
Abstract
Abstract
Objective:
The aim of this retrospective study was to present our surgical experience in patients with bronchiectasis who underwent thoracoscopy and to compare the results with those of patients who underwent thoracotomy.
Methods:
We analyzed the medical records of patients who underwent lung resection to treat bronchiectasis through video-assisted thoracoscopic surgery (VATS) or open lung resection between November 2012 and November 2017.
Results:
In total, 99 patients were enrolled. Forty-nine patients with bronchiectasis underwent VATS lung resection and 50 patients underwent thoracotomy. The patients in the VATS group were older (P = .025), but no difference was observed in blood loss (P = .62) or morbidity (P = .67) between the two groups. The patients in the VATS group had a shorter duration of chest tube placement (P = .01) and length of hospital stay (P = .04) but a longer operative time (P = .01). No significant difference was found in symptom improvement between the two groups (P = .694).
Conclusions:
Surgical resection for bronchiectasis can be performed with acceptable morbidity and can lead to significant relief of symptoms. Video-assisted thoracoscopic lung resection for localized bronchiectasis is a safe and efficient procedure that results in good recovery.
Introduction
Bronchiectasis is a chronic respiratory disease characterized clinically as a syndrome consisting of cough, sputum production, and bronchial infection and radiologically by abnormal and permanent dilatation of the bronchi. 1 The prevalence of diagnosed bronchiectasis is likely increasing due to aging population and increased use of radiological investigations. 2 Before the antibiotic era, bronchiectasis occurred frequently and was considered a morbid disease with high mortality. 3 After the advent of effective antibiotics, the incidence of bronchiectasis in developed countries has decreased over the past half century. In developing countries, bronchiectasis still constitutes an important problem. 4 Surgical resection has been used to treat bronchiectasis since the end of the 1930s. 5
Currently, surgery for bronchiectasis still plays an important role in thoracic surgical practice in China. Despite advances in thoracic surgery, the optimal treatment approach of bronchiectasis remains controversial.6–9 The aim of this retrospective study is to present our surgical experiences regarding bronchiectasis treated through VATS compared with that treated through traditional thoracotomy.
Materials and Methods
The Institutional Review Board of Harbin Medical University approved this study. Informed consent was not required for this retrospective study.
Patients and surgery indications
We reviewed the medical records of consecutive patients who underwent surgery for bronchiectasis between November 2012 and November 2017 at the Department of Thoracic Surgery of the Second Hospital Affiliated to Harbin Medical University, China. Data were obtained from the hospital's database and medical records. The demographic features and symptoms of patients, surgical approach, morbidity, mortality, and outcomes after surgical management were analyzed. Preoperative preparation consisted of a detailed history, physical examination, laboratory examination, pulmonary function test, cardiac ultrasound, electrocardiogram, and high-resolution computed tomography scan. Sputum samples were collected and sent for microbiological culturing. Patients with positive cultures were administered systemic antibiotics, based on culture results. Prophylactic antibiotics were administered for 24 hours before surgery.
The surgical indications for bronchiectasis in our department include the following: localized bronchiectasis documented by high-resolution computed tomography and obvious symptom such as chronic productive cough, repeated or significant hemoptysis, and recurrent pulmonary infections and failure of medical treatment. The selection of the surgical approach was mainly based on the preference of surgeons. Follow-up was conducted by telephone and was performed for all patients for a mean period of 33.6 months (range 5–65 months). Patients were assessed for symptoms such as dyspnea, hemoptysis, frequency of acute infection, and daily sputum volume at the time of follow-up. Symptom relief was classified as follows: symptoms disappeared, symptoms improved, or symptoms did not improve (no reduction in preoperative symptoms), or worsened (frequent exacerbation requiring hospitalization).
Operative technique
A double-lumen endotracheal tube was used in all patients to avoid the possibility of intraoperative contamination of the contralateral lung. Patients were placed in the lateral decubitus position, and one-lung ventilation was established. Forty-nine patients were treated by video-assisted thoracoscopic surgery (VATS) and posterolateral thoracotomy was performed on 50 patients. A lobectomy was performed if the disease was limited to the single lobe, whereas pneumonectomy was performed when the entire lung was affected. Patients with limited disease symptoms underwent segmentectomy.
For VATS, A 10 mm incision was made in the seventh intercostal space to insert the camera. A 3 cm incision was made in the fifth intercostal space without spreading the ribs. If severe adhesions were present in the thoracic cavity, blunt mobilization using a finger was recommended to establish a tunnel first, and electrocautery was performed to achieve sharp dissection. The pulmonary artery was identified and dissected first. Typically, the division of the arteries was performed before the division of the veins to avoid congestion of the lobe. The major pulmonary veins and the bronchus were dissected separately. For the thoracotomy group, lung resection was performed through a posterolateral thoracotomy. The chest was entered through the fifth or sixth intercostal space, and a retractor was used to obtain satisfactory exposure.
At the end of the operation, one chest tube (28F) was placed. Air leak lasting longer than 5 days was considered prolonged air leak (PAL). Chest tube removal was usually performed 1 day after air leak cessation, based on pleural drainage (<100 mL/day) and the absence of thoracic contamination.
Statistical analysis
Statistical analysis was performed with SPSS v.24. The Kolmogorov–Smirnov test was used to analyze the distribution of variables. For normally distributed data, an unpaired t-test was used to compare the values. Levene's test was used to compare the homogeneity of variance. Categorical variables were compared through the χ 2 test with the Monte-Carlo method when appropriate. A P value <.05 was considered statistically significant in all cases.
Results
Between November 2012 and November 2017, 99 patients with bronchiectasis were treated in our department. Among them, 49 patients underwent attempted VATS lung resection and 50 patients underwent thoracotomy. The patient characteristics are given in Table 1. The patients in the VATS group were older (52.84 ± 8.66 versus 49.25 ± 10.74). In the VATS group, the chief symptoms included productive cough in 8 patients (16.3%) and hemoptysis in 41 patients (83.7%). Five patients were considered emergency cases due to massive hemorrhage. In the thoracotomy group, the chief symptoms included productive cough in 23 patients (46%) and hemoptysis in 27 patients (54%). Two patients were considered emergency cases due to massive hemorrhage. In the VATS group, 11 patients had positive microorganism cultures from sputum and 14 patients had a positive sputum culture in the thoracotomy group. Pleural adhesion was observed in 46 patients (93.9%) in the VATS group and 8 of these patients had severe adhesion. In the thoracotomy group, pleural adhesion was observed in 45 patients (90%) and 9 patients had severe adhesion. No conversion to open surgery occurred in the VATS group.
Characteristics for Video-Assisted Thoracoscopic Surgery and Thoracotomy Patients
COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; TB, tuberculosis; VATS, video-assisted thoracoscopic surgery.
The distribution of surgical procedures is given in Table 2. Most patients underwent lobectomy, followed by lobectomy and segmentectomy, bilobectomy, segment resection, and pneumonectomy. No difference was observed in blood loss between the two groups. Patients in the VATS group had a shorter duration of chest tube placement and length of hospital stay. The operative time was longer in the VATS group (as given in Table 3). No intraoperative or postoperative deaths occurred. No bronchopleural fistula or respiratory insufficiency was observed in the two groups (as shown in Table 4). In the VATS group, postoperative complications occurred in 15 patients compared with 18 patients in the thoracotomy group (P = .671).
Distribution of Surgical Procedures for Video-Assisted Thoracoscopic Surgery and Thoracotomy Patients for Bronchiectasis
VATS, video-assisted thoracoscopic surgery.
Perioperative Data for Video-Assisted Thoracoscopic Surgery and Thoracotomy Patients for Bronchiectasis
VATS, video-assisted thoracoscopic surgery.
Postoperative Complications of Video-Assisted Thoracoscopic Surgery and Thoracotomy Patients for Bronchiectasis
VATS, video-assisted thoracoscopic surgery.
All patients underwent follow-up for a mean duration of 33.6 months (range 5–65 months). In the VATS group, symptoms disappeared after surgery in 35 patients, symptoms improved after surgery in 11 patients, and symptoms did not improve or worsened in 3 patients. In the thoracotomy group, symptoms disappeared in 38 patients, symptoms improved in 8 patients, and symptoms did not improve or worsened in 4 patients (Table 5). No significant difference was observed between the two groups (P = .694) (Fig. 1).
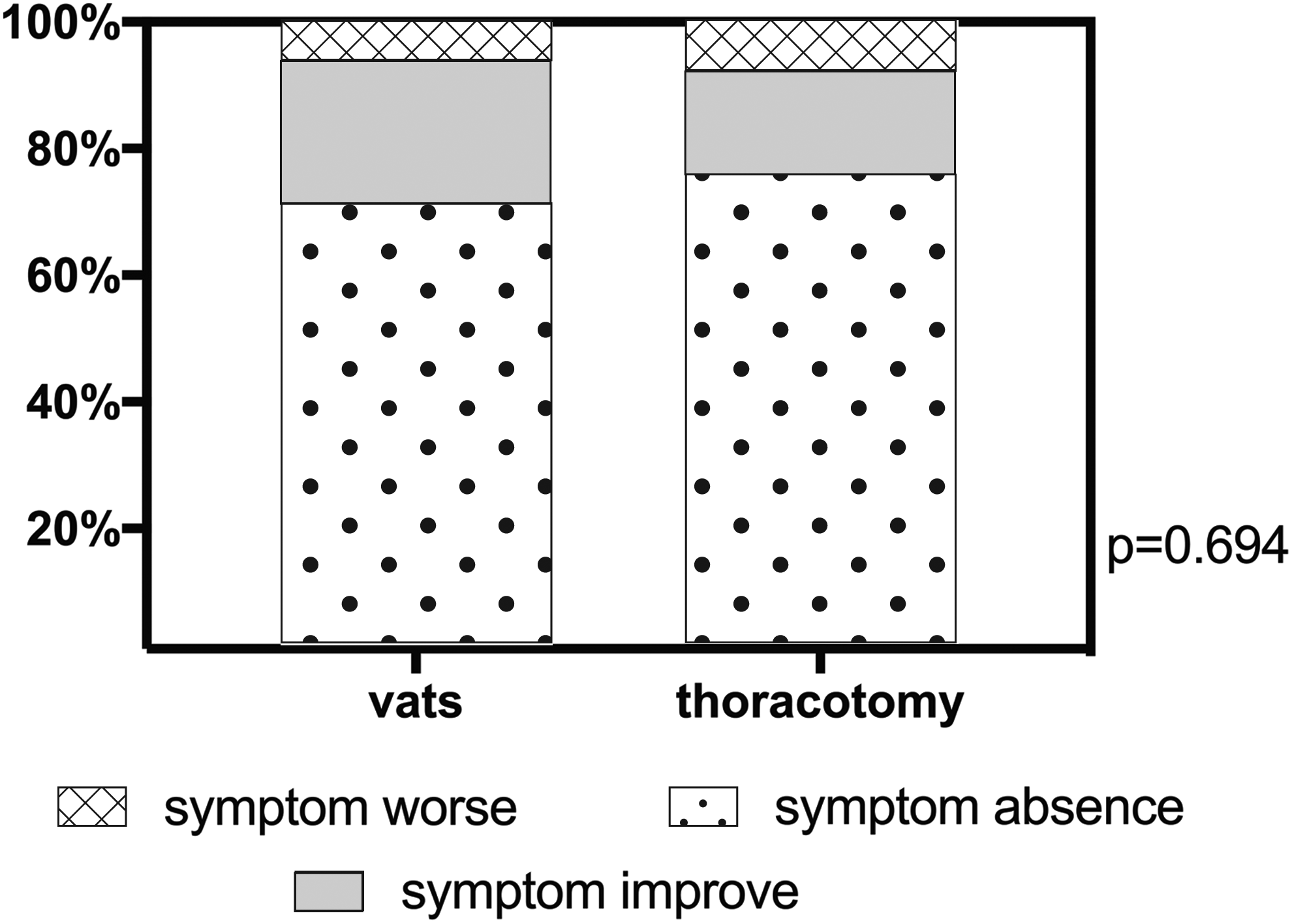
Symptom changes after surgery.
Follow-Up Symptoms of the Patients
VATS, video-assisted thoracoscopic surgery.
Discussion
Bronchiectasis is a chronic infection of the bronchi and bronchioles that leads to abnormal and permanent dilation of the proximal bronchi. The prevalence of bronchiectasis was 1106 cases per 100,000 people from 2000 to 2007 in the United States, with an average annual percentage increase of 8.7%. 6 This increase may be due to a true increase in the condition or increased recognition of previously undiagnosed cases. 6 An urban population-based cross-sectional survey of bronchiectasis conducted in China between 2002 and 2004 showed that the overall prevalence of bronchiectasis in China was 1.2%, 7 although the reported percentage included only those individuals diagnosed with bronchiectasis. In fact, the number of patients with undiagnosed bronchiectasis remains largely unknown, and the actual prevalence of bronchiectasis in China is expected to be far greater than 1.2%. 8
The objectives of bronchiectasis treatment are to prevent exacerbations, reduce symptoms, improve quality of life, and halt disease progression.9–14 Surgical treatment is usually considered an appropriate therapy for bronchiectasis among patients with recurrent exacerbations or refractory disease. Before modern antibiotics were available, surgery played an important role in the treatment of bronchiectasis. Currently, surgical treatment of bronchiectasis remains controversial. Surgery is usually reserved for localized disease that is refractory to medical management in patients with life-threatening comorbidities, such as recurrent or massive hemoptysis. Owing to the absence of randomized control trials, no unbiased evidence exists of the effect of surgery for bronchiectasis. Conversely, there is no evidence that surgery is not beneficial. 15 A meta-analysis that included 38 observational studies with 5541 patients examined the efficacy and safety of different surgical interventions for adult patients with bronchiectasis and focused on postoperative mortality, morbidity, and symptom improvement. 16 In this meta-analysis, among the adult population, the rate of absence of symptoms was 71.5%, the rate of improvement of symptoms was 20.2% (95% CI 17.3–23.1), and only 9.1% of patients showed no improvement or worse conditions. 16
The surgical intervention for treatment of bronchiectasis was notable; for most patients, lung resection diminished or eliminated symptoms. 16 In our study, the total improvement rate was 93.6%, and no significant difference was observed between the two groups, which is similar to other series.17–19 Vallilo et al. demonstrated that patients with bronchiectasis gained a significant improvement in their quality of life and exercise capacity after surgery. 17
If patients do not have unilateral localized bronchiectasis, the improvement may be limited. Selected patients with diffuse bronchiectasis can also undergo incomplete resections. This surgery can reduce the hospital stay and antibiotic use, resulting in improved quality of life and, more importantly, a delay in the progression of the disease by preventing contamination of the adjacent lung.20–24 No perioperative deaths occurred in this cohort. The total morbidity rate was 17.2%, which was similar to the pooled outcome of all complications (16.7%). 16 The most common complication in this cohort was PAL, but the 7 patients with air leak recovered without reoperation. Surgery for bronchiectasis in this cohort was associated with acceptable morbidity rates and favorable symptom improvements.
The use of VATS for lung cancer has become a routine procedure in recent years, with promising outcomes. 25 The use of VATS for infection or inflammatory conditions, but not lung cancer, is controversial. 26 In most developed countries, <5% of VATS procedures are performed for infectious conditions. 26 Although open thoracotomy continues to be the preferred choice for infectious conditions, the advantages of VATS over thoracotomy include the excellent exposure of all parts of the chest cavity, shorter hospital stay, and fewer complications due to decreased chest wall injury during the treatment of infectious lung diseases. 26 Zhang et al. reported that VATS resulted in a shorter hospital stay and fewer complications than thoracotomy for bronchiectasis. 18 In our study, bronchiectasis treatment through VATS resulted in a longer operative time. This result may be due to the technical challenges of the lysis of dense adhesions, management of hypertrophied bronchial vessels, and dissection of hypertrophied and calcified lymph nodes under a thoracoscope. Similar blood loss and a shorter duration of chest tube placement indicated that the use of VATS for bronchiectasis treatment is a safe and fast recovery approach.
Complications in these two groups were similar. This result may be due to the expansion of VATS indications. Zhang et al. chose patients with young age, no severe parenchymal and (or) pleural scarring, and no calcified lymph nodes near pulmonary arteries and veins shown on CT scans. These carefully selected indications may reduce the operative difficulty and ensure a better postoperative outcome. In our department, we did not strictly choose the VATS indications. Hence, no significant difference was found in the morbidity or complication rates. VATS resection allows older and more severe patients with multiple comorbidities to undergo resection. In this cohort, the age of the VATS group was notably lower than that of the thoracotomy group (49.25 ± 10.74 years versus 52.84 ± 8.66 years, P = .025). In China, patients with bronchiectasis may choose conservative therapy first, until these patients become severely ill or older.
The resection of purulent lesions through minimal access may predispose patients to contamination of the thoracic cavity and incision. In this study, no significant difference was found in postoperative empyema or wound infection. After resection, a large volume of saline solution was applied to wash the thoracic cavity and incision to prevent contamination.
In conclusion, surgical resection of bronchiectasis can be performed with acceptable localized disease morbidity. Video-assisted thoracoscopic lung resection is a safe and efficient procedure with improved recovery, especially for older patients with bronchiectasis.
Footnotes
Disclosure Statement
No competing financial interests exist.