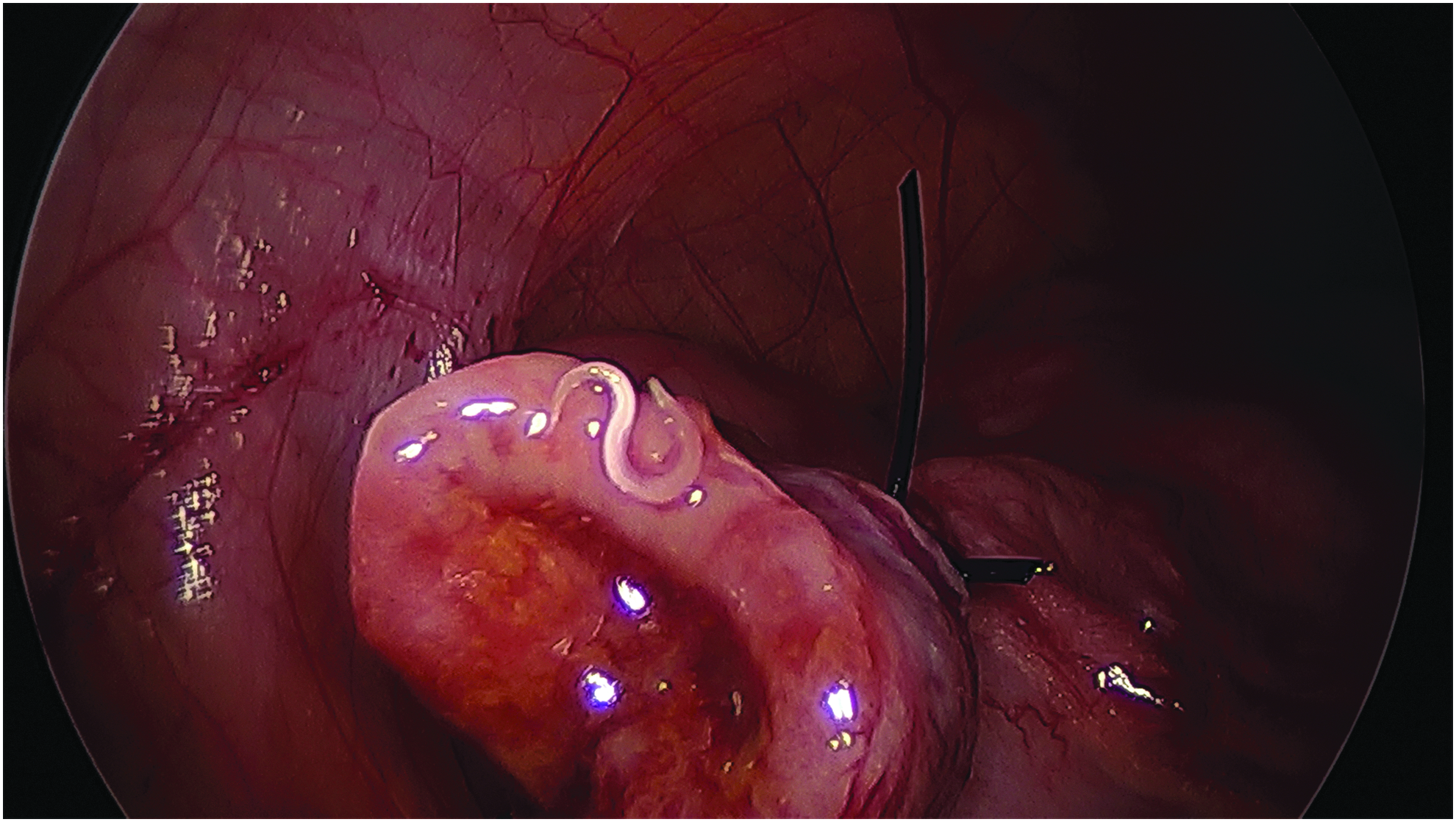
Intraoperative image. An intraoperative image taken of the Enterobius vermicularis helminth on the appendiceal stump after division of the appendix.
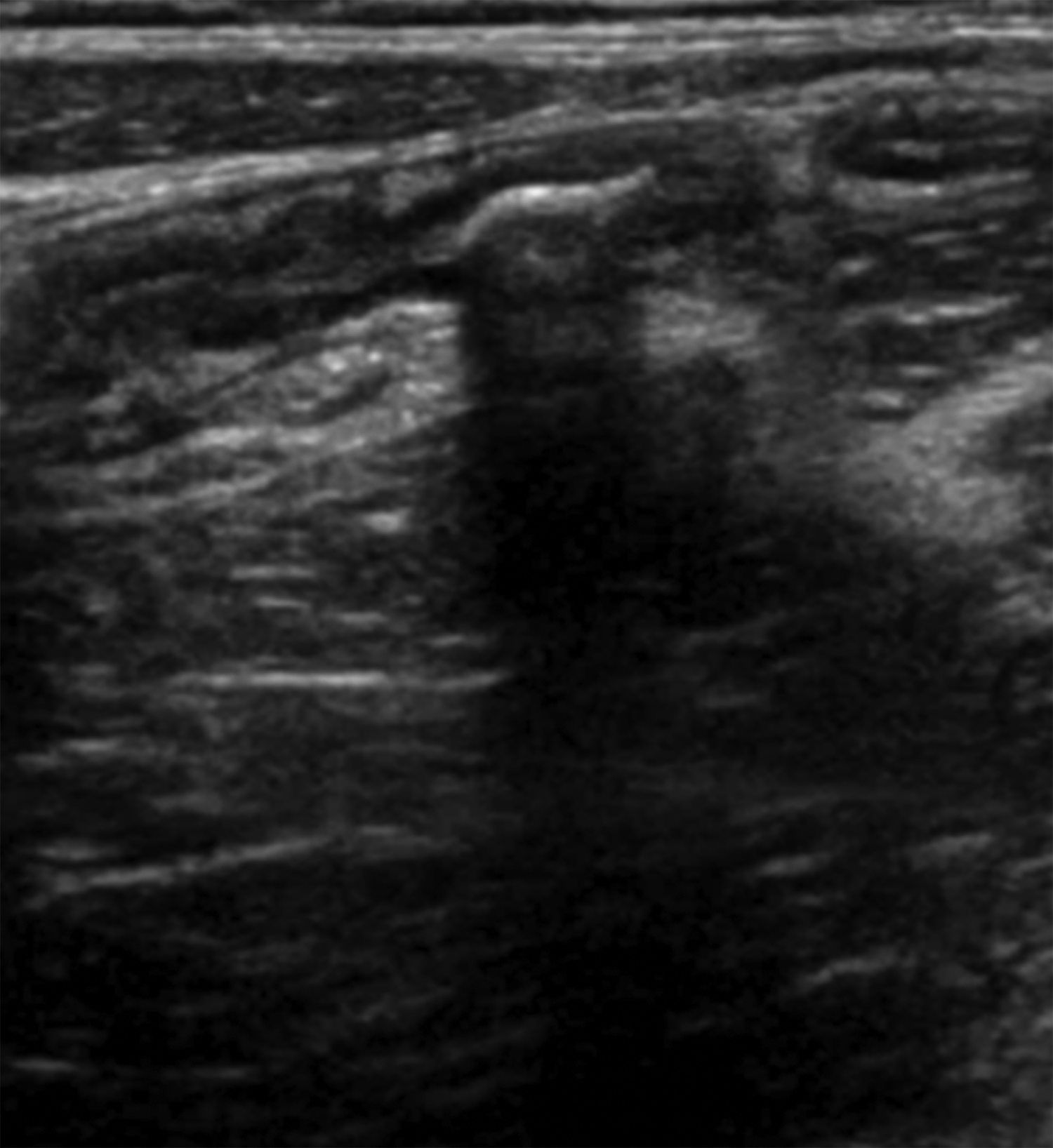
Abdominal ultrasonography. Abdominal ultrasonography showing visualization of the Enterobius vermicularis helminth measuring 6 mm with posterior shadowing. The radiological interpretation was initially misread as an obstructive appendicolith.
Discussion
Parasitic inhabitance with E. vermicularis has been afflicting humans for centuries, having first been referenced in medical texts by Hippocrates circa 490 BC. 1 It is considered the most common helminth infection worldwide, affecting between 4% and 50% of children globally.1,2 It is transmitted through the fecal–oral route with eggs remaining viable for 2–3 weeks on fomites such as human clothing or bedding. 3 Once ingested, adult worms most commonly live in the ascending colon and vermiform appendix eliciting gastrointestinal symptoms and evoking inflammation of the anatomic regions of inhabitance. 3 The most common manifestation of E. vermicularis is perianal pruritus that results from the migration of the female pinworm to lay its eggs in the perianal area. 1 However, it has also been noted to present as a mesenteric abscess, urinary tract infections, salpingitis, and appendicitis.3,4 Before improved sanitary conditions, in 1899 Still reported that 19% of acute appendicitis occurred in conjunction with E. vermicularis infestation. 2 Throughout the next century, the association of the helminth and appendicitis became less corollary and has only recently become more apparent internationally.3–8
Although E. vermicularis has become a less common etiology of appendicitis globally, it still remains more common internationally. Specifically in Turkey and Pakistan, E. vermicularis was considered the etiology for 2.8% of 2956 cases of acute appendicitis in Pakistan and for 2% of 665 cases of acute appendicitis in Turkey.5,6 In Western countries, it accounts for 1.5% of cases in the United Kingdom and 1.4% of cases in the United States.2,3 It remains unclear why females show a predominance in cases of appendicitis caused by E. vermicularis, ranging from 74% to 76%.5,7 Differentiating appendiceal colic from acute appendicitis is challenging and may often only be discovered after histological evaluation of the appendix. Patients with E. vermicularis are more likely to have an Alvarado score <6 (61% versus 28%; P = .01) when compared with a patient with acute appendicitis.3,9 E. vermicularis appendiceal colic is less likely to manifest a leukocytosis, and only 14% will demonstrate an eosinophilia.3–5
Historically, appendiceal colic associated with E. vermicularis was believed to result from an acute inflammatory response but other theories exist. 5 The current hypothesis is that the nematode in the lumen transiently obstructs the lumen of the appendix, and this intermittent obstruction manifests as appendiceal colic.3,10 Female pinworms can grow up to a size of 10 mm in length, more than an adequate size to obstruct the appendiceal lumen. All 9 cases examined by Akkapulu et al. in 2014 demonstrated E. vermicularis within the lumen of the appendix.3,4 Further supporting this theory, of 13 cases of E. vermicularis associated appendiceal colic, Fleming et al. in 2015 demonstrated that only 30% demonstrated evidence of acute inflammation. 4 However, in the presence of a fecalith, 75% of cases manifested acute inflammation. 8 Other studies describe lymphoid hyperplasia to be more frequently associated with E. vermicularis associated appendiceal colic.4,5 A literature review performed by Arca et al. found that of the 2308 appendices inhabited with E. vermicularis, only 286 (12.4%) were associated with appendiceal inflammation. 2 In fact, patients infested with E. vermicularis who undergo appendectomy are 5–10 times more likely to have no evidence of inflammation on pathological examination. 11 Pathophysiology of the relationship between inflammation and E. vermicularis remains nebulous and unsubstantiated, leading some authors to postulate whether E. vermicularis is protective against appendiceal inflammation. 7
The discrepancy of E. vermicularis associated appendiceal colic and E. vermicularis associated acute appendicitis has resulted in variable author recommendations. Fleming et al. call for better methodologies of distinguishing E. vermicularis to prevent unnecessary surgeries. 8 In contrast, Ahmed et al. have shown that E. vermicularis associated appendiceal colic can progress and result in perforation of the appendix in 6% of cases and necrosis of the mucosal wall in 9.5% of cases, and this risk is enough to justify surgical intervention. 5 Our case report demonstrates the challenges facing the clinician, especially in a geographic location not endemic to E. vermicularis. The patient's clinical presentation and radiological findings were initially consistent with acute appendicitis. The patient's laboratory values were less consistent with acute appendicitis, although this may have been confounded by early antibiotic administration at the outside hospital emergency department. Retrospectively, the lack of leukocytosis and eosinophilia was consistent with pinworm associated appendiceal colic. Intraoperative hyperemia and edema of the appendix appeared consistent with a preoperative diagnosis of acute appendicitis, and it was not until division of the appendix and visualization of the mobile helminth that the diagnosis was changed. Pathological evaluation showed a normal appendix, and although the radiological and surgical teams were unable to visualize the helminth on ultrasonography, a retrospective review clearly demonstrated an obvious helminth within the lumen of the appendix. To our knowledge, this is the first documented appendiceal helminth identified on ultrasonography, and should help future identification of pinworm if clinically suspected.
When diagnosed intraoperatively, E. vermicularis should be treated based upon several principles. If any pinworms are appreciated, they should be controlled with thermal ablation or endoscopic suctioning. 10 A specimen bag should be implemented for removal of the appendix. 10 After removal of the appendix, the port sites, abdominal cavity, and pelvis should be meticulously examined for any spillage before closing. 10 These steps should be taken to protect against potential intraperitoneal contamination, which can be complicated by omentitis, pelvic inflammatory disease, and pelvic peritoneal granulomas. 10 Concurrent with surgical treatment, patients should be treated with a dose of mebenedazole, pyrantel pamoate, or albendazole at the time of diagnosis, and another dose 2 weeks after treatment. 12 Household contacts do not need to be treated for E. vermicularis unless more than one household member is affected or if the infection recurs. 12 Finally, an ophthalmological examination may be performed to ensure absence of ocular pinworm.
Footnotes
Disclosure Statement
No competing financial interests exist.