
Abstract
Abstract
Background:
Solid pseudopapillary neoplasms (SPNs) of the pancreas are rare pancreatic tumors. This study summarizes the clinicopathological characteristics and treatment outcomes of SPN patients through a 10-year single-center case series.
Materials and Methods:
Medical records of patients diagnosed with SPNs and who underwent surgery between August 2007 and July 2017 at Qilu Hospital, Shandong University, were retrospectively analyzed.
Results:
This study included 91 patients: 13 males/78 females, mean age 28.8 ± 11.5 years. Among the cases, 38.5% were incidentally confirmed without specific symptoms, while the others displayed various abdominal symptoms. All patients had single pancreatic lesions, and 1 patient presented with liver metastasis. Abdominal enhanced computed tomography, magnetic resonance imaging, and endoscopic ultrasound were the diagnostic imaging techniques used to identify SPNs. All patients had successful surgical removal of their tumors; 28 patients underwent laparoscopy. During the 2–121-month follow-up period, 1 patient died of lung metastasis and multiple organ failure at 35 months postoperatively, but no other tumor recurrence or metastasis was found.
Conclusions:
SPN usually occurs in the young female population and presents with various clinical characteristics. Mixed solid–cystic masses with calcification or hemorrhage are typical morphological tumor features. Minimally invasive organ-/function-preserving operations are advocated for benign cases, while aggressive radical resection should be performed in patients with local invasion or distant metastasis.
Introduction
Due to rapid development of abdominal imaging technology and its ubiquitous use in clinical practice, pancreatic cystic neoplasms (PCNs) have been increasingly detected in recent years. PCNs include a variety of pathological subtypes that show markedly different malignant potential and biological behaviors.1,2 Solid pseudopapillary neoplasm (SPN) of the pancreas accounts for only 2%–5% of all PCNs; 1%–2% of exocrine pancreatic neoplastic lesions. SPN is believed to be a rare disease with low malignant potential.1,3 It was first described by Frantz in 1959 4 and designated as solid pseudopapillary neoplasm by the World Health Organization in 1996. 5
SPN cases are being diagnosed much more frequently than before; the current incidence rate is reported to be 7-fold that of 2000. 6 Based on previous studies, SPN has a malignancy rate of 8%–20%.1,7–9 Hence, early detection and surgical intervention provide the best treatment strategy for this disease. However, the variable clinicopathological and radiological features of SPNs make these procedures challenging to surgeons, resulting in pitfalls in diagnosis and surgical treatment. In this retrospective study, we summarized and presented clinicopathological characteristics of 91 SPN patients from our center over a 10-year period. We also investigated outcomes of surgical treatment to identify the best strategies for diagnosing and treating this rare disease.
Materials and Methods
Patients
The clinicopathological data of patients who were diagnosed with SPNs between August 2007 and July 2017 at Qilu Hospital, Shandong University, in China were retrospectively collected and analyzed. We included 91 consecutive patients who underwent surgical resection, were confirmed to have SPNs by pathological examinations, and had integrated clinicopathological data and a follow-up time exceeding 2 months. Patients who suffered from other malignances or underwent surgical biopsy rather than resection were excluded.
To investigate differences in the incidence rate and management strategies of SPNs, we divided the patients into two groups: patients treated from August 2007 to July 2012 and patients treated from August 2012 to July 2017. We also categorized the patients according to the surgical technique used: open surgery (OP) or laparoscopic surgery (LAP). Pancreatic fistula was defined according to the new International Study Group of Pancreatic Fistula classification. 10 This study was approved by the Ethics Committee of our hospital.
Observation index
The observation index included demographic information, clinical manifestation, radiological examination, surgical procedures, postoperative complications, pathological results (including surgical margin, tumor size, hematoxylin and eosin staining, and immunohistochemical [IHC] staining), and follow-up information.
Preoperative imaging diagnosis
All patients underwent enhanced computed tomography (CT) scanning, and 25 patients also underwent a magnetic resonance imaging (MRI) examination. Endoscopic ultrasound (EUS) evaluation was performed on 11 patients.
Pathological data
Histological slides from each tumor were reviewed by experienced pathologists to confirm SPN diagnoses. Histological features of malignant pathology, including extrapancreatic invasion, lymph node or distant metastasis, pancreatic parenchymal invasion, lymphovascular invasion, and perineural invasion, were recorded. IHC staining results were also reviewed and scored.
Follow-up
The last follow-up date was the end of September 2017, at which time all data were acquired from hospital records and were supplemented with information collected from telephone interviews or clinic visits with patients. We collected survival, tumor recurrence, and metastasis data points.
Statistical analyses
All statistical analyses were performed using SPSS, version 20.0 (IBM, Armonk, NY). All quantitative data are expressed as mean ± standard deviation. Independent sample t-test and ANOVA were used to compare quantitative variables. Chi-square test and Fisher's exact test were used to compare categorical variables. A value of P < .05 was considered statistically significant.
Results
General and clinical characteristics
Demographic information, clinical characteristics, and comparison of clinical features between the first 5 years and the last 5 years are shown in Tables 1 and 2. A total of 91 patients, including 13 males and 78 females, were included in this study. The mean age was 28.8 ± 11.5 years (range: 9–65 years). Twenty-nine patients were diagnosed in the first 5 years (August 2007–July 2012), while the remaining 62 cases were diagnosed in the last 5 years (August 2012–July 2017). Approximately 38.5% (35/91) of cases were incidental findings during routine physical examinations, whereas the rest of the patients presented with a variety of clinical symptoms, which ranged from abdominal pain or discomfort (45.1%), abdominal masses (13.2%), nausea and vomiting (11.0%), jaundice (1.1%), and constipation (1.1%). No patients presented with a history of abdominal trauma or pancreatitis (acute or chronic). Assessment of serum tumor markers found that 3 of 82 patients had elevated serum carbohydrate antigen-199 (CA-199) levels, while all other markers (including carcinoembryonic antigen) were recorded within normal limits.
Demographic Information and Clinical Characteristics of Solid Pseudopapillary Neoplasm of the Pancreas by Surgical Resection
CA, carbohydrate antigen; CEA, carcinoembryonic antigen; LAP, laparoscopic surgery; M, mean; OP, open surgery; SD, standard deviation.
Comparison of Demographic and Clinical Characteristics of Solid Pseudopapillary Neoplasm of the Pancreas Between the First 5 Years and Last 5 Years
The first 5 years were from August 2007 to July 2012, the last 5 years were from August 2012 to July 2017.
CP, central pancreatectomy; DP, distal pancreatectomy; DPPHR, duodenum-preserving pancreatic head resection; LAP, laparoscopic surgery; M, mean; OP, open surgery; PD, pancreaticoduodenectomy; SD, standard deviation.
All patients had a single pancreatic lesion, ranging from 1.5 to 30 cm in size (mean: 6.9 ± 4.0 cm). In 70.3% (64/91) of the patients, the tumor was ≥5 cm. The locations of tumors within the pancreas were as follows: head and uncinate process (35.2%, 32/91), neck (15.4%, 14/91), and body and tail (49.4%, 45/91). One patient presented with liver metastasis, and their preoperative imaging is shown in Figure 1D.
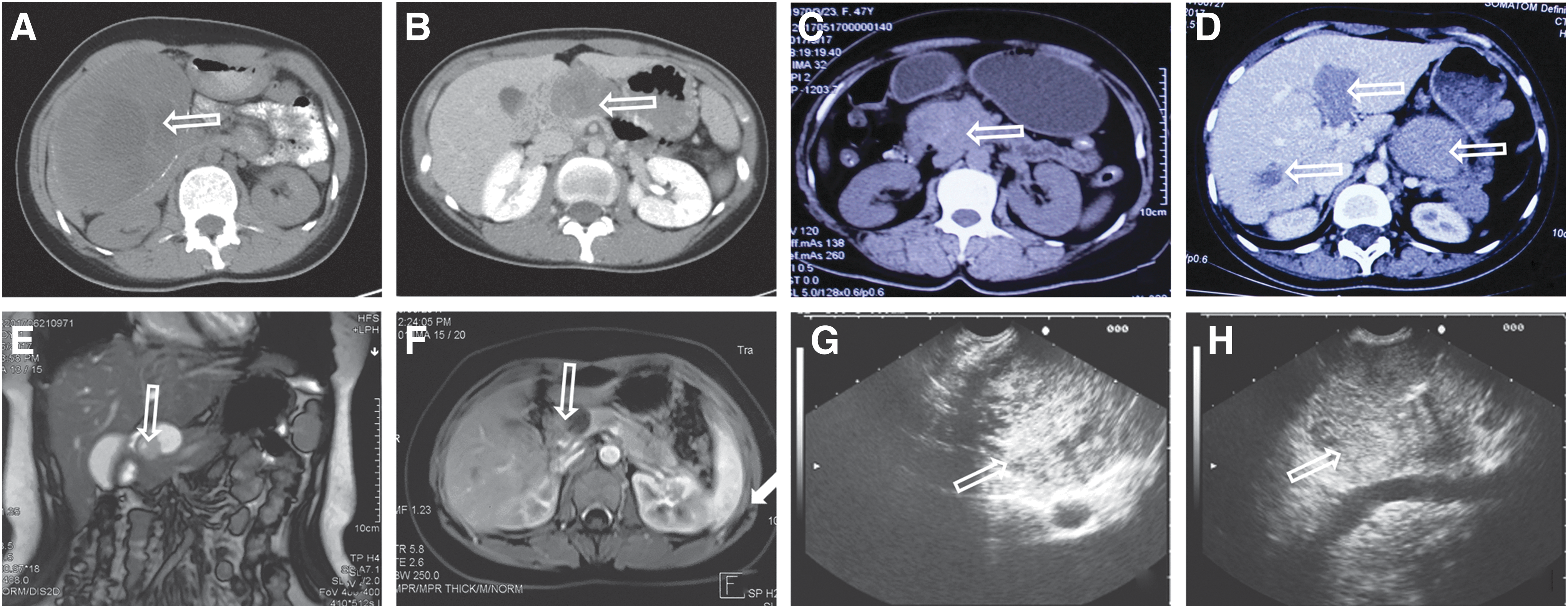
Images of different SPN patients. CT images of
Diagnostic imaging
The imaging results of some patients are shown in Figures 1 and 2. The typical imaging features were well-encapsulated heterogeneous masses with cystic and solid components; calcifications and signs of degeneration, necrosis, or hemorrhage could also be found. Typical mixed solid and cystic lesions were confirmed in 67.0% (61/91) of cases, while purely cystic lesions accounted for 4.4% (4/91), and purely solid lesions were found in 28.6% (26/91) of cases.
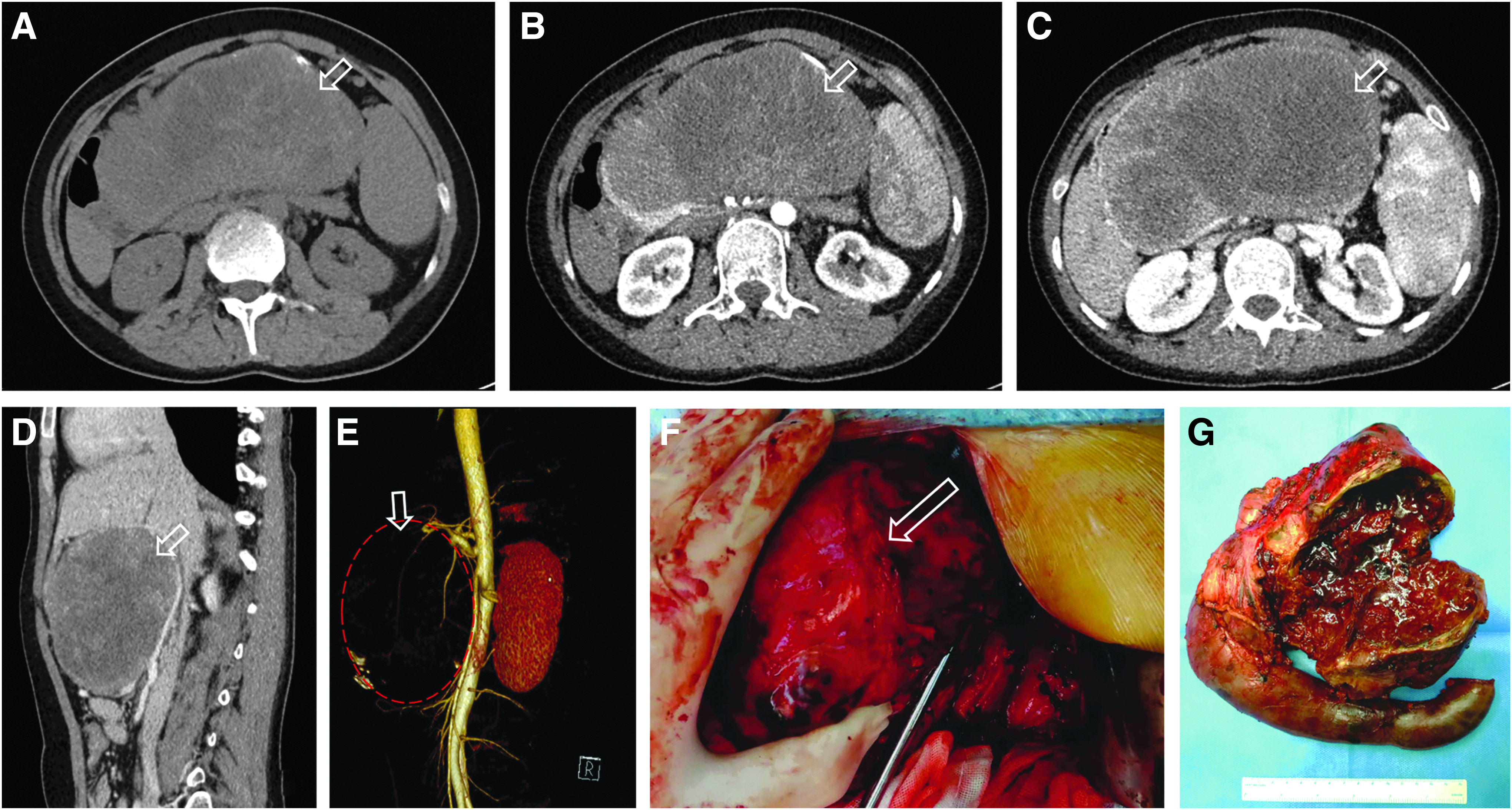
Preoperative enhanced CT images, intraoperative findings, and resected specimen of a 20-year-old female patient with a 15-cm cystic-SPN in the pancreatic head who underwent pancreatoduodenectomy. Preoperative enhanced CT images:
Surgical procedures
Surgical procedures are summarized in Tables 2 and 3, and Figure 3 shows intraoperative photographs of different surgical procedures under laparoscopy. Briefly, 69.2% (63/91) of patients underwent OP, while LAP was performed in 30.8% (28/91). Tumor enucleation was the most common surgical technique (34.0%, 31/91), followed by distal pancreatectomy with (14.3%, 13/91) or without (27.5%, 25/91) splenectomy. Pancreaticoduodenectomy (12.1%, 11/91), central pancreatectomy (9.9%, 9/91), and duodenum-preserving pancreatic head resection (2.2%, 2/91) were also used to resect some tumors. More laparoscopic surgeries were performed (25 versus 3, P = .004), and the days of postoperative hospital stay were shorter (12.5 ± 4.8 days versus 16.1 ± 6.4 days, P = .003) for patients treated over the last 5 years compared with those treated during the first 5 years (Table 2). There was no statistically significant difference in operation time and blood loss between the OP and LAP groups (Table 3). The mean operation time was 227.6 ± 96.8 minutes, and the intraoperative blood loss was 246.4 ± 494.1 mL.
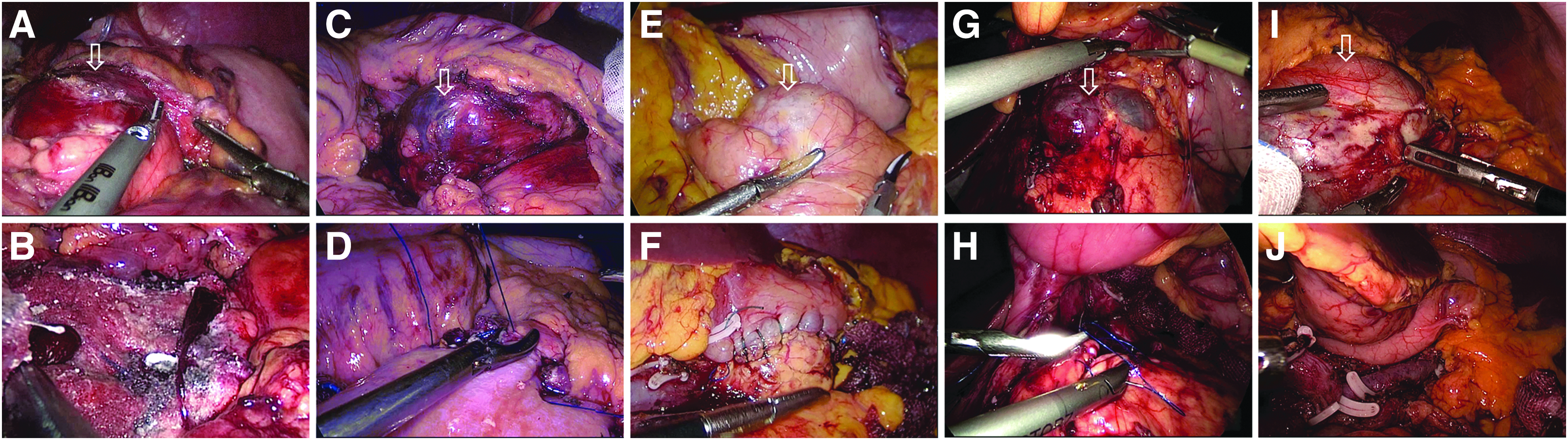
Intraoperative photographs of 5 SPN patients in laparoscopic operations.
Comparison of Procedures and Postoperative Outcomes Between Laparoscopic and Open Surgery
CP, central pancreatectomy; DP, distal pancreatectomy; DPPHR, duodenum-preserving pancreatic head resection; LAP, laparoscopic surgery; M, mean; OP, open surgery; PD, pancreaticoduodenectomy; SD, standard deviation.
Postoperative complications
There were no operative mortalities in these patients. Morbidity for all patients was 28.6% (26/91). Causes of morbidity included pancreatic fistula (Grade B, 23.1%, 21/91), abdominal bleeding (2.2%, 2/91), pneumonia (1.1%, 1/91), delayed gastric emptying (1.1%, 1/91), and incomplete obstruction (1.1%, 1/91) (Table 3). No differences were noted between the LAP and OP groups regarding postoperative complications, but the length of postoperative hospital stay was shorter in the LAP group (11.6 ± 5.0 days versus 14.5 ± 5.7 days, P = .021).
Pathological and IHC assessment
All histological slides were reviewed and malignant features were found in 8.8% (8/91) patients, including pancreatic parenchymal invasion (3.3%, 3/91), liver metastasis (1.1%, 1/91), splenic capsule invasion (1.1%, 1/91), duodenal invasion (1.1%, 1/91), peritoneal implantation of the vesicouterine pouch (1.1%, 1/91), and intravascular cancer emboli (1.1%, 1/91) (Table 1). As summarized in Table 4, IHC assessment was performed to confirm SPN diagnoses. The markers with the highest rates of positive staining were vimentin (97.1%, 34/35), followed by β-catenin (96.5%, 55/57), cluster of differentiation 10 (CD10; 93.9%, 62/66), alpha-1-antitrypsin (AAT; 93.7%, 45/48), progesterone receptor (PR; 93.3%, 56/60), and synaptophysin (Syn; 70.0%, 42/60). Pathological pictures are shown in Figure 4.
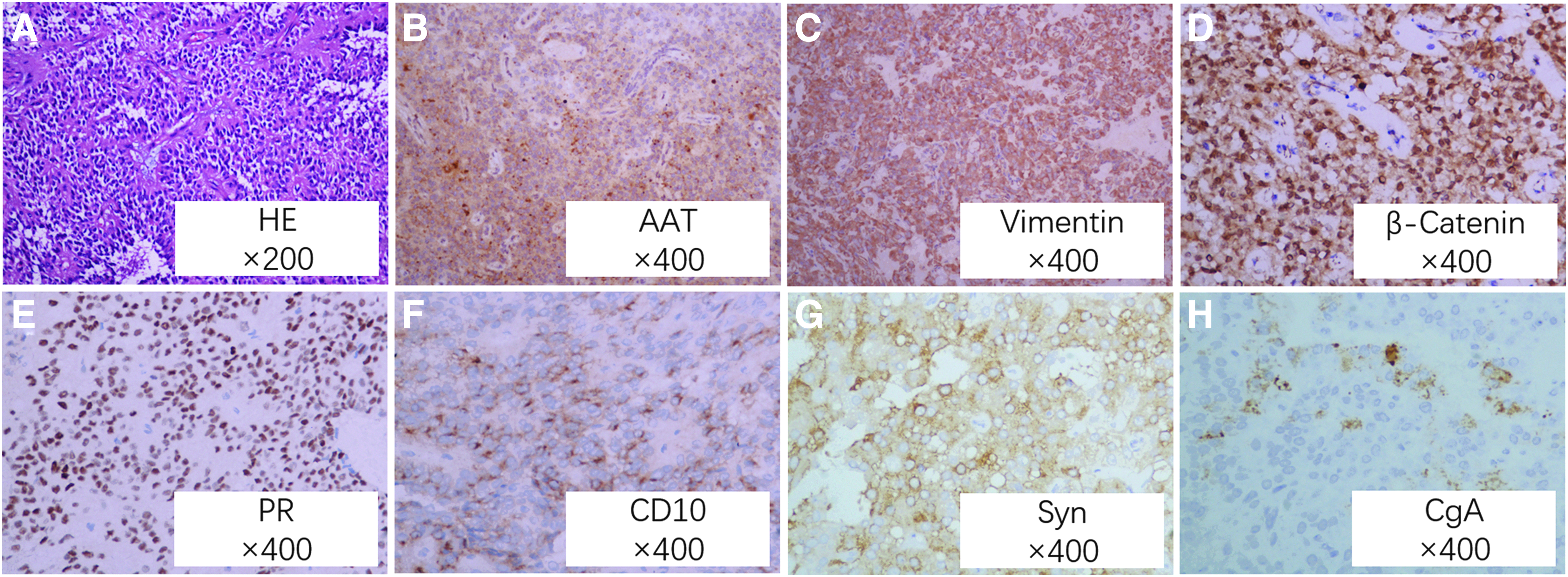
Hematoxylin–eosin
Immunohistochemical Expression of 91 Solid Pseudopapillary Neoplasms of the Pancreas
AAT, alpha-1-antitrypsin; CD, cluster of differentiation; CgA, chromogranin A; PR, progesterone receptor; Syn, synaptophysin.
Follow-up
The median follow-up period was 38 months (range 2–121 months). Eighteen patients were lost from follow-up during this period, giving a follow-up rate of 80.2%. During the follow-up period, 1 patient died of lung metastasis and multiple organ failure at 35 months postoperatively, but no other tumor recurrences or metastases were found. The 1-, 3-, and 5-year overall survival rates were 100%, 97.9%, and 96.0%, respectively.
Discussion
SPN of the pancreas was thought to be a rare tumor; however, in recent years, it has been more frequently diagnosed because of the wide use of advanced imaging techniques and increased familiarity with these neoplasms by both surgeons and pathologists.3,11 Unique clinicopathological characteristics can help diagnose this disease. In this study, we summarized and presented a case series of 91 SPN patients who were seen over the last 10 years at one medical center in China. The results showed that SPNs predominantly occurred in young female patients and that mixed solid and cystic lesions were typical imaging findings. Although SPN patients usually present with remarkable tumor sizes and potential malignancy, long-term survival of these patients is excellent. As a result, minimally invasive and organ-preserving procedures are the best surgical approaches; however, aggressive surgery is recommended for malignant cases.
In our study, 85.7% (78/91) of all SPN patients were females and the mean age was 28.8 ± 11.5 years, which was consistent with previous studies. As to why SPNs occur more often in young female patients remains unknown. Previous work has revealed that SPNs may derive from genital ridge or ovarian anlage-related cells, which are attached to pancreatic tissues during early embryogenesis. 12 Estrogenic molecules may promote cell proliferation of SPNs. 13 These results support the strong female predominance of this disease and suggest that female sex hormones may play a pivotal role in SPN carcinogenesis. SPN should be considered a likely differential diagnosis when young female patients present with cystic pancreatic lesions.
Clinical manifestations of SPNs are often atypical; for 38.5% of patients in this study, SPN was an incidental finding during routine examinations. Among patients who experienced symptoms, the most commonly reported were abdominal pain or discomfort, abdominal masses, nausea, and vomiting. These are likely to be due to large tumors and subsequent compression of adjacent tissues. This study showed that the number of SPN patients being diagnosed has increased in recent years, while mean tumor size has decreased (8.1 ± 4.3 cm August 2007–July 2012 versus 6.3 ± 3.7 cm August 2012–July 2017, P = .044). These findings are consistent with a recent article by Lubezky et al. 14 Despite tissue compression by SPN tumors, jaundice is a rare finding in SPN patients. Among this cohort, over one-third (35.2%, 32/91) had tumors located in the head and uncinate process of pancreas, but only 1 patient presented with jaundice. This patient's CA 19–9 level was within normal limits, a pancreaticoduodenectomy was performed, and the pathological examination confirmed SPN.
Enhanced abdominal CT is the most widely used imaging technique to diagnose SPNs. The typical features seen on imaging are a well-circumscribed, encapsulated, heterogeneous mixed solid and cystic mass with calcification and signs of necrosis or hemorrhage.3,15,16 Typical imaging characteristics were found in 67% (61/91) of cases in this study. The presence of small solid masses or large unilocular cysts may complicate diagnosis. Small (≤3 cm) SPNs frequently appeared as purely solid tumors with sharp margins, while large atypical SPNs appeared as calcified solid masses or large cystic masses. 17 For atypical cases, SPNs must be differentiated from other pancreatic neoplasms, including pancreatic ductal adenocarcinoma, neuroendocrine tumor, and other pancreatic cystic tumors. MRI is more accurate at characterizing soft tissue, which can help clinicians distinguish SPNs from other tumors, in particular neuroendocrine tumors.18,19 EUS-guided fine-needle aspiration (EUS-FNA) is a reliable preoperative diagnostic tool that significantly increases sensitivity and specificity up to 91% and 94%, respectively.3,20,21 However, it must be emphasized that the accuracy of EUS and EUS-FNA depends on the experience of the operators and should only be performed by experienced clinicians. Additionally, cytology samples may be insufficient to form a diagnosis, and EUS-FNA can lead to tumor rupture in SPNs. 22 For these reasons, EUS-FNA is only recommended for select cases.
SPN is generally considered a tumor with low malignant potential. However, malignancy criteria for SPNs have not been clearly established. The WHO classification of tumors of the digestive system is usually used to differentiate benign and malignant SPNs. For malignant SPNs, imaging and pathological features include incomplete envelope, vascular invasion, perineural invasion, invasion into the surrounding tissues/organs, invasion into pancreatic parenchyma, or metastasis.7,23 Nishihara et al. 24 found that malignant SPN had a higher nuclear grade and more prominent necrobiotic nests characterized by aggregates of cells with pyknotic nuclei and eosinophilic cytoplasm.
Early detection and radical resection provide the best management strategy for this rare tumor. Due to its mild biological behaviors, low frequency of invading surrounding tissues or organs, and predominance in the younger population, SPN patients are good candidates for minimally invasive surgery (MIS). MIS for SPNs has been increasingly reported in recent years,25–27 and results have shown that MIS is safe and feasible for SPNs. SPN patients can benefit from the common advantages of MIS as well as comparable oncological outcomes and long-term survival, as seen in the open surgical approach. In our study, 30.8% of patients underwent laparoscopic surgeries and 89.3% (25/28) of these were performed in the last 5 years. No significant differences were observed in operation times, blood loss, or postoperative complications between the OP and LAP groups, but postoperative hospital stays were significantly shorter in the LAP group. Our results were consistent with those of previous studies and suggest that LAP should be the standard procedure for SPNs. It is important to note that SPN tumors are usually large and have rich blood flow, so aseptic inflammation often occurs in tissues surrounding the tumor. All these factors increase the difficulty of this surgical procedure; hence, it is recommended that MIS be performed by experienced surgeons in high-volume centers. Considering the favorable prognosis of SPN, organ-/function-preserving surgical procedures are recommended to reduce damage and long-term complications and also to ensure quality of life. However, for malignant SPN patients with liver metastases or locally advanced patients, aggressive radical resection or debulking operations should be performed to prolong long-term survival. 28 One patient in our study had undergone a debulking operation to treat a tumor 9 years before presenting at our hospital. This patient presented with local recurrence and liver metastasis 1 year ago, and we performed radical distal pancreatectomy with splenectomy and radiofrequency ablation for the metastatic lesions, this patient survived and reported no symptoms as of the last follow-up.
The SPN can be definitively diagnosed by routine pathological examination, which can also investigate its malignant potential. Microscopically, the solid pseudopapillary pattern with a rich microvasculature is identified as a typical pathological feature. 29 For some difficult cases, IHC can help distinguish SPNs from pancreatic neuroendocrine tumor, acinar cell carcinoma, and other pancreatic neoplasms. Vimentin, β-catenin, CD10, AAT, PR, and CgA (chromogranin A) are common markers to aid diagnosis. The first five markers are usually positive in SPN tissue, while CgA is usually negative in SPN, but positive in neuroendocrine tumors.3,14,30
SPN patients usually have favorable long-term survival after surgery, even if they suffer local invasion or distant metastasis. The 5-year survival rate is 95%–97%, with an estimated 10-year survival rate of ∼93%.14,31 In our study, the 1-, 3-, and 5-year overall survival rates were 100%, 97.9%, and 96.0%, respectively. Patients whose lesions present with malignant features may suffer from local recurrence or metastasis after initial surgery. The recurrence rate is reported to be 4.4% 6 ; thus, a planned follow-up program is warranted for these patients, and active management is recommended for patients with tumor recurrence or distant metastasis.
Conclusions
SPN usually occurs in young females as mixed cystic and solid masses, with calcification or hemorrhage as a typical imaging feature. CT or MRI can accurately diagnose this disease, while EUS and EUS-FNA are recommended for difficult cases. Laparoscopic or robotic organ-/function-preserving operations are the best surgical procedures for cases with no malignant features. However, aggressive radical resection should be performed in patients with local invasion or distant metastasis. Routine histological examination and IHC assessment can adequately distinguish SPNs from other tumors. Follow-up programs should be applied for SPN patients, especially for malignant cases.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Nos. 81702365, 81502508, and 81500496) and the Natural Science Foundation of Shandong Province, China (No. ZR2017MH090).
Compliance with Ethical Standards
Disclosure Statement
The authors have no relevant affiliations with any organization or entity with a financial interest in the subject matter or materials discussed in the article.