
Abstract
Abstract
Purpose:
Acute appendicitis (AA) is the most frequent surgical entity in the emergency department, but its correct diagnosis remains challenging. To improve diagnosis, clinical prediction rules (CPRs) have been created to establish objective scores for the probability of suffering AA. In this study, we establish scores indicating whether laparoscopy would be superior to clinical observation or repeat diagnostic test.
Methods:
A retrospective observational study was conducted with 433 patients submitted to surgery for suspected AA using a laparoscopic approach. The Alvarado, Raja Isteri Pengiran Anak Saleha Appendicitis, appendicitis inflammatory response, and adult appendicitis score scales were applied in each case to establish a high, medium, or low probability of suffering AA.
Results:
Of the 433 patients analyzed, 381 (88.0%) had AA. Twelve (2.8%) were converted to open surgery, and complications were observed in 54 (12.5%) cases. The CPRs studied showed statistically significant differences between AA and negative appendectomies. However, in patients with intermediate probability scores, the diagnostic accuracy of the CPRs evaluated was not adequate.
Conclusions:
Laparoscopic surgery can serve as a diagnostic tool for patients with intermediate AA probability scores because of its low associated morbidity and mortality and because it affords a direct diagnosis of the problem, allowing determination of the appropriate treatment.
Introduction
A
The diagnosis of AA is based mainly on clinical history, physical examination, and laboratory and imaging tests. However, accurately diagnosing AA remains challenging. 7 An estimated 20%–40% of cases are misdiagnosed, and the negative appendectomy (NA; normal appendix in the histological examination) rate is 10%–34%,3,8 with a 5%–10% NA rate accepted as appropriate to reduce the incidence of complications (perforation, peritonitis, etc.). 9
The universally accepted treatment for suspected AA is appendectomy; although it has not yet been established as the “gold standard,” 10 laparoscopic appendectomy is gaining acceptance because of its obvious advantages.11–13
Clinical prediction rules (CPRs) were created to facilitate the diagnosis of AA. These are systems of scales used to objectively determine the diagnostic probability of suffering AA.14,15 Among the numerous CPRs in existence, the best known are the Alvarado score (AS), appendicitis inflammatory response (AIR) score, Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score, and adult appendicitis score (AAS). In general, these diagnostic tools have acceptable efficacy for the extreme scores (low or high probability of AA), but a significant percentage of patients have an intermediate score, precluding the use of CPRs to confirm a diagnosis. In these situations, the options are to perform successive diagnostic studies and/or keep the patient under clinical observation. In this group of patients, laparoscopy, as a diagnostic and therapeutic procedure, could be an option that shortens the diagnostic process and allows early treatment.
In this study, we establish score intervals for the above CPRs at which laparoscopy would be a better strategy than clinical observation or new analytical and imaging studies.
Materials and Methods
A retrospective observational study was conducted. The clinical records of 500 patients evaluated for suspected right lower quadrant pain (RLQP) from January 2010 to December 2016 were reviewed. Of these patients, 458 patients underwent surgery for suspected AA. Twenty-five patients treated using an open approach were excluded. Diagnostic confirmation was obtained through the anatomopathological report, which indicated AA when the presence of inflammatory cells (leukocytes, lymphocytes, or plasma cells) in the surgical specimen was confirmed,16,17 or NA in the absence of these cells. 17
Once the patients were selected for inclusion in our study, we reviewed 433 clinical records. The information collected included demographic and personal data, clinical features, analytical data at admission, radiological data, intervention reports, and postoperative outcomes. With all this information the CPR scores were established:
AS: Introduced in 1986 by Alvarado, this scoring system was the first to facilitate AA diagnosis.
18
It is reliable for ruling out AA, and its implementation has been recommended in the emergency department and in primary care in areas with limited medical resources for the initial triage of patients with suspected AA.
19
It is considered the gold standard among CPRs. RIPASA score: This system was designed to increase diagnostic reliability in eastern patient populations (Asia, Pakistan, China, India, Egypt, and Eastern Europe).20,21 AIR score: In some studies of external validation, this system has been proven to be superior to the Alvarado scale.
22
In addition, its reliability is high even in the most complex patient groups, which can be difficult to diagnose.
23
AAS: This system was designed to improve the insufficient discriminative capacity of the previous CPRs in the adult population.
24
The scale allows clinicians to classify most patients into low- or high-probability AA groups, significantly reducing the need for diagnostic imaging tests.
21
The data obtained were entered into an anonymized database created in Microsoft Excel (Microsoft Corporation, Redmond, WA; EEUU) 2016 and were analyzed in IBM (IBM Corporation, Armonk, NY) SPSS Statistics version 20.0. In the descriptive analysis, the quantitative variables were reported as median and interquartile range (IQR). The qualitative variables were reported as frequencies and percentages of the total number of patients (N, %). The number of patients with AA or with a normal appendix according to each variable studied was established. We expressed this proportion relative to the total number of patients who fulfilled the respective condition (N, %). Associations between the qualitative variables were analyzed by the Pearson chi-square (χ2) test. Comparisons of the quantitative values were carried out using the nonparametric Mann–Whitney U test. A descriptive analysis was performed for the scores of each scale under investigation in the patients of our cohort. To determine the diagnostic value of these scales, an analysis was performed using receiver operating characteristic curves, with calculation of the area under the curve (AUC) for each scale. Then, the scores were stratified according to a low, medium, or high probability of presenting AA according to established guidelines in the literature for each scale: Alvarado,18,19 RIPASA,20,21 AIR,22,23 and AAS.24,25 Three possible probabilities were established as follows: low probability, which should exclude the diagnosis of AA and should therefore serve as an indication against surgery; high probability, which warrants surgical intervention without delay; and intermediate probability, which reflects “doubtful” circumstances warranting continuation of the diagnostic process.
Ultrasound scans were performed in all cases, and computed tomography (CT) was performed in 121 cases (27.9%). The results of these studies were recorded as positive when the radiological report was compatible with AA, negative when the radiological report specified a normal appendix or lacked pathological findings, and doubtful cases (DC) when the appendix was not visualized but when free fluid, mesenteric adenopathies, alteration of intestinal loops, and/or pericoecal fat were identified. To evaluate the impact of positive radiological results on the anatomopathological diagnosis of AA in the DC subgroup, univariate binary logistic regression was performed, and the odds ratio (OR), IQR, and P-value were calculated. The comparison of DC subgroups with nonpositive, negative, or doubtful radiological data versus the subgroup with positive findings was performed using the χ2 test.
The study was approved by the Clinical Research and Ethics Committee of this hospital. Informed consent was waived given the observational nature of the study. The data were treated confidentially and anonymously according to the provisions of Spanish Organic Law 15/1999 of December 13 of the Personal Data Protection (LOPD). 26
Results
We analyzed 433 patients who fulfilled the inclusion criteria: patients with RLQP suspected of AA and submitted to laparoscopic appendectomy. Of these, 381 (88.0%) patients had histological confirmation of appendicitis and 52 (12.0%) had a normal appendix. In 36 patients, the intraoperative appearance of the appendix was considered normal; however, in 10 of these patients (27.8%), the histological report confirmed the presence of AA.
The most relevant data of our patient cohort are summarized in Table 1. The median age of the patients was 31 years, with an IQR of 18.0–48.0 years. Most (249; 57.5%) patients were men. Conversion to open surgery was required in 12 of 443 patients (2.8%).
Values are given as median (IQR) and n (%).
CPR, C protein reactive; CT, computed tomography; IQR, interquartile range; NS, not significant; WBC, white blood cells.
Postoperative complications occurred in 54 patients (12.5%). Only 8 patients (1.8%) required invasive treatment (Grade IIIb Clavien–Dindo classification 27 ) by surgical reoperation. The mortality rate was 0.2% (1 patient); an older patient experienced perforated AA and fecaloid peritonitis complicated by septic shock.
The scales under investigation were applied to all patients of our cohort, all of which showed statistically significant results in terms of predictive ability and diagnostic performance (Table 2). The AUC of each CPR based on the probability of AA diagnosis is given in Table 3.
Values are given as median (IQR).
AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AS, Alvarado score; IQR, interquartile range; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AUC, area under curve; CI, confidence interval; CPR, clinical prediction rule; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
The risk stratification for AA of each CPR is given in Table 4. Of the four CPRs, the AS presented the most accurate diagnosis when the scores were high (high probability of AA), assigning a high probability of AA to 198 patients, 96.5% of whom had AA. The RIPASA was the least accurate when the scores were intermediate, assigning a medium probability of suffering from AA (DC) to 95.2% of the patients, compared with 36.7% for the Alvarado scale and 50.3% for the AAS. In the low AA probability subgroup, in which AA would be ruled out, the AIR score was most effective, as it identified 155 patients, 22.6% of whom did not have AA. From these data, we infer that all CPRs assigned a high number of patients to the intermediate probability subgroup (Table 5).
AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AS, Alvarado score; PTOS, points; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AS, Alvarado score; CPR, clinical prediction rule; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
The diagnoses were verified by imaging studies. Ultrasound scans were performed in all cases: AA was reported in 260 (60%) patients, including 243 patients for whom AA was confirmed by the histological report (sensitivity 63.8% and specificity 67.3%). The OR of a positive ultrasound scan in the DC group was associated with a higher probability of AA (Table 6).
AA, acute appendicitis; AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AS, Alvarado score; CI, confidence interval; NA, negative appendicitis; OR, odds ratio; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
For the patients with an intermediate probability of AA and nonpositive ultrasound results, we found that 74.2%, 80%, 89.5%, and 84.3% of the patients in the intermediate range of the AS, RIPASA, AIR, and AAS had AA, respectively (Table 7).
AA, acute appendicitis; AAS, adult appendicitis score; AIR, appendicitis inflammatory response; AS, Alvarado score; NA, negative appendicitis; RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
The last analysis carried out was for the DC group and inconclusive cases. In 121 patients, the diagnostic study was completed with CT; AA was confirmed in 95 patients, and the diagnosis was confirmed during laparoscopy in 84 (88.4%) of these patients (sensitivity 82.4% and specificity 42.1%).
From these data, we conclude that ultrasound is not very useful in patients with an intermediate probability of AA according to the CPRs studied.
Discussion
AA is the most frequent surgical emergency encountered by general surgeons and is the main cause of acute surgical abdomen, 28 which is often the reason for many first surgeries among adolescents and young adults. 29 The incidence is 1.1 cases per 1000 people per year,30,31 and the male-to-female ratio is 1.3:1, although this ratio appears closer to 1 in adulthood.32,33 Our cohort of patients complies with previously published data. We had a slight male predominance (57.5% versus 42.5%), with a male-to-female ratio of 1.35:1. The median age was 31 years (IQR = 18.0–48.0), confirming that this pathology is more frequent in the first decades of life. 6 The typical clinical presentation of AA is observed in only 60% of patients 34 compared with 14.1% in our cohort. In the remaining patients, the presence or absence of AA is less clear and can generate problems in diagnosis.
The main concern in the diagnosis of AA is that a delay will increase the risk of surgical complications. Delaying surgery 36 hours from the onset of symptoms increases the risk of appendicular perforation by 5% every 12 hours. 35 On the contrary, an inadequate diagnosis can lead to unnecessary operations and potential associated morbidity. 36
Although an NA rate of up to 20% is considered acceptable 37 in certain populations, such as older patients or women of childbearing age, the incidence of NA can reach 40%. 38 We recorded an NA rate of 12.0%, slightly higher to the 5%–10% rate accepted by the current literature. 39 However, these data are similar to that reported by authors with similar attitude in the presence of a macroscopically normal appendix during laparoscopic exploration. 9
As in the Dutch study by Lahaye et al., in our center, routine imaging is included in the diagnostic approach for patients with suspected AA, which should result in a lower NA rate. 40 However, ultrasound has a limited sensitivity and specificity for diagnosing AA because of several limitations, including observer dependence, obesity, scars from previous surgeries, and the location of the appendix.6,41,42 In addition, as reflected in the study by Kryzauskas et al., ultrasound use increases the number of negative appendectomies 31 by 6.5% according to our data.
Since their introduction, CPRs have been applied to improve the diagnostic approach in patients with suspected acute abdomen of the right iliac fossa with the aim of decreasing morbidity and NA rates. 43 These scales provide objective and standardized evaluations of patients with suspected AA. 43 Many scores have been created, but the score with the highest sensitivity or specificity remains unclear.
The heterogeneity of the methods and the quality of the studies available prevent meta-analysis, but 12 validated scales are available for the diagnosis of patients with suspected AA. 43 Our results showed a median AS of 6.0 [5.0–8.0] for AA and 5 [4.0–5.0] for NA (P < .001). Similar to previously published data, 44 we found that an AS ≥7 was associated with a high probability of AA: 93% in the cited study, and 96.5% in our study, which is a high positive predictive value. The AUC of the AS in our cohort was 0.74 [0.67–0.81] (P < .001), which is similar to that reported by Tekeli et al. in a study carried out over 3 years in 281 patients (0.78 ± 0.031) (P < .001). 45
Several studies have identified a correlation between the severity of inflammation and the AS.46,47 Our results do not support this finding.
Application of the RIPASA scale in our cohort also resulted in statistically significant differences between patients with AA and patients with NA, with an average score of 7.5 [6.5–9.0] (P < .001) and an AUC = 0.65 [0.57–0.73] (P < .001) in the former group. Specifically, this score of 7.5 is the most useful cutoff point for this scale, providing the best sensitivity and specificity as demonstrated by Butt et al. 46 Although the RIPASA score was statistically significant in our study, its AUC was lower than those of the other three scales tested, which is different from the data published by other authors, such as Chong et al., 20 who reported an AUC = 0.81 [0.74–0.88]. Ethnic differences in the population enrolled in this study may explain this discrepancy. However, other studies have implemented this scale in Western populations with good results. 21
Similar to the other scales, the AIR showed statistically significant differences between patients with AA and patients with NA (P < .001). This scale uses simple clinical criteria and two common laboratory tests (leukocyte count and PCR). 48 When these two tests yield high values, the probability of AA is five times as high as the probability associated with low values. 49 In our cohort, this scale had an AUC = 0.71 [0.63–0.80] (P < .001), revealing its adequacy as a probability scale, although this result is very different from those reported by other authors such as de Castro et al. (AUC = 0.96). 22
The AAS also showed significant differences between the AA and NA patients. Our AUC for this scale was 0.70 [0.62–0.78] (P < .001). Sammalkorpi et al. demonstrated the utility of this scale to decrease unnecessary imaging tests and the rate of NA. 25
When we compared the four scales in our patients, the Alvarado scale showed the best AUC (0.74), followed by the AIR and AAS (between 0.71 and 0.70) and RIPASA scales (0.63). These results contrast with those of other authors who found a higher AUC for the AIR scale22,23 or superior specificity for the AAS.6,50 Nevertheless, as confirmed in this study, CPRs do not lead to good results in a large number of patients. 51 Their diagnostic accuracy is acceptable for extreme scores, but it is not adequate for medium probability scores; greater diagnostic efficiency is needed for DCs. Our data show a high rate of AA in patients with intermediate scores. In these situations (DCs and nonconclusive imaging studies), patients may benefit from a laparoscopic procedure.
The laparoscopic approach as a diagnostic tool seems to be a reasonable option in the DC group, given its low morbidity and mortality. In addition, it enables intraoperative diagnosis that can lead to earlier and more appropriate management of clinical conditions. Our data suggest that this option should be considered in patients with intermediate scores for the CPRs: ASs between 5 and 6, RIPASA scores between 5 and 12, AIR scores between 5 and 8, and AASs between 11 and 15, in a similar manner to what The European Association of Endoscopic Surgery has proposed in the consensus document of 2016. 52
The use of laparoscopy as a diagnostic tool in patients with right iliac fossa pain of an uncertain etiology has been proposed by several authors.53–55 In a study published in the Cochrane Database of Systematic Review in 2014 conducted with women of childbearing age with unrelated abdominal pain, Gaitán et al. concluded that the use of laparoscopy as a diagnostic tool decreased the number of NAs. 55 However, none of these studies used CPRs in the diagnostic approach.
At present, the treatment for AA is always surgical. In recent years, numerous studies have raised the concern of whether the surgical approach to all AA patients, with the associated morbidity, mortality, and costs, is appropriate, 56 and several studies have advocated antibiotic treatment of uncomplicated AA because of its superior safety.10,57,58 Based on the available scientific evidence, conservative treatment of AA is not yet standardized and should not be considered a management option in DCs.
Once AA is confirmed, surgery is the only established option, but the ideal surgical approach remains controversial. The rate of laparoscopic appendectomy increased from 20.6% in 1998 to 70.8% in 2008 and has become the approach of choice in many institutions. 11 In our center, since 2005, the technique of choice for the management of AA patients has been laparoscopic appendectomy. Of the 443 laparoscopic appendectomies in this cohort, 12 (2.8%) were converted to open surgery, which is lower than the rate reported in most published studies, with conversion rates of up to 13%. 59 In a study conducted between 2008 and 2012, Minutolo et al. found a conversion rate of 1.4%, although their sample was only 139 patients. 11
One concern during laparoscopic appendectomy is how to proceed in the presence of a macroscopically normal appendix. The Dutch guide recommends not performing appendectomy in this situation. 60 The European Association for Endoscopic Surgery advocates not performing appendectomy if another intra-abdominal pathology justifies the clinical presentation, although the recommendations in the absence of another pathology are not definitive. 52 The Society of American Gastrointestinal and Endoscopic Surgeons states that, without other pathological findings, the decision to remove the appendix should be based on the individual considerations of each patient. 61 According to the literature, a normal appendix can be safely left intact, 62 whereas resection is associated with 6% morbidity. 63 Hamminga et al. established a score to evaluate normal vermiform appendices during laparoscopic explorations with the aim of avoiding unnecessary resection, morbidity, and costs. 64 We personally choose to perform appendectomy in these cases and justify this choice with the following reasons. Macroscopically normal appendices can harbor microscopic incipient pathology and eventually lead to a more severe abdominal condition. In our study, of the 36 appendices with a normal appearance intraoperatively, 10 (27.8%) were described as AA-like in the anatomopathological report. Second, incidental appendectomy may mitigate future clinical mistakes in the context of new episodes of acute abdominal pain, especially in certain population groups such as fertile women or young children.65,66 The low morbidity of incidental appendectomy recorded in our series (3 cases) suggests that the laparoscopic procedure is a good option for the management of DCs.
The laparoscopic approach seems to be a good initial option for patients with acute right iliac fossa pain and intermediate probability scores for the CPRs, allowing the surgeon to directly identify the source of abdominal pain and initiate early management. Therefore, we propose in this article the algorithm of action before the pain picture in the lower right quadrant of the abdomen (Fig. 1).
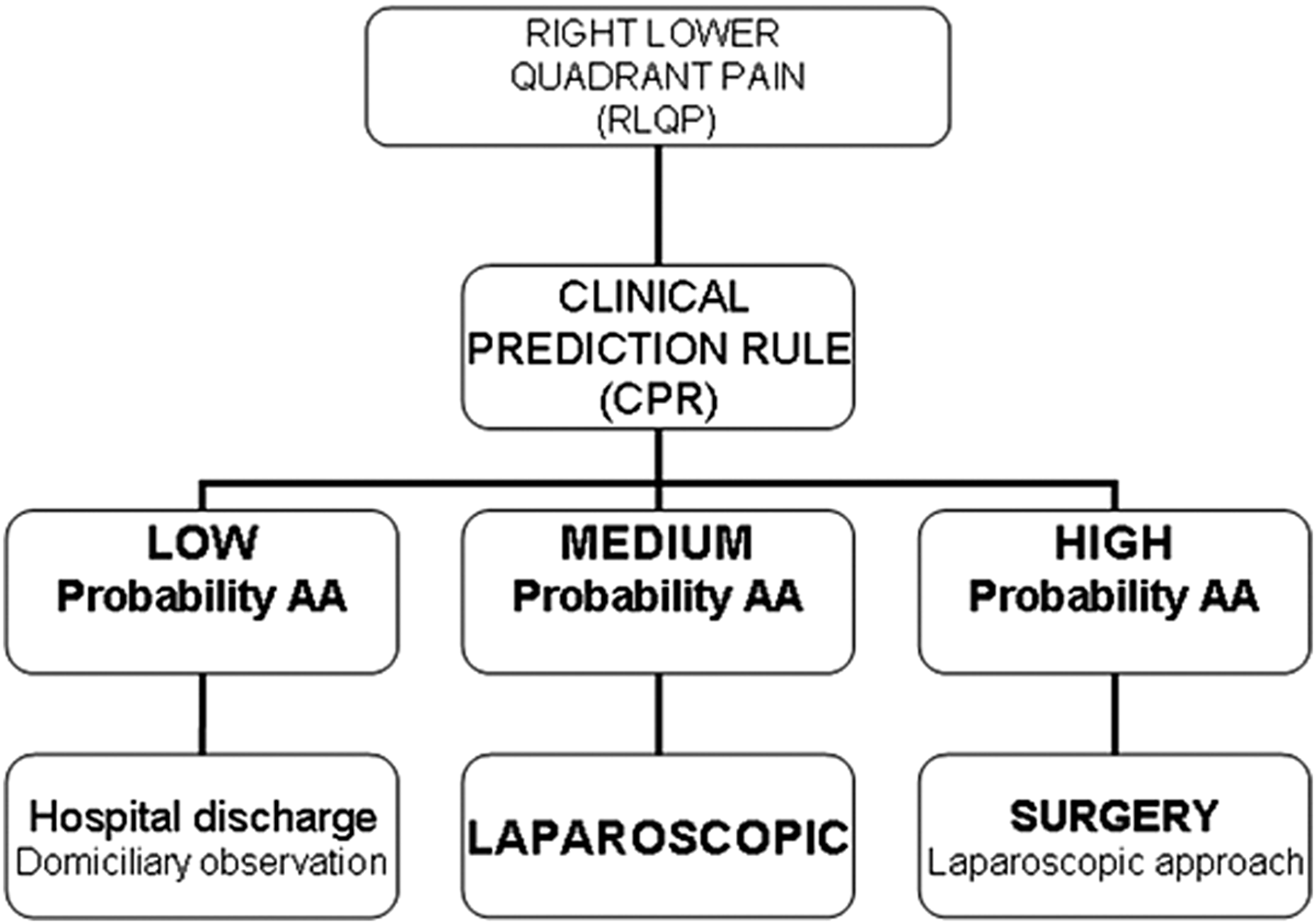
Performance algorithm for right lower quadrant pain because of suspected AA. AA, acute appendicitis.
In conclusion, CPRs are useful diagnostic tools for assessing abdominal pain in the right iliac fossa, especially when resources are limited. CPRs do not replace imaging tests when the latter are considered necessary. Of the four CPRs studied in our cohort, the AS was the most reliable, followed by the AIR. Laparoscopy should have an active and important role in the diagnosis of patients with an average probability of AA according to the CPRs.
Footnotes
Acknowledgments
The authors express deepest appreciation to all those who provided them the possibility to complete this report.
Disclosure Statement
No competing financial interests exist.