
Abstract
Abstract
Background:
Abdominal wall defects (AWDs) include recti diastasis and midline hernias (umbilical, epigastric, and incisional). In the coexistence of such fascia defects, simultaneous repair is recommended. Conventional and hybrid techniques have been reported as an option of approach. This study aims to present the results of a total minimal invasive access to treat AWD with mesh reinforcement (subcutaneous videosurgery for abdominal wall defects [SVAWD] technique).
Patients and Methods:
The prospective observational study included patients with small/medium midline incisional hernia and/or multiple AWDs (symptomatic umbilicus and/or an epigastric hernia and/or abdominal rectus diastasis >2 cm) operated between August 2016 and February 2018. The exclusion criteria were, namely, fascia defects >10 cm, complex hernias, excess of skin and/or subcutaneous abdominal fatty tissue, and body mass index >35 kg/m2.
Results:
Twenty-one patients were treated by SVAWD technique, with a median follow-up of 14 (range 6–22) months. The mean size of all fascia defects was 7.46 cm (range 4.5–10.5). Surgical site occurrence was identified in three (14.3%) patients and surgical site occurrence requiring procedural intervention in two (9.5%). Diabetes mellitus was the only predictor factor for higher intraoperative bleeding (R2 = 0.63, P = .025). Fibrin sealant (used for mesh fixation) and transverse abdominis plane (TAP) block with ropivacaine 0.2% were associated with less oral analgesics intake (P < .001 and P < .001, respectively) and fewer complications (P = .005 and P = .034, respectively).
Conclusion:
Despite the low number of patients operated, the subcutaneous approach presented has proven to be safe, feasible, and effective, as no major complications and relapse occurred. Still, fibrin sealant and TAP block were associated with fewer complications and less oral analgesics intake.
Introduction
Abdominal wall defects (AWDs) include rectus diastasis, middle line hernias (umbilical and epigastric), and incisional hernia. They are very common pathologies and may occur singly or simultaneously. Abdominal recti diastasis (ARD) is a condition that weakens the linea alba resulting in abdominal protrusion. Its incidence in the general population is unknown. It occurs more frequently in elevated intra-abdominal pressure.
It mainly affects mid-/old-age obese people or after multiple pregnancies or women who carried a large fetus. 1
Usually, ARD causes no symptoms and the distance between rectal muscles <2 cm requires no intervention. 2 Apart from esthetics deterioration, some patients may experience abdominal discomfort or even pain related to abdominal movements. In addition, the association with midline hernias such as umbilicus, epigastric, and incisional hernia occurs frequently. 3 The etiology of middle hernias is multifactorial and may include collagen deficiency, smoking, and handyman workers. Incisional hernias may occur in 15%–20% after laparotomy and are mainly caused by wound infection, malnutrition, and technical errors during abdominal wall closure. 4 It has been reported that patients with umbilicus and epigastric hernia are more likely to have a relapse if the ARD is not treated at the same time. 5 Therefore, in the coexistence of such fascia defects, simultaneous repair of all AWDs is recommended. 6
Nevertheless, until now there is no global consensus in the medical literature regarding indications and the best surgical approach to treat the fascia defects. Most data published correspond to open procedures (85%). 7 Conventional abdominoplasty with plication of the superficial aponeurosis of recti muscle with or without excess skin removal is the most common method used. 8
Another great debate concerns the durability of ARD plication associated or not to midline hernias. Probably small/single defects and a short distance between both rectus aponeurosis will not require reinforcement with prothesis and are unlikely to relapse. In contrast, multiple fascia defects, severe musculoaponeurotic laxity, and diastasis >5 cm will certainly need the use of reinforced prothesis. Al-Qattan reported 100% recurrence after longitudinal rectus muscle plication without mesh in severe musculoaponeurotic laxity after 1 year of follow-up. 9
Thus, hereunder we present the subcutaneous videosurgery for abdominal wall defects (SVAWD) technique, a total minimal invasive access to repair midline and incisional hernias as well as rectus diastasis with mesh reinforcement, in addition to mid-term outcomes.
Patients and Methods
We prospectively analyzed patients submitted to SVAWD technique from 2016 to February 2018. The indication of this approach were small/medium midline incisional hernia and multiple midline AWDs (umbilicus and/or epigastric hernia and/or abdominal rectus diastasis >2 cm). Fascia defects >10 cm, complex hernias, loss of abdominal domain, an excess of skin and/or subcutaneous abdominal fatty tissue, and body mass index (BMI) >35 kg/m 2 were treated by a different approach.
Patient demographics analyzed included age, gender, BMI, and main comorbidities. Perioperative data included ASA classification, type and size of fascia defect, type and size of mesh used, method for mesh fixation, operative time, and blood loss. The use of transverse abdominis plane (TAP) block with ropivacaine 0.2% was also evaluated.
Surgical site occurrence (SSO) and surgical site occurrence requiring procedural intervention (SSOPI) were analyzed. Complications were graded according to Clavien–Dindo's classification. 10 The length of hospital stay (LOS), the subcutaneous drain period, and length of oral analgesic intake (days) were also evaluated. Dipyrone was the first-line drug therapy and piroxicam was used as salvage analgesia. Postoperative follow-up evaluation included a physical examination at 2 weeks, 1 month, 3 months, 6 months, 1 year, and then annually.
This study was approved by the hospital ethical committee and registered in “Plataforma Brasil” (CAAE: 97379418.2.0000.5374) that collects all research projects that involve human beings in the country. Informed consent was obtained from all patients.
Surgical technique
After administering general anesthesia and antimicrobial prophylaxis with 1 g of cefazolin, the patient is placed in a modified lithotomy position with the legs apart. The surgeon stands between the patient's legs, the first assistant (camera operator) on the patient's left and second assistant on the right side. The pneumo-subcutaneous is established with a Veress needle very carefully, to avoid entering the abdominal cavity or perforating the rectus muscle aponeurosis. Once a small space between the rectus aponeurosis and the subcutaneous fat is made, a 10 mm trocar is placed for the camera and a blunt dissection is performed. Subsequently, two 5 mm ports are placed according to Figure 1. The pressure is maintained at 8–10 mmHg.

Trocar positions for subcutaneous dissection (mm).
The subcutaneous cellular tissue is dissected with the monopolar hook until the anterior rectus sheath is liberated (Fig. 2). This dissection can also be performed with the introduction of a 10 mm trocar with a balloon. The same device is used in laparoscopic totally extraperitoneal inguinal hernia repair. The extension of dissection is made avascularly toward the xiphoid appendix and to the bilateral subcostal space. The umbilical scar is released from the aponeurosis and the AWD may be fixed. Epigastric, incisional, and umbilical hernia defects are closed with running sutures using 0V-Loc 180 device™ (Medtronic) as shown in Figure 3. Diastasis recti is also treated with plication of the superficial aponeurosis of both recti muscles. To facilitate closing the defects, CO2 pressure may be diminished to 8 mmHg. In case of inadvertent entry of the abdominal cavity with pneumoperitoneum, an extra 5 mm trocar may be inserted to allow the gas to escape, whereas the suture is performed without the tension of the abdominal wall musculature. In some cases of incisional hernias with adherence of viscera in the posterior abdominal wall, the release of these adhesions by laparoscopy may be performed before the dissection of the subcutaneous space is accomplished. In addition, other surgical interventions such as cholecystectomy and inguinal hernia repair may be performed during this procedure. After closing the defects, a large polypropylene mesh is placed to reinforce the abdominal wall strength (Fig. 4). It may be pinned with biological glue or absorbable tacks. The umbilicus is reinserted at the aponeurosis through a small transumbilical incision. It is pivotal to place a closed system suction drain to avoid seroma and infection. The drain is removed once the output amount is <30 mL per day for at least two consecutive days.

Area of subcutaneous dissection under direct endoscopic view, without entering the abdominal cavity.
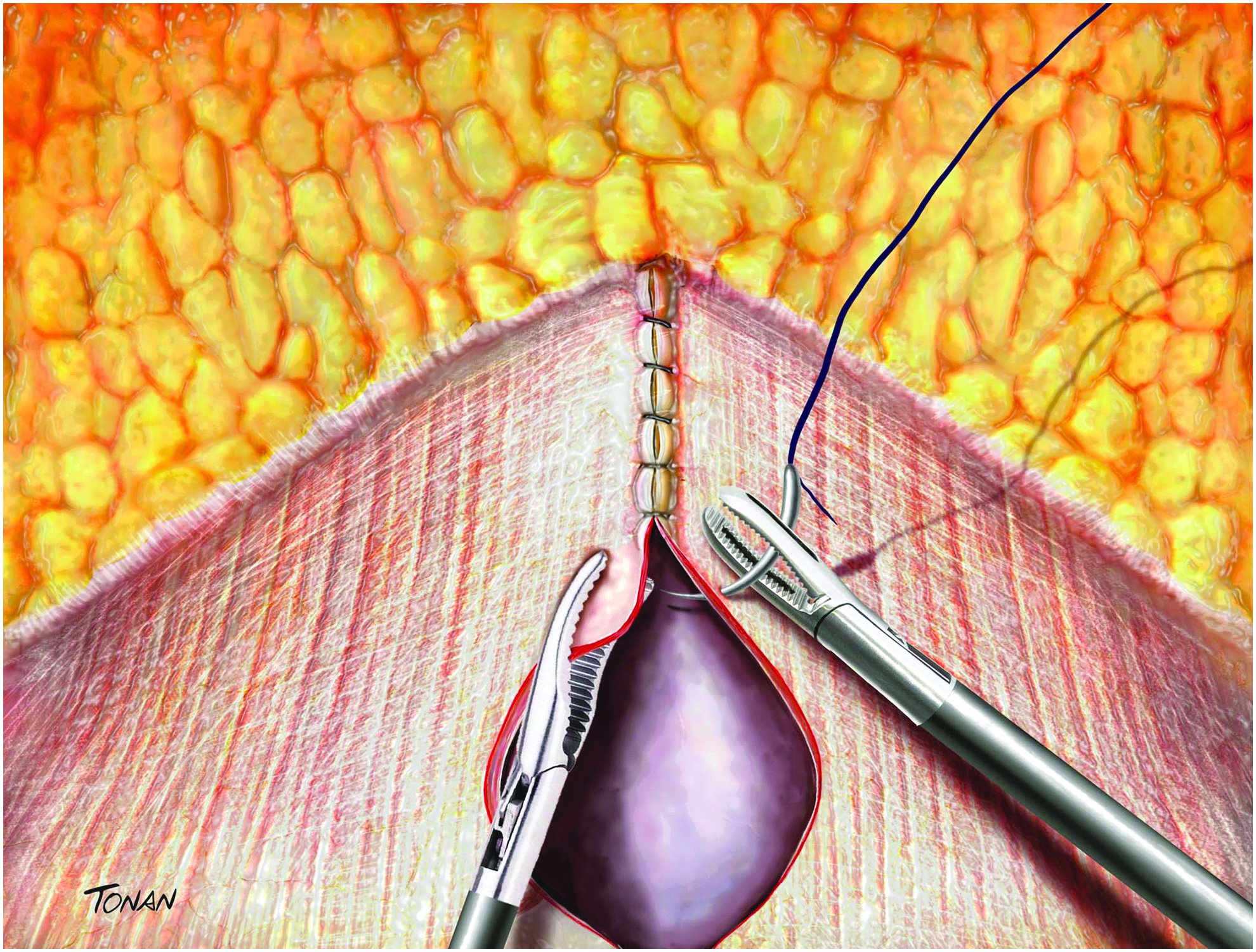
Area of subcutaneous dissection under direct endoscopic view, without entering the abdominal cavity.
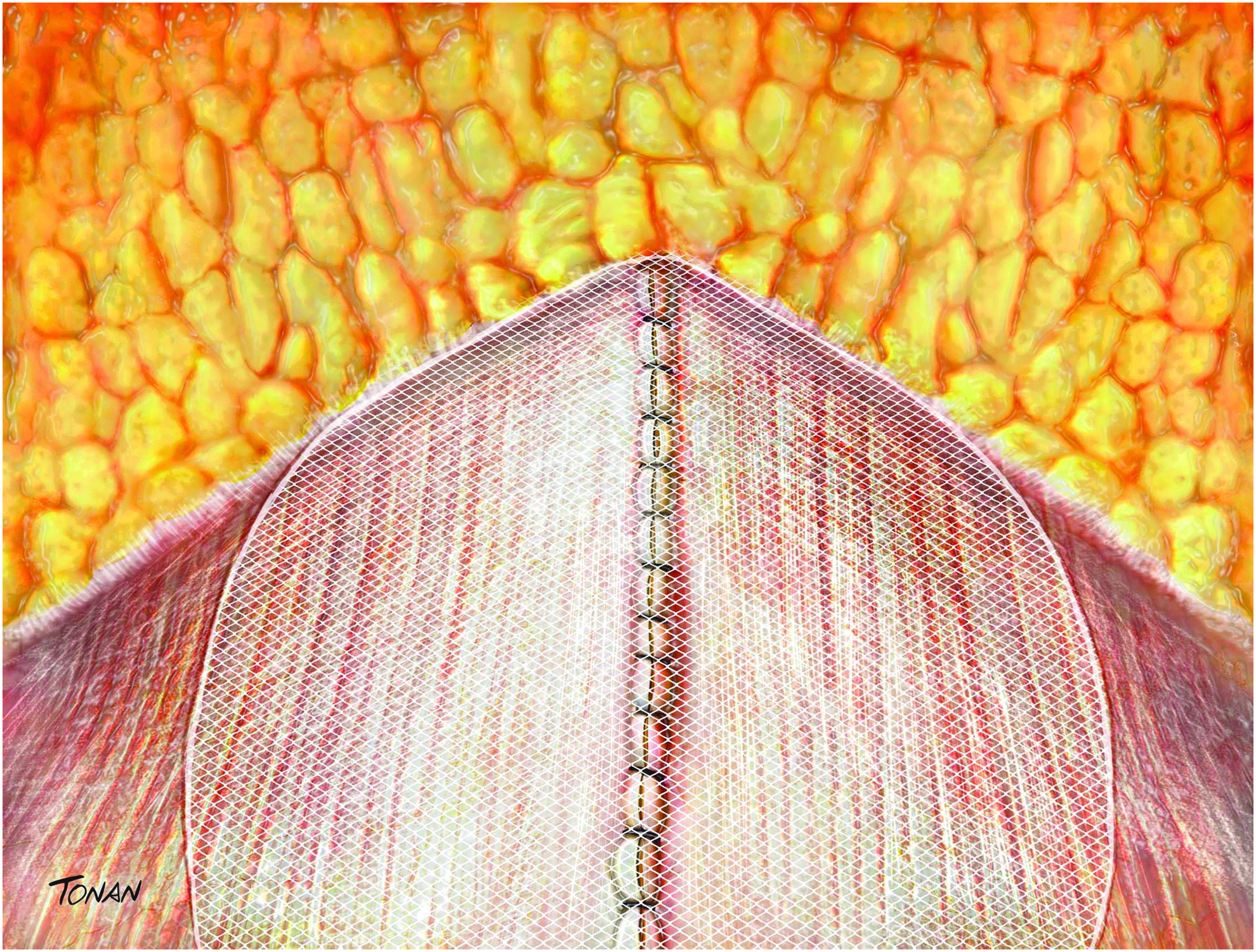
Endoscopic view and onlay polypropylene mesh placement.
Statistical analysis
The data were organized and encoded in Microsoft Excel Office 2016®. Statistical analysis was performed using the software R 3.4.1 (R Core Team, 2017). Absolute quantities, central tendency measurements (mean and median), and distribution (percentage) were used for the descriptive analysis. To evaluate the association between operative results (for instance: analgesic days, length of hospitalization, Clavien–Dindo's classification for surgical complications, operative time, intraoperative bleeding and time of subcutaneous drainage) and local anesthesia (TAP Block; yes/no) the t-test, Wilcoxon-Mann-Whitney and Fisher's Exact Test were applied. To analyze the association between operative results and type of mesh fixation (Clips, Histoacryl™, and Tisseel™), the ANOVA one-way test with Tukey post-test and Kruskal–Wallis test were applied. The tests that obtained a descriptive level of <5% (P < .05) were considered significant.
Results
A total of 21 patients were treated with SVAWD with synthetic mesh reinforcement. Patient demographics and hernia characteristics are represented in Table 1. The mean age of the total population was 47.5 years (range 29–62) with a male preponderance (57.2% versus 42.8%). More than half patients (57.1%) were overweight or obese, with a mean BMI of 26.3 kg/m 2 . Seven (33.3%) patients had associated comorbidities such as systemic arterial hypertension, diabetes mellitus (DM), or dyslipidemia. Four (19%) patients had one fascia defect (incisional hernia), eight (38%) patients had two defects (umbilicus or epigastric hernia and rectus diastasis), and nine (42.8%) patients had three defects (umbilicus and epigastric hernia and rectus diastasis). Two (9.5%) patients were simultaneously treated for inguinal hernia repair and one for cholelithiasis. None of the patients had previous hernia repair.
Patient Demographics and Fascia Defects Characteristics
Values are listed as amean (range) or number (percentage).
There are patients with more than one fascia defect.
BMI, body mass index.
Perioperative and postoperative data
A midweight macroporous polypropylene mesh was used in all incisional hernia cases. In all other defects, a lightweight mesh was placed. Operative data and patient outcomes are shown in Table 2. Most of the meshes were fixated with Tisseel (66.6%—fibrin sealant). Its use was associated with less oral analgesics intake and fewer complications (P < .001 and P = .005, respectively). TAP block was used in 13 (61.9%) patients. It was also related to less oral analgesics intake and fewer complications (P < .001 and P = .034, respectively) (Table 3).
Operative Data and Patients' Outcomes
Values are listed as amean (range), bmedian, or number (percentage). Histoacryl: n-butyl-2-cyanoacrylate; Tisseel (fibrin sealant).
TAP, transverse abdominis plane.
Association Between Transverse Abdominis Plane Block, Mesh Fixation, and Operative Results
Histoacryl: n-butyl-2-cyanoacrylate; Tisseel (fibrin sealant).
ANOVA one-way test, bKruskal–Wallis rank sum test, cANOVA one-way with Tukey post-test P = .001.
Two sample t-test; ##Wilcoxon–Mann–Whitney test; ###Fisher's exact test.
Values shown in bold denote (P<.05) is considered significant.
SD, standard deviation; TAP, transverse abdominis plane.
Table 4 represents the linear regression model. DM was the only predictor factor for higher intraoperative bleeding (R 2 = 0.63, P = .025). SSO was identified in three (14.3%) patients and SSOPI in two (9.5%). One (4.7%) patient had a minor umbilical infection and was successfully treated with antibiotics. Another patient had a seroma and required evacuative puncture. In one patient (4.7%) the mesh needed to be removed after 7 months of the operation due to infection. The median follow-up of the study population was 14 months (range 6–22). No recurrence occurred during this period.
Linear Regression Model on Intraoperative Bleeding
R 2 : variable proportion explained by the predictor.
Values shown in bold denote (P<.05) is considered significant.
ASA, American Society of Anesthesiologists risk classification.
Discussion
Several methods for the correction of ARD have been described. Most of them include plication of the rectus sheaths (anterior, posterior, or both). When it is associated with midline hernias, mesh reinforcement is required. 6 Hence, large incisions are mandatory for the placement of a prosthesis that covers all the anterior AWD. It may be performed by conventional surgery through a long midline incision and large lateral dissections 8 or through abdominoplasty with an arciform suprapubic incision (with or without skin removal). 11 In both situations, there is an increased risk of surgical wound infections, as well as skin scar esthetic deterioration.
Minimal invasive surgery has been developed to diminish surgical complications, and among them is wound morbidity. Thusly, laparoscopy has been described as an option to repair AWD. Laparoscopic intraperitoneal onlay mesh (IPOM) consists in the deployment of a partially absorbable tissue-separating mesh to treat ventral hernia. Indeed, this technique considerably increases costs and several problems as recurrence, seroma formation, and bulging have been described. 12 The IPOM reinforcement (IPOM-plus), which consists in plication of the defects, performed intracorporeally (which may be challenging through laparoscopy) or extracorporeally (with Reverdín needle) has been introduced to improve IPOM outcomes. 13 However, some issues remain. Sharma et al. reported recurrent rate of 4.4% in 1223 patients operated by laparoscopic for ventral and incisional hernia (IPOM and IPOM-plus). Inadvertent enterotomies occurred in 2% of patients, 25% presented seroma, and 15% complained of chronic pain after 5 years of follow-up. 14 Interestingly, it does not solve the problem of recti diastasis.
To solve these problems, the subcutaneous approach allows major dissections with minimally invasive access. It avoids entering the abdominal cavity and, for this reason, organs injury, especially in small/mid incisional hernias. It was first reported in 1998 by Champault et al. The technique described at that time was for purely cosmetic reasons. The dissection was very limited, without CO2 gas, and used only as an accessory in conventional abdominoplasty. The indications included the only plication of small ARD and primary closure of umbilicus or epigastric hernias with no mesh placement. 15 Recently, hybrid procedures have been described as variations of the open technique, such as the endoscopic-assisted linea alba reconstruction plus mesh augmentation (ELAR plus), 16 mini/less open sublay repair (eMILOS), 17 and the endoscopic midline plication. 18
In 2015, Bellido Luque et al. published good results in a prospective cohort study using a hybrid subcutaneous approach with CO2 gas to treat ARD and midline hernias. The mean hernia size was 3.4 cm and the mean ARD size was 3.05 cm. As size defects were in general small, limited subcutaneous dissection was carried out and not all patients received mesh reinforcement. Furthermore, the prothesis used in that study was Ventralex™ Hernia Patch (Bard), only applied at the hernia defect, leaving the rest of the plication unprotected, with a higher chance of ARD recurrence. Meanwhile, seroma was the main complication (23%), probably related to the early removal of the drain (average 4.2 days, range 2–6). 18 In our study, only one patient (4.7%) had a seroma. The subcutaneous drain was removed on the ninth postoperative day. For this reason, we advocate longer period for its removal (median of 15 days, range 9–19). 18
Köckerling et al. described a hybrid (open and endoscopic) technique used for reconstruction of the linea alba with mesh placement for umbilicus/epigastric hernias and concomitant ARD with good outcomes. The skin incision was done on the left side, encircling all the umbilicus and extending 3 cm upward. The dissection was performed above the umbilicus and consequently, infraumbilical ARD or infraumbilical hernias are not eligible for treatment by this approach. 16 Still, the size of fascia defects was not informed and neither were mid-/long-term outcomes, as only 30 days of follow-up was reported.
The technique presented in this study has some peculiarities. To the best of our knowledge, this is the first prospective study that analyzed the feasibility of total minimally invasive subcutaneous approach treating incisional hernias and other AWDs. Multiple fascia defects, including infraumbilical rectus diastasis, were treated at once by this approach as the dissection area was wide and large prothesis that covered up all the anterior abdominal wall was placed. In fact, most of the patients treated with SVAWD technique in this study had multiple fascia defects. The mean size of all fascia defects was 7.46 cm (range 4.5–10.5), demonstrating the feasibility to place large mesh by this technique. Another relevant aspect of the technique presented is the low cost for its achievement, as no special material is required (separating tissue mesh or energy device).
Three different types of mesh fixation were used: absorbable tacks, Histoacryl, and Tisseel. In the first group of cases, it was absorbable tacks that were used, and we progressively moved to fibrin sealant. It is expected that using tacks could lead to more postoperative pain. Fortelny et al. published a systematic review of the use of fibrin sealant in hernia repair. It was associated with less morbidity, less chronic pain, less bleeding, shorter operative time, and LOS when compared with a tissue penetrating fixation method. Yet, it did not increase the risk of recurrence. 19 In addition, Köhler et al. demonstrated a protective effect against seroma formation and a lower rate of wound complications with this type of mesh fixation in ventral hernia repair. 20 Indeed, this was observed in our data, as patients treated with fibrin sealant had fewer oral analgesic intake days (P < .001) and fewer complications (P = .005). Histoacryl was used in two (9.5%) patients. One of them experienced an intense inflammatory response and mesh infection. Regardless of the conservative management with antibiotics, analgesics, and hyperbaric oxygen therapy, the mesh was explanted after 7 months and the patient remained without recurrence (14 months of follow-up).
Some studies have demonstrated that DM is an important risk factor for complications. For instance, Huntington et al. reported that in 15,589 patients undergoing laparoscopic ventral hernia repair, diabetic patients had higher rates of major complications (12.2% versus 7.1%, P < .0001). 21 Although linear regression found that DM patients could bleed ∼57 mL more than nondiabetic individuals (P = .025), our results have shown minimal intraoperative bleeding and no major complications.
Another important factor is the use of TAP block as an enhancement in postoperative analgesia. It has been associated with less postoperative pain in minimally invasive hernia repair. 22 Furthermore, a recent study has shown that TAP block under direct visualization provides superior analgesia in the immediate postoperative period than ultrasound-guided TAP block after ventral hernia repair with posterior component separation. 23 As expected in our analysis, patients with TAP block had fewer oral analgesic intake days (P < .001). Interestingly, there was also an association with fewer complications, including wound infection (P < .034). This “protector effect” of TAP block in hernia surgery was also observed in a meta-analysis published by Gao et al. There was a significant reduction of general postoperative complications in patients who had received a TAP block compared with control or placebo (313 patients, P = .03). 24
Table 5 shows the comparison between the main subcutaneous approach techniques recently published. The most important variable for patients is the cosmetic result and functional recovery of the abdominal wall. The SVAWD technique, as well as the other hybrid procedures, may accomplish it. In contrast, one of the primary medical goals in AWD surgery is to avoid recurrence. Whereas these innovating techniques have been described recently, with limited data, they appear to be a promising alternative for AWD with very low recurrence.
Comparison Between the Main Subcutaneous Approach Techniques Recently Published
Mean (range).
Median.
ARD, abdominal recti diastasis; BMI, body mass index; Epig H, epigastric hernia; LOS, length of hospital stay; NA, data not available; SVAWD, subcutaneous videosurgery for abdominal wall defects; UH, umbilical hernia.
Conclusions
Despite the low number of patients operated, the subcutaneous approach presented has proven to be very safe and feasible, as no major complications occurred. It has shown to be comparable in efficiency to hybrid techniques described previously, with total minimally invasive access. It allows the repair of most abdominal wall fascia defects, including incisional hernias with mesh reinforcement. In addition, recurrence has not been observed during follow-up. Still, fibrin sealant used for mesh fixation and TAP block used for postoperative analgesia was associated with fewer complications and less oral analgesics intake.
Authors' Contributions
L.C.B.: conception and design, and/or acquisition of data, and/or analysis and interpretation of data; L.C.B. and M.Y.F.: drafting the article or revising it critically for important intellectual content; B.Z.: final approval of the version to be submitted and any revised version to be published.
Footnotes
Disclosure Statement
No competing financial interests exist.