
Abstract
Abstract
Purpose:
The purpose of this study was to summarize the clinical experience of the laparoscopic percutaneous extraperitoneal closure of the internal ring using an epidural needle for the treatment of inguinal hernias.
Methods:
There were 1,142 children with an isolated inguinal hernia who participated in this study from January 2013 to May 2018. An epidural needle was used to treat the indirect inguinal hernia with laparoscopic assistance. Symptoms and signs were followed up at 1 week, 3 months, and every 1–2 years after the operation.
Results:
All 1,142 children underwent laparoscopic surgery successfully. All patients were discharged 1–2 days after the operation. During the hospitalization and follow-up, there were 21 patients with complications, including 6 cases of hernia recurrence, 7 cases of poor healing of the umbilical incision, 5 cases of suture granuloma and 3 cases of groin traction pain discomfort. None of the following complications occurred: abdominal wall vascular injury, deferent duct injury, umbilical hernia, iatrogenic cryptorchidism, testicular atrophy, hydrocele, or scrotal oedema.
Conclusion:
Laparoscopic percutaneous extraperitoneal closure of the internal ring using an epidural needle is a safe and feasible method for the treatment of inguinal hernias in children. This method has the advantages of less trauma, no scarring and a good cosmetic effect.
Introduction
Inguinal hernias are a common disease in pediatric surgery; the reasons are because the peritoneal sheath did not close or atresia occurred during the growth process.1,2 Isolated high ligation of the hernia sac can cure inguinal hernias in children. However, the traditional operation with a transverse or oblique incision in the inguinal area requires a complete separation of the hernia sac from the neck and high ligation, which would destroy the normal anatomical structure of the inguinal area, with the disadvantages of greater surgical injury, more obvious scar.3–6
With the improvement of laparoscopic instruments, the progress of surgical techniques, and the popularization of the concept of minimally invasive surgery, laparoscopic surgery has been widely used in the treatment of inguinal hernias, and has achieved a great therapeutic effect.7–12 Laparoscopic percutaneous extraperitoneal closure of the internal ring using an epidural needle to treat inguinal hernias is not only safe, reliable, and effective but also easy to perform and less traumatic, and it can realize the aesthetic requirement of no scar on the abdominal wall.13–17 In recent years, high ligation of the epidural hernia sac using an epidural needle with the assistance of a single-hole laparoscopy has been widely and successfully applied in various nations.7,9,13,18
Materials and Methods
This study was approved by the ethics committee of our university and strictly adhered to the tenets of the Declaration of Helsinki. All patients' guardians signed an informed consent form before the operation.
Patients
We retrospectively analysed the clinical data of 1142 patients with an isolated inguinal hernia in our hospital from January 2013 to May 2018, including preoperative, intraoperative, postoperative and follow-up data. Patients met the inclusion criteria if they presented with an isolated inguinal hernia. Patients were excluded from this study if they: (1) had other congenital deformities, such as cryptorchidism, hydrocele, etc.; (2) had an incarcerated hernia; (3) had a recurrent inguinal hernia; (4) refused to sign the consent form for surgery or refused to comply with the follow-up schedule.
According to the clinical manifestation and physical examination, all patients were positively diagnosed with an inguinal hernia, including 392 cases on the left side, 426 cases on the right side, and 324 bilateral cases, with 814 males and 328 females, and the age and weight were 3.7 ± 2.8, 4.3 years and 17.5 ± 6.4, 9.6 kg (Table 1). A routine clinical examination was performed before the operation, including an electrocardiogram, chest radiography and blood examination.
Clinical Data of the Patients in This Study (Mean ± Standard Deviation, Interquartile Ranges)
Technology
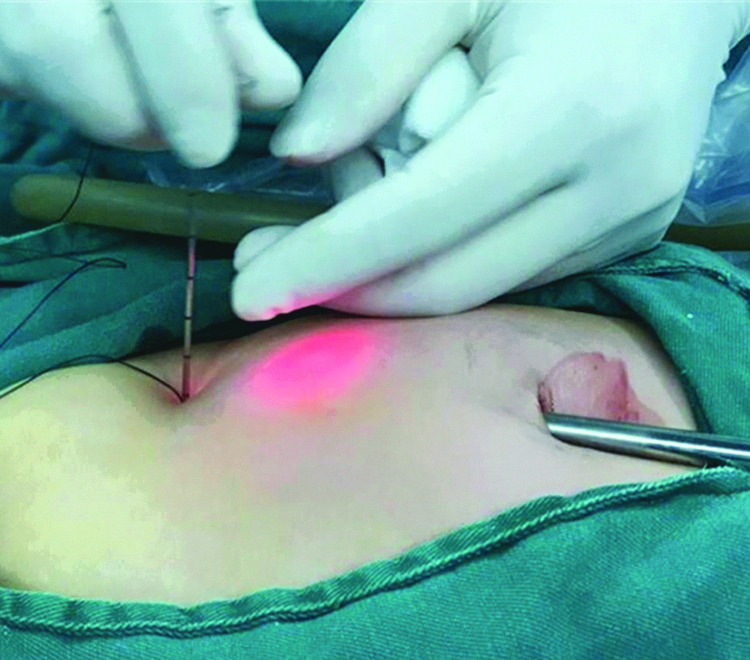
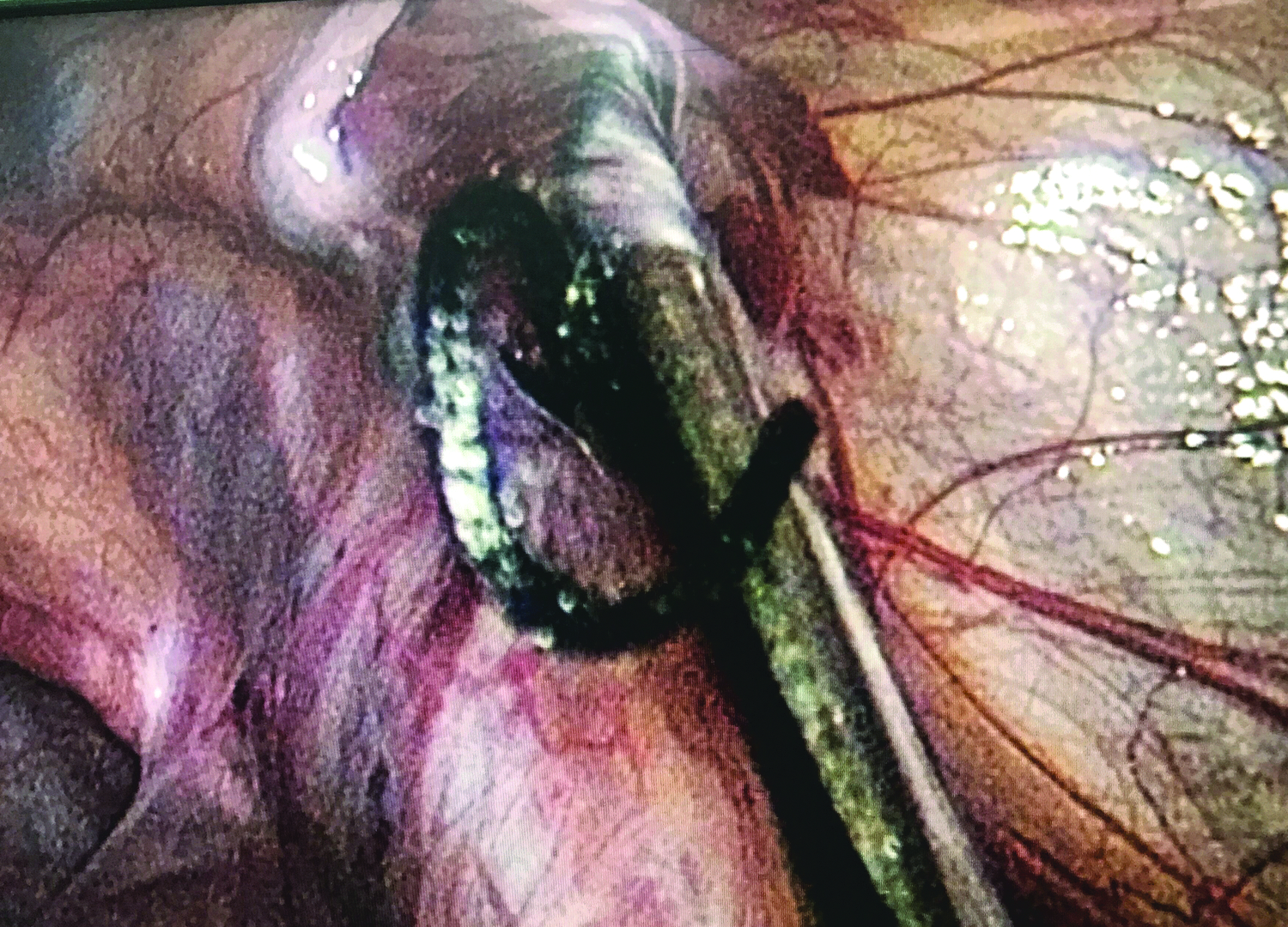
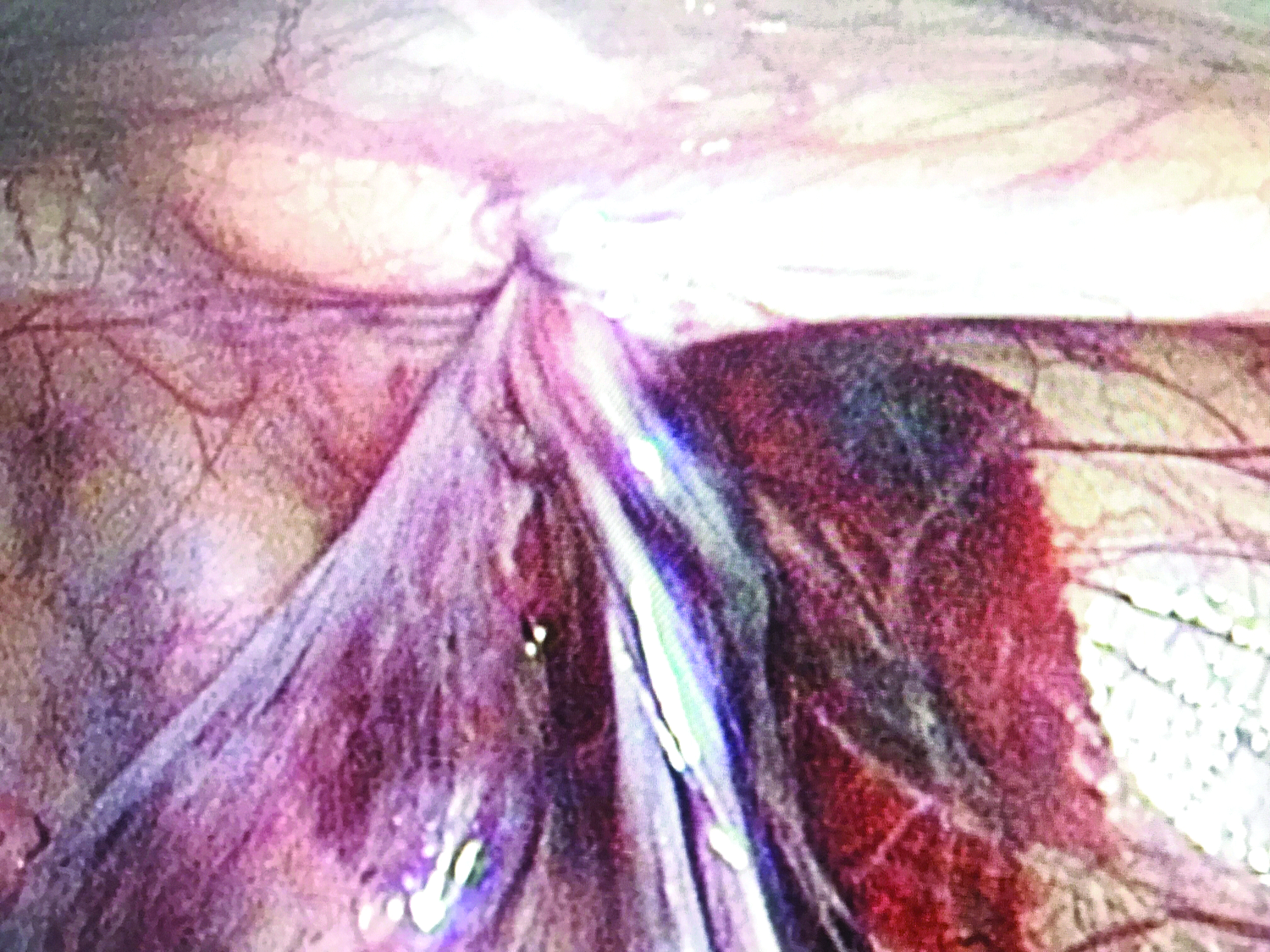
After anaesthesia, the patient was placed in a supine position with the waist slightly raised using a cushion, and then, we routinely disinfected and draped the surgical area. The umbilical skin was incised ∼5 mm layer-by-layer, and a 5 mm trocar was placed directly into the abdomen to establish pneumoperitoneum (12 mmHg). Then, we explored whether the bilateral inguinal canal was closed (Fig. 1). Under the guidance of a laparoscope, the skin was punctured at the unclosed side of the skin by the needle of a No. 12 syringe (Fig. 2), and the epidural puncture needle with double-stranded 2-0 not absorbable braided suture was punctured into the anterior wall of the inguinal tube through the anchor point (Fig. 3). We performed a sharp separation of the outer half-circle of the inner ring mouth at the extraperitoneal space and pulled the puncture needle out after the coil was pressed by the laparoscope (Fig. 4). The epidural puncture needle was pierced into the front wall of the inguinal tube again through an anchor point with a double-stranded 2-0 not absorbable braided suture. After sharply separating the inner half-circle of the inner ring mouth at the extraperitoneal space, the epidural puncture needle was pierced through the centre of the original coil (Fig. 5). We also used the laparoscope to press the coil and exit the puncture needle before tightening the front coil. The pierced coil was removed to bring out the second one, and one of the double strands was drawn out (Fig. 6). And then, we gradually tightened the coil with the inner ring until it closed under the laparoscope (Fig. 7). Finally, we tied a knot under the skin. If neither side of the inner ring was closed, the other side was treated the same way. After closing the inner ring, we carefully checked the abdominal cavity for bleeding, released the peritoneal gas, and removed the trocar before suturing the umbilical incision (Fig. 8).
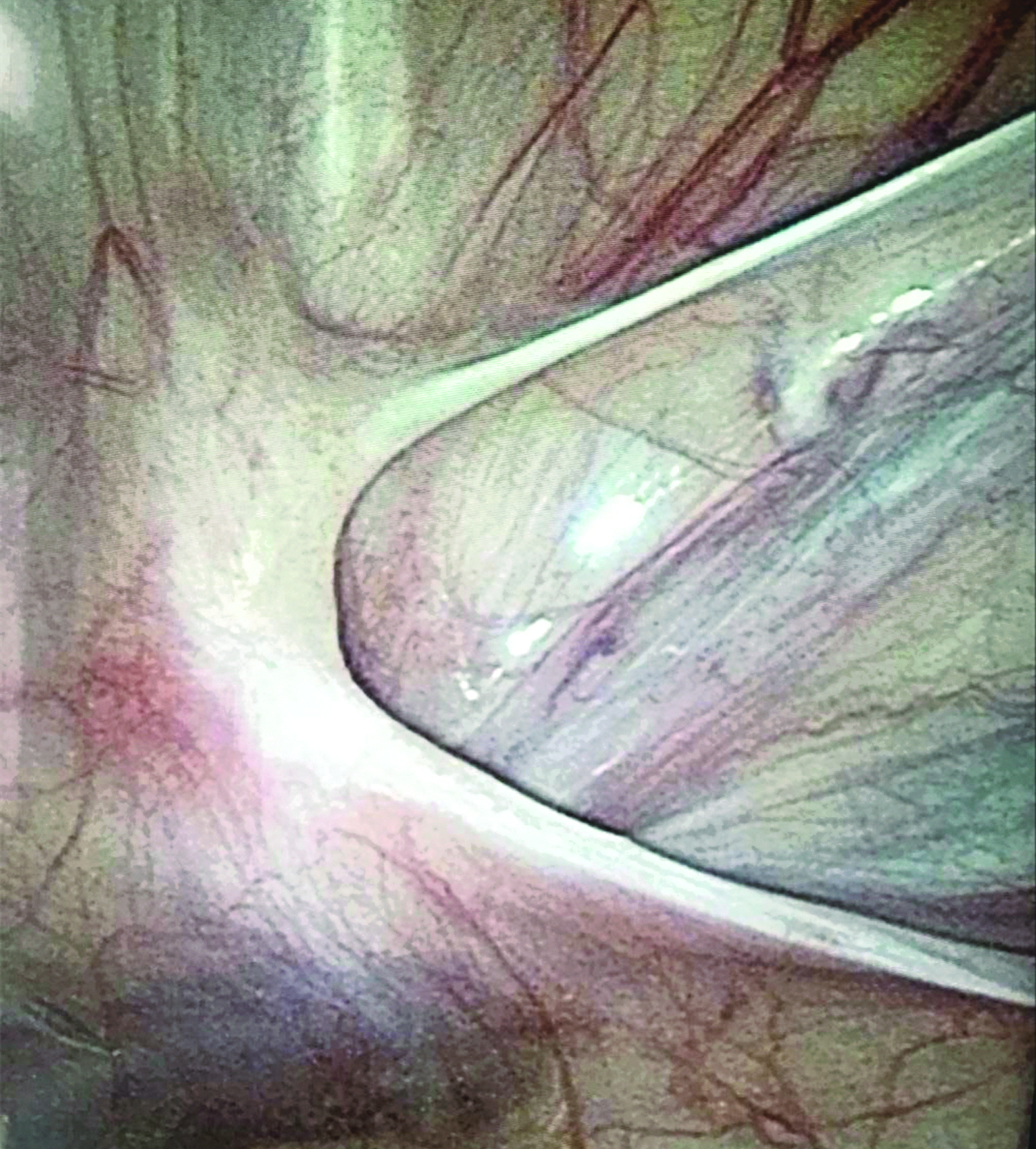
We explored the bilateral inguinal canal and found the internal ring was not closed.

The epidural puncture needle was punctured into the anterior wall of the inguinal tube through the anchor point.
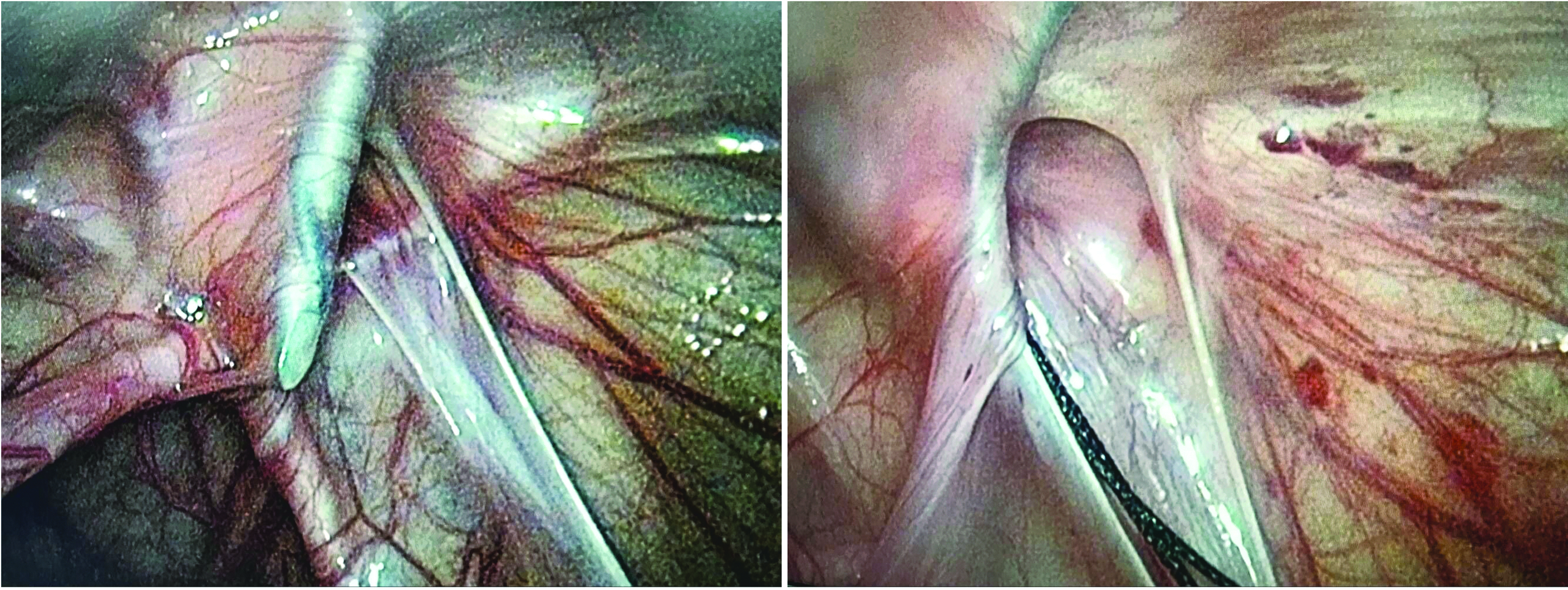
We performed a sharp separation of the outer half-circle of the inner ring mouth at the extraperitoneal space and pulled the puncture needle out after the coil was pressed by the laparoscope.
After sharply separating the inner half-circle of the inner ring mouth at the extraperitoneal space, the epidural puncture needle was pierced through the centre of the original coil.

The pierced coil was removed to bring out the second one, and one of the double strands was drawn out.
We gradually tightened the coil with the inner ring until it closed under the laparoscope.

Incision of postoperation.
If the abdominal cavity was very deep or there were many peritoneal folds at the inner orifice and it was difficult to puncture over the deferent duct, we injected normal saline through the puncture needle to increase the gap between the peritoneum and the deferent duct. Alternatively, a 3 mm incision can be made next to the umbilicus to place a grasping forceps for assistance.
The entire operation was performed by 2 associate chief physicians and 1 protomedicus from our hospital who followed the procedural protocol above. For all patients, the skin at the operative site, especially the umbilicus, was cleaned by the nurses and was followed by the procedural protocol before the operation; during operation the skin was disinfected with iodophor three times. After the operation, we did not use antibiotics.
Results
All 1,142 children with an inguinal hernia (including 392 cases on the left side, 426 cases on the right side and 324 bilateral cases) successfully underwent the laparoscopic percutaneous extraperitoneal closure of the internal ring using an epidural needle. Among them, 78 cases were assisted by grasping forceps and 35 cases involved hydrodissection. The operative time of unilateral and bilateral inguinal hernias was 18.4 ± 3.5, 5.2 minutes and 25.1 ± 3.2, 5.4 minutes, respectively. All patients were discharged 1–2 days after the operation (Table 1). During hospitalization and follow-up, there were 21 patients with complications, including 6 cases of hernia (not subclinical patent processus vaginalis) recurrence, 7 cases of poor healing of the umbilical incision, 5 cases of suture granuloma and 3 cases of groin traction pain discomfort. There were no complications of abdominal wall vascular injury, deferent duct injury, testicular vascular injury, umbilical hernia, iatrogenic cryptorchidism, testicular atrophy, hydrocele, or scrotal oedema. The 6 cases of hernia recurrence were cured by open operation, and the 7 cases of poor healing of the umbilical incision were cured after dressing change 1–2 weeks. The groin traction pain discomfort was disappeared after 6–12 months and the suture granuloma in inguinal region did not cause uncomfortable during follow-up, so that we did not treat it.
The follow-up period was 3 months to 5.5 years, and the median follow-up time was 3.7 years. The follow-up intervals were 1 week, 3 months, and every 1–2 years after the operation. The content of the follow-up included the symptoms and signs of the children, which were followed up via outpatient visits or telephone. All the patients were followed up in 1 week and 3 months after operation, 99.5% of the patients were followed up in 1 year, 97% of the patients were followed up in 2 years, 93% of the patients were followed up 3 years, 89% of the patients were followed up 4 years and 86% of the patients were followed up 5 years after operation. Seventy-eight percent of the patients were followed up by outpatient service and the residual patients were followed up by telephone.
Discussion
Hernia is a common disease in children, the cause of which is due to the absence of the peritoneal sheath.1,2 Children do not have the problem of a weak abdominal wall structure that is common in adult inguinal hernias. Therefore, most paediatric inguinal hernias do not need to be repaired via the abdominal wall structure, and only a high ligation of the hernia sac can be performed, which includes the traditional high ligation of the hernia sac and a laparoscopic high ligation of the hernia sac. 19 Traditional high ligation requires dissection of the inguinal canal structure, layer-by-layer through the anterior approach, to expose the spermatic cord and free the hernia sac. This procedure may damage the spermatic cord structure and cause iatrogenic cryptorchidism, or even testicular atrophy. Traditional high ligation would leave more obvious surgical scar and cannot discover subclinical patent processus vaginalis unless exploration with laparoscopic equipment during the operation,3–6 while the subclinical patent processus vaginalis are very common in paediatric inguinal hernias with the incidence rate about 21.2% 20 ; and a part of the patients with subclinical patent processus vaginalis would appear symptoms late and require surgery. The laparoscopic high ligation of the hernia sac directly reaches the peritoneum by a blunt needle under direct vision, avoiding the anatomy of the groin structure, causing less trauma, and leaving almost no surgical incision on the abdominal wall, and subclinical patent processus vaginalis can be found and treated at the same time. This method has the advantages of less trauma and good cosmetic results, as a result, it has been widely used in clinical practice and has achieved good clinical effects.18,21–23 However, laparoscopic high ligation of the hernia sac requires high anaesthetic depth, and there may be certain complications regarding the abdominal puncture. 24
Laparoscopic percutaneous extraperitoneal closure of the internal ring uses a spinal epidural needle laparoscopically placed into the abdominal cavity. The simple puncture technique can be accomplished by external ligation without special practice of laparoscopic suture techniques, and the method is safe, simple, reliable, and easy to master. In this study, 1,142 children with an inguinal hernia were successfully operated. Compared with conventional surgical methods, laparoscopic surgery has the following advantages: First, no special equipment is required. Conventional laparoscopic instruments, epidural needles, No. 12 syringe needles and 2-0 braided suture can be used to complete the operation, so the procedure can be carried out in most hospitals. Second, it reduces the trauma of a laparoscopic multi-hole operation. The 5-mm observation hole is hidden in the umbilical fold. There is only a needle hole in the hernia area, and almost no scar is left after healing, so the cosmetic effect is very good. Third, under the condition of laparoscopic enlargement, anatomical structures such as the bilateral internal ring orifice, inferior epigastric artery, vas deferens and spermatic vessels can be clearly identified, making it hard to injure the inferior epigastric artery, vas deferens and spermatic vessels. The procedure is easy to perform and easily mastered by surgeons; it is also convenient for detecting contralateral patent processus vaginalis in time and addressing it during the operation to avoid a part of this patients appear symptoms late and require secondary surgery. In this study, 112 cases of subclinical patent processus vaginalis were found. Fourth, the small trauma and the postoperative pain is light, which reduces crying in children.
A puncture injury is a common complication of laparoscopic surgery. 24 There are inferior epigastric arteries and veins in the anteromedial ring of an inguinal hernia, and genital vessels outside the posterolateral peritoneum. There are external iliac arteries and veins outside the dangerous triangular peritoneum between the vas deferens and spermatic cord. The needle will be adjacent to these important vessels when it sneaks along the extraperitoneal space of the inner ring, and inadvertent operation will cause puncture damage. Therefore, when selecting the puncture point on the body surface, we should project the inferior abdominal vessels outside the inner ring, and use the laparoscopic lens close to the inner ring to take care of the intraabdominal blood vessel, to avoid needling the blood vessels into the abdominal wall. The operation should be gentle and stay close to the peritoneum during the course of the puncture, and attention should be paid to the direction of the hernia needle, especially when crossing the vas deferens and testicular vessels, to avoid damage to them. In difficult cases, physiological saline can be injected through the puncture needle to increase the gap between the peritoneum and vas deferens so that the puncture needle can be crossed across the vas deferens, or another 3 mm incision can be made next to the umbilicus to place a grasping forceps for assistance. According to the above principles, no complications of abdominal vascular injury, vas deferens injury, or testicular vascular injury occurred in this study.
Whether a traditional open surgery or laparoscopic surgery is performed, there are problems with postoperative recurrence.25,26 The causes of hernia recurrence after laparoscopic surgery include giant hernias, incomplete peritoneum ligation, the accidental slippage of knots, etc. 27 In this study, there were 6 cases of recurrent hernias, 3 of which were giant hernias. The initial operation for a giant inguinal hernia consisted of only a simple ligation of the inner ring, and surgery found that the ligation line slipped to the distal side of the hernia sac, indicating that if the inner ring is wide, the peritoneum around the inner ring ligation is loose. With the increase of abdominal pressure, the peritoneum of the inner ring slid into the defect and broad inguinal canal, leading to postoperative recurrence. Therefore, for giant hernias, we can use the puncture hook to cover the medial umbilical fold of the same side and strengthen the repair to prevent recurrence.28,29 No ligation line was found during the reoperation of 2 cases of recurrent hernia, which may be due to loosening of the ligation line; therefore, the knot should be tied exactly during ligation, and at least three single knots tied before clinging to the line knot cut-off. Another case of hernia recurrence was due to incomplete peritoneal ligation of the internal ring, so the position of the ligated hernia inner ring must be high enough, the ligation line must be in a complete circle, and the suture should be tightened to avoid hernia recurrence caused by leaving gaps. Before ligating the hernia sac, the residual gas in the hernia sac must be discharged. Otherwise, it may lead to gas accumulation in the distal hernia sac, and when ligating the hernia ring, the testicle should be properly pulled to prevent scrotal pneumocele and iatrogenic cryptorchidism.
There were 5 cases of inguinal suture granuloma and 3 cases of inguinal traction pain and discomfort. The reason may be that the different abdominal tunnels formed by two needle punctures caused more abdominal wall tissue to be ligated in the knots, so that in some cases the knots could only be subcutaneously located, and even carried the risk of ligating the abdominal nerves and vessels, resulting in postoperative local discomfort, pain, knot reaction and local foreign body sensation. 30 Therefore, complications such as subcutaneous knots, foreign body reaction, groin pulling pain and discomfort can be greatly reduced by ensuring the introduction and pulling of the ligation line through the same puncture tunnel and avoiding ligating excessive abdominal wall tissues. 31
Although the results of our study, with the largest number of cases, are promising, there are still several limitations. First, this was a single-centre study, and more research from multiple centres is mandatory to assess the effectiveness and complications of this technique in further studies. Second, this study was a retrospective review without a control group.
Conclusion
In conclusion, laparoscopic percutaneous extraperitoneal closure of the internal ring using an epidural needle to treat inguinal hernias is a safe and feasible alternative to conventional surgery. The cosmetic results are impressive and the follow-up results are promising.
Footnotes
Acknowledgments
We highly acknowledge the contribution by the participating doctors: Yi-fan Fang, Bing Zhang, Ming-kun Liu, Jian-cai Chen, Jian-xi Bai, Wen-chen Xu, Yuan-bin He.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of our university and strictly adhered to the tenets of the Declaration of Helsinki. In addition, all patients' guardians signed an informed consent form before the operation.
Authors' Contributions
Y.-J.W., Q.L.Z. and C.M.Z. designed the study, collected the clinical data, performed the statistical analysis, participated in the operation, and drafted the manuscript. L.C., Y.L., J.Q.Z., D.M.W., W.H.H. participated in the operation and revised the article. All authors read and approved the final manuscript.
Consent for Publication
All authors read and approved the final manuscript and publication.
Disclosure Statement
No competing financial interests exist.