
Abstract
Abstract
Background:
Colorectal cancer, one of the most common tumor- and cancer-related deaths worldwide, requires a multidisciplinary management including neoadjuvant chemoradiotherapy and surgery. Laparoscopic surgery for rectal cancer is gaining popularity due to its safety profile and good oncological results, if performed by experienced surgeons in specialized centers. This study describes our 10 years experience in minimally invasive rectal cancer surgery.
Methods:
We have retrospectively evaluated a series of 140 patients treated with laparoscopic approach for rectal malignant and benign diseases.
Results:
A total of 134 patients (95.7%) underwent anterior rectal resection, in the remaining 6 cases (4.3%) abdominoperineal amputation was performed. All but 13 cases have been treated with laparoscopic approach, with conversion rate of 5.7%. Postoperative morbidity rate was 8.6% (2 cases of peritoneal bleeding and 10 cases of anastomotic fistulae; in 2 cases, fistula occurred in patients previously treated with chemoradiation).
Conclusions:
Conventional laparoscopy can provide adequate oncological outcomes even in patients with advanced rectal cancer, with advantages in terms of postoperative hospital stay, recovery time, acceptable operative time, and low complication and conversion rates.
Introduction
Colorectal cancer is the third most common cancer in developed countries and the third leading cause of cancer death 1 ; rectal cancer, which makes up nearly one-third of colorectal cancer cases, 2 is often difficult to treat and carries a much higher risk of local recurrence. 3
Rectal cancer often requires multidisciplinary management, including neoadjuvant chemoradiotherapy and surgery. 4
Several prospective randomized trials have demonstrated that laparoscopic surgery for rectal cancer is a safe and feasible procedure. The quality of the surgical specimen and the long-term oncological outcomes of laparoscopic surgery are equivalent to those of open surgery; however, recovery, physiological function, and other short-term outcome measures improve after laparoscopic surgery. 5 However, laparoscopic surgery for rectal cancer is technically demanding, limiting its application in nonspecialized centers, and the effect of laparoscopic surgery varies somewhat according to surgeon volume6,7; moreover, in the past years there had been concern regarding the safety of laparoscopic colectomy after reports of cancer recurrence in the abdominal wall 8 ; laparoscopy in patients with distal rectal cancer was associated with a lower rate of involved circumferential resection margin and a lower locoregional recurrence rate than open surgery, mainly due to a better visualization and dissection in narrow spaces such as the pelvis. 9
Recent studies also demonstrated that laparoscopy and robot-assisted rectal cancer surgery in specialized centers provide overall comparable results, especially in terms of overall and disease-free survival 9 ; the less surgical trauma associated with the use of laparoscopic technique seems to reduce tumor recurrence, especially in patients with stage III disease and lymph nodes involvement. 10 Laparoscopic approach also leads to an attenuated stress response and to a improved preservation of immune function. 11
This study describes our 10 years experience in minimally invasive rectal surgery, with attention to technical aspects, surgical method, and postoperative short-term outcomes.
Materials and Methods
From January 1, 2008 to December 31, 2017, 140 patients, 79 males (56.4%) and 61 females (43.6%), median age 68 years old (range 30–89), were consecutively admitted to our institution to undergo rectal resection.
Preoperative diagnosis was proximal rectal cancer in 52 cases (37.9%), mid third rectal cancer in 58 cases (41.4%), distal rectal cancer in 24 cases (17.1%), rectal endometriosis in 3 cases (2.1%), and postrectal resection anastomotic stenosis in 3 cases (2.1%).
Preoperative radiochemotherapy was applied in 49 patients (35%) with locally advanced mid and distal third rectal tumor.
All patients were admitted to hospital the day before the surgical procedure, intestinal preparation was never administered, a total dose 600 mg of symeticon was routinely used to reduce bowel distension, and preoperative endoscopic tumor tattooing was not routinely performed.
All patients included in the study provided signed written informed consent for surgical procedure, blood transfusion, and sensitive personal data processing.
For each patient included in the study, the following data were recorded: gender, age at admission, comorbidities, type of treatment, total and postoperative hospital stay, and postoperative morbidity.
Patients' surgical risk was classified by the American Society of Anesthesiologists physical status classification system.
Normally we use three trocars; the standard positions for trocars was considered as follows: 5 mm ∼2 cm above umbilicus; 10 mm on transverse umbilical line, left hypochondrium, 12 mm in left iliac fossa (Fig. 1); after laparoscopic exploration of peritoneal cavity, the first step of the surgical procedure consists in performing inferior mesenteric artery ligation at the origin; left colon mobilization was then completed, thus rectum was isolated and transected with a radical total mesorectal excision (TME). A periumbilical mini laparotomy was conducted, with extraction and transection of the colon; after abdominal closure, a tension-free transanal mechanic terminoterminal anastomosis (Knight Griffen technique) was performed; methylene blue test or hydro pneumatic test was not routinely performed.

Trocars' position for laparoscopic rectal resection.
Overall global and per stage survival was evaluated by drawing Kaplan–Meyer curves.
Results
A total of 134 patients (95.7%) underwent anterior rectal resection; in the remaining 6 cases (4.3%), abdominoperineal amputation was performed.
Laparoscopic approach has been conducted in 123 patients (87.9%), regardless the distance of the tumor from the anal margin; direct open surgery was considered in 13 patients in whom macroscopic pelvic neoplastic infiltration was detected by preoperative imaging; other 4 patients were approached open due to previous major abdominal surgery.
Local radical R0 resection with a disease-free distal margin of at least 2 cm was achieved in all cases; the median number of harvested lymph nodes was 23 (range 11–38); histology demonstrated a complete and adequate TME in all cases.
Terminoterminal mechanic transanal colorectal anastomosis was applied in 110 procedures (78.6%); anastomosis was protected by temporary lateral ileostomy or colostomy only in 35 cases (31.8%); the remaining 30 patients underwent Hartmann procedure (24 cases) and abdominoperineal amputation (6 cases).
Temporary enterostomy was considered only in cases of very low rectal resection with the anastomosis 4 cm or less from anal margin in cases previously treated with chemotherapy and radiation; Hartmann procedure was reserved to elderly patients with advanced stage tumors and low life expectancy.
Colon transection was routinely conducted following an oblique line, to preserve mesenteric tissue, thus providing an adequate vascularization to the proximal stump and permitting the insertion of a 29 circular stapler anvil for transanal colorectal anastomosis.
Mean operative time was 75 minutes (range 40–210).
Conversion rate was 5.7%: 3 cases required conversion to open procedure because of macroscopic pelvic infiltration; 4 procedures have been converted due to the impossibility to detect the tumor at laparoscopic exploration. Three patients who underwent neoadjuvant treatment required conversion to open procedure.
No perioperative mortality occurred.
Overall postoperative morbidity rate was 8.6%; we recorded 2 cases of peritoneal bleeding requiring reoperation (1.4%) and 10 anastomotic fistulae (7.1%); 8 fistulae occurred after laparoscopic surgery, 2 in patients treated with open approach. In 2 cases, fistula occurred in patients previously treated with chemoradiation. Conservative treatment was applied in 4 cases; the other 6 patients with anastomotic fistula required reoperation (anatomotic resection and reanastomosis with ileostomy in 4 cases, Hartmann procedure in 2 cases); overall morbidity in patients treated with laparoscopic and open approach was, respectively, 8.1% and 11.8%. Perioperative results in relation to the surgical approach are summarized in Table 1.
Perioperative Surgical Results After Rectal Resection (Laparoscopic Versus Open)
n.s., not significant.
Overall survival analysis divided for stage disease is shown in Figure 2.
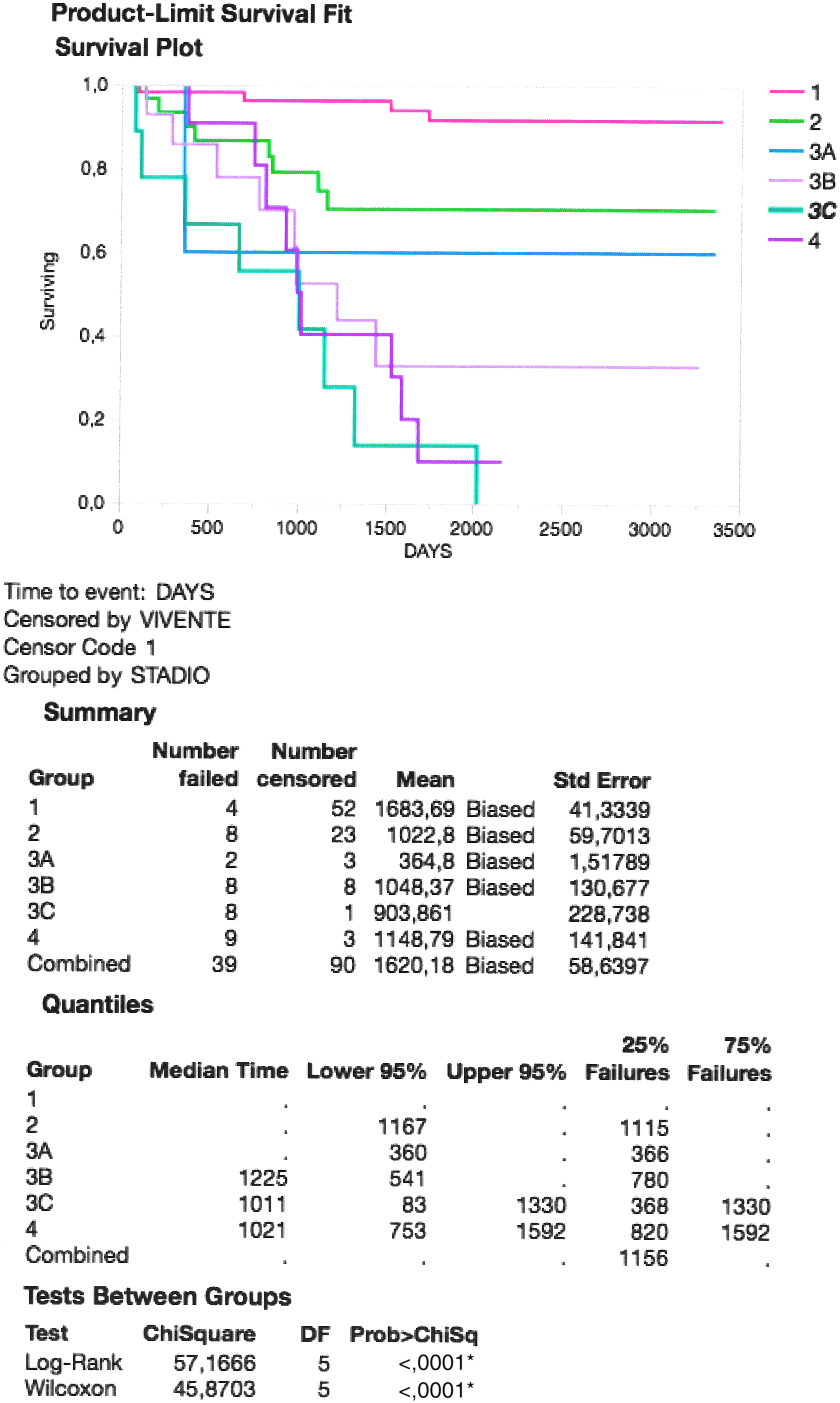
Overall survival divided by disease stage. *denotes the statistical significance of the result.
Discussion
Rectal cancer remains a common and complex surgical problem; there is growing evidence that minimally invasive surgery can provide ideal care for patients with rectal cancer. 12
Minimally invasive surgery demonstrates itself to be related to decreased analgesic use, shorter length of stay, and faster postoperative recovery. 13 Several in vitro and in vivo studies also show a reduced tissue expression of cytokines and flogosis biochemical markers, thus indicating a weaker inflammatory activity potentially adding to the clinical benefits observed in patients undergoing laparoscopy. 14
Although the employment of laparoscopy for colorectal cancer is spreading worldwide, high-volume hospitals with experienced surgeons may offer a better multimodality treatment, especially for advanced tumors. 15
Robot-assisted rectal resection is gaining popularity, but limited data are available regarding safety and efficacy; some studies demonstrated that among patients with rectal cancer suitable for curative treatment, robot-assisted surgery, if compared with conventional laparoscopy, does not show significant advantages in terms of intraoperative and postoperative complications, 30 days mortality, urinary and sexual dysfunction, and conversion rate, suggesting that robotic surgery does not confer an actual advantage in rectal cancer resection. 16
Among the technical aspects that should be taken into consideration in oncological rectal surgery, particular attention has to be paid to vascular ligation and mesorectal excision. Although distal mesenteric artery ligation with left colic artery preservation has been related by some authors with lower incidence of anastomotic leakage due to a better blood supply, large multicentric trials demonstrated that a more powerful disease staging achieved with the high tie overweighs the risk of dehiscence. 17
TME is the gold standard for cancer rectal surgery; however, it is hardly achievable with the laparoscopic technique in a number of cases due to anatomic issues 18 ; in our experience, an adequate mesorectal excision has been achieved in all cases. Transanal TME (TaTME) may benefit from pneumodissection ad expedites the laparoscopic step; anyway, the safety and cost-effectiveness of the procedure still warrant consideration 19 ; compared with laparoscopic TME, advantages of TaTME on pathological outcomes remain nowadays undetected. 20
Our 10 years experience of rectal resection, mainly conducted for malignant disease, strongly demonstrates the safety and effectiveness of the laparoscopic approach, even in patients with locally advanced tumor, requiring neoadjuvant chemoradiation (35% in our series) and in metastatic disease; laparoscopy would have permitted to achieve also partial bladder resection (1.4%) or hysterectomy (2.1%) in cases of cancer infiltration, and liver metastasis resection or ablation (5.7%).
Of the 140 cases enrolled in our retrospective study, “d'emblée” laparotomic approach has been employed in a restricted number of patients (12.1%); the choice of avoiding laparoscopy was mainly related to the prevision of an impossibility to perform the laparoscopic resection of very large cancers adherent to the presacral fascia, and in subjects with history of previous abdominal major open surgery.
High inferior mesenteric artery ligation and conventional TME led to a radical oncological resection in all cases, with adequate number of harvested lymph nodes and disease-free resection margins.
Hartmann procedure has been performed in elderly patients with metastatic disease and low life expectancy (17.1%).
Unprotected terminoterminal mechanic tension-free anastomosis has been performed in the majority of the patients of our series, without the employment of intraoperative methylene blue or hydropneumatic tests. Protection with temporary loop ileostomy was reserved only to cases of locally advanced tumors previously treated with chemoradiotherapy, with high risk of dehiscence (30.1%).
The employment of radiofrequency scalpel allowed us, in the past years, to achieve bloodless dissection while accelerating the operative time.
Overall postoperative complication rate was 8.6%, with an incidence of anastomotic fistula of 7%; no significant differences in terms of morbidity were recorded among patients treated with laparoscopy versus open procedure; even taking into consideration the statistical limit in comparing 2 inhomogeneous patient groups in terms of numerosity, the main advantages of laparoscopy in our experience have been demonstrated in the average operating time and mean blood loss.
Our 6% conversion rate, related to 3 cases of laparoscopically unmanageable pelvic infiltration and to 4 cases of undetectable tumor position, seems to be comparable with the results of other large series published studies,20,21 and could probably have been lowered to <3% by introducing a routinely preoperative endoscopic tattooing, especially in patients affected by small rectal tumors.
Mid- and long-term follow-up demonstrated a globally high overall survival rate especially for stages 1, 2, and 3A tumors, being a locally advanced disease with lymph nodes involvement the main independent predictor of worse prognosis.
Laparoscopy is the last diagnostic step and the first therapeutic step for malignant and benign pathology of rectum. With laparoscopy, we can explore the abdominal cavity, the viscera, and the peritoneum, then we can start the dissection of the colon–rectum and if it is possible complete a correct mesorectal excision. Laparoscopy is recognized to be less traumatic than open technique, allowing a better and faster recovery of the patients. In our series of patients, the oncological outcome at 5 years is comparable with the results in the literature. 22
Our experience shows that conventional laparoscopy can provide adequate oncological outcomes even in patients with advanced rectal cancer, with advantages in terms of postoperative hospital stay, recovery time, acceptable operative time, and low complication and conversion rates.
Laparoscopic surgery after neoadjuvant chemoradiation for low and mid third rectal cancer is associated with similar long-term outcomes when compared with open surgery.
Inferior mesenteric artery ligation at the origin and conventional TME seem to provide better oncological results without increasing morbidity; the actual benefits of robot-assisted surgery and of the TaTME still need to be demonstrated.
Footnotes
Authors' Contributions
A.O. designed this study and wrote the article after collecting all data. S.O. designed this study. He performed the greatest part of rectal resection and revised the article before submission. G.C. collected all data about patients' surgical outcomes and follow-up, and supervised the statistical analysis. M.U. collected patients' follow-up and performed the statistical analysis of data. F.C. revised the article before submission and conducted the bibliography research. R.G. collected patients' follow-up data and literature review. S.M.C. performed statistical analysis and revised the “results” paragraph. R.V. revised the “discussion and conclusion” paragraphs and collected data about surgical outcomes.
Disclosure Statement
All authors of this article declare no conflicts of interest.