
Abstract
Abstract
Background:
Laparoscopic pancreatectomy (LP) is increasingly performed with several institutional series and comparative studies reported. We have applied LP to a variety of pancreatic resections since 2004. This article is to report results of 15-year practice of 605 LPs for pancreatic and periampullary diseases.
Methods:
Patients with benign or malignant diseases in the pancreas and periampullary region, who underwent LP from June 2004 to June 2018, were retrospectively reviewed. The demographics and indications, and intraoperative and perioperative outcomes were evaluated.
Results:
A total of 605 consecutive LPs were analyzed, including 237 (39.2%) distal pancreatectomy with splenectomy (DPS), 116 (19.2%) spleen-preserving distal pancreatectomy (SPDP), 30 (5.0%) enucleation (EN), 30 (5.0%) central pancreatectomy (CP), 186 (30.7%) pancreatoduodenectomy (PD), and 6 (1.0%) pancreatoduodenectomy with total pancreatectomy (PDTP). The most common pathologic finding was pancreatic ductal adenocarcinomas (146, 24.1%). Conversion to open procedure was required in 22 patients (3.6%) (12 with PD, 8 with DPS, 1 with CP, and 1 with PDTP). The mean operative time was 241.5 ± 105.5 minutes (range 50–550 minutes) for the entire population and 367.1 ± 61.8 minutes (range 230–550 minutes) for PD. Clinically significant pancreatic fistula (ISGPF grade B and C) rate was 12.4% for the entire cohort and 16.1% for PD. Rate of Clavien-Dindo III-V complications was 17.4% for the entire cohort and 23.7% for PD. Ninety-day mortality was observed only in the cohort of patients undergoing PD (n = 4).
Conclusions:
The LP procedure appears to be technically safe and feasible, with an acceptable rate of morbidity when performed at our experienced, high-volume center. However, PD has less favorable outcomes and needs further evaluation.
Introduction
Although first introduced in the mid 1990s, laparoscopic pancreatectomy (LP), especially pancreatoduodenectomy (PD), has not been as widely adopted as other surgical techniques, presumably due to anatomic complexity of the region and complicated reconstruction leading to morbidity. 1 Therefore, while LPs needing no reconstruction like distal pancreatectomy (DP), and enucleation (EN), are frequently performed in various institutions, PD and central pancreatectomy (CP), in which the complicated anastomosis is necessary, are still uncommon and only performed in high-volume centers by experienced surgeons. 2
The laparoscopic distal pancreatectomy (LDP) with or without splenectomy was first proposed by our team in 2003.3,4 In addition, we successfully performed laparoscopic CP in 2011 and laparoscopic pancreatoduodenectomy (LPD) in 2012, thus transferring this technique from the phase of innovation to the phase of development.5,6 This long development process could be related to the learning curve in which technical refinements improve outcomes. In this study, we report the surgical outcomes of 605 patients who received LPs in the course of 15 years, which have passed since its first application.
Materials and Methods
Patients
This study was approved by the Ethics Committee of Zhejiang University. Written consent was obtained from every patient before surgery. The data for 605 consecutive LPs performed at Sir Run Run Shaw Hospital during the 15 years from June 2004 to June 2018 were retrospectively reviewed. The procedures were classified into six categories: EN, distal pancreatectomy with splenectomy (DPS), spleen-preserving distal pancreatectomy (SPDP), CP, PD, and pancreatoduodenectomy with total pancreatectomy (PDTP).
Patients were evaluated in an intention-to-treat manner. The evaluated variables were the patients' demographics, surgical indications, intraoperative details (conversion, operative time, estimated blood loss, and transfusion requirements), and short-term outcomes (morbidity, 90-day mortality, and postoperative hospital stay). Postoperative pancreatic fistula (POPF) was classified in accordance with the criteria of the International Study Group on Pancreatic Fistula (ISGPF), 7 whereas the 2016 update version recommended grade A fistula as “biochemical leak”, and grade B and C as “clinically relevant pancreatic fistula (CR-POPF)”. 8 The severity of postoperative complications was based on the Clavien-Dindo classification. 9 Among them, major complications consist of Grades III, IV, and V, while minors include Grades I and II. Within 90 days of the primary procedure related to the pancreatic resection, any unintended admission or operation can be referred to as a readmission or reoperation.
Operating procedures
Patient selection and choice of procedure were at the discretion of each surgeon. The surgical procedures were standardized, with all surgeons having received similar training. The details of various procedures were described previously.3,5,6,10–13 In brief, the supine position was required in the placement of the patient, where the head was slightly elevated. In addition, two 12-mm trocars and three 5-mm ones were utilized, all of which were placed in a shape “V.” Pneumoperitoneum was established at a pressure of 13–15 mm Hg. For malignancies, only DPS and PD were performed. Intraoperative ultrasonography was used to guide the EN if necessary. For distal pancreatectomy, the performance of dissection was carried out mainly in a right-to-left manner. And the choice of splenectomy is primarily determined by tumor factors, such as location, pattern, size, and malignancy. In general, SPDP can be intraoperatively performed in precedence to spleen preservation under the circumstance of smaller-than-5 cm, single and benign, or low-grade malignant pancreatic lesion in the absence of splenic vessels and hilus involvement. There were two techniques of SPDP. Conventional splenic vessel preservation that preserves the main splenic artery and vein, also known as Kimura's technique, was the most common used method. Warshaw technique was only conducted when it was impossible to dissect the pancreas from the splenic vessels. The initial attempt of CP was undertaken in April 2011, in the hope of retaining more pancreatic parenchyma once a low-grade or benign tumor was found at the pancreatic neck. Then an end-to-side pancreaticojejunostomy (PJ) was conducted as long as a diameter of 2 mm at most was attained at the pancreatic duct, despite the difficulty in identification, while the duct-to-mucosa PJ could be utilized in the case of the pancreatic duct with a diameter of over 2 mm. The PD was applied since September 2012 when surgeon gained sufficient experience. The protocol for PD was similar to open surgery and Child's approach was used for the reconstruction with principle of PJ just like CP. Total pancreatectomy was only used for multiple malignancies which were impossible merely using DPS or PD to remove tumors. All specimen and its margins were routinely sent for intraoperative frozen section examination. One or two drainage tubes were left close to pancreatic remnant surface, hepaticojejunostomy (HJ), and PJ.
Drainage tubes were routinely removed on postoperative day 3 for DP and EN, whereas postoperative day 5 for CP and PD, when amylase of drain fluid was less than three times the upper normal serum value. In patients with any measurable volume of drain fluid rich in amylase (>3 times the upper normal serum value), drainage tubes were kept in place and removed individually, depending on the enzyme levels.
Results
Patient demographics
From June 2004 to June 2018, a total of 605 laparoscopic pancreatic resections were performed in our center, including 237 (39.2%) DPSs, 116 (19.2%) SPDPs, 30 (5.0%) ENs, 30 (5.0%) CPs, 186 (30.7%) PDs, and 6 (1.0%) PDTPs. We divided the period into three stages: early stage (2004.6–2008.12), middle stage (2009.1–2013.12), and late stage (2014.1–2018.6). It can be seen from the Figure 1 that only DPS, SPDP, and a small amount of EN were carried out at the earliest stage. After intracorporeal hand-sewn technique maturity, we started CP in April 2011 and PD in September 2012. In the last period, the number of LP, especially PD, increased sharply. All 6 cases of PDTP were performed in late stage. Detailed demographic and pathological characteristics for our patient cohort are shown in Table 1. The mean age of the patients (257 men and 348 women) was 55.6 years. The mean body mass index (BMI) was 22.7 kg/m2. The median American Society of Anesthesiologist (ASA) score was 2. The most common comorbidity was hypertension. Among different procedures, patients who received SPDP and EN were younger and had high proportion of females and low proportion of comorbidity (Table 1).
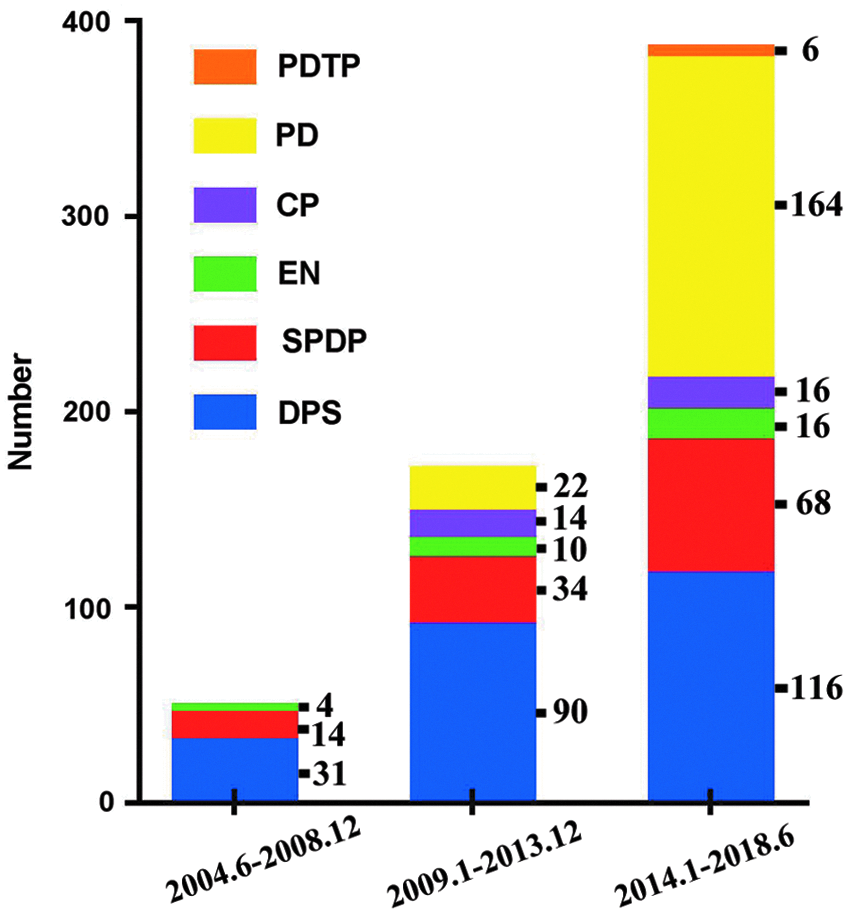
The number of various laparoscopic pancreatectomies for pancreatic and periampullary diseases in three stages.
Clinicopathological Characteristics
Nine (7.4%) of 122 patients had more than two comorbidities.
BMI, body mass index; DPS, distal pancreatectomy with splenectomy; SPDP, spleen-preserving distal pancreatectomy; EN, enucleation; CP, central pancreatectomy; PD, pancreatoduodenectomy; PDTP, pancreatoduodenectomy with total pancreatectomy.
Pathologic examinations showed PDAC in 146 (24.1%) patients, serous cystadenoma (SCA) in 71 (11.7%) patients, mucinous cystadenoma (MCA) in 73(12.1%) patients, intraductal papillary mucinous neoplasm (IPMN) in 49 (8.1%) patients, solid pseudopapillary tumor (SPT) in 49 (8.1%) patients, neuroendocrine neoplasm (NEN) in 73(12.1%) patients, pancreatic cyst in 42 (6.9%) patients, ampulloma in 49 (8.1%) patients, biliary adenocarcinoma in 20 (3.3%) patients, duodenal adenocarcinoma in 8 (1.3%) patients, duodenal gastrointestinal stromal tumor (GIST) in 7 (1.2%) patients, chronic pancreatitis in 11 (1.8%) patients, and others in 7 (1.2%) patients. Among these, PDAC patients only received DPS, PD, or TP. All ampulloma, biliary adenocarcinoma, duodenal adenocarcinoma, and GIST patients underwent PD. SPDP, EN, and CP were only used for benign or low-grade tumors like SCA, MCA, SPT, cyst, and benign IPMN or NEN.
Intraoperative effects
Operative findings are listed in Table 2. Surgery lasted a mean of 241.5 ± 105.5 minutes (range: 50–550 minutes) for the entire population. It was longer for resections with a reconstruction phase (CP, 266.0 ± 47.6 minutes, range: 180–340 minutes; PD, 367.1 ± 61.8 minutes, range: 230–550 minutes) or complicated resection (PDTP, 435.0 ± 69.2 minutes, range: 370–540 minutes). Mean blood loss was 219.8 ± 138.2 mL (range: 20–900 mL) for the entire population and 293.2 ± 156.3 mL (range 120–900 mL) for PD.
Operative Factors
Twenty-two (3.6%) of all patients underwent conversion to laparotomy, which mainly concentrated on DPS and PD. Reasons were as follows: severe adhesion caused from historical abdominal surgery or inflammation of chronic pancreatitis (n = 5); intraoperative uncontrollable bleeding from branches of major vessels like superior mesenteric artery, gastroduodenal artery, splenic artery, and portal vein (n = 7); difficulty in exposing lesions of huge duodenal GIST (n = 2); suspicious vascular invasion to achieve safe margin (n = 7); and acidosis due to long time pneumoperitoneum (n = 1).
Postoperative outcomes
Postoperative complications classified by the Clavien-Dindo schema are presented in Table 3. POPF was confined to CR-POPF according to the recommendation of the 2016 update ISGPF version. 8 The most common complication was POPF (n = 75, 12.4%), with a high incidence after CP (n = 7, 23.3%) and a relatively low incidence after DPS (n = 26, 11.0%), SPDP (n = 10, 8.6%), EN (n = 2, 6.7%), and PD (n = 30, 16.1%). Delayed gastric emptying (23 of 605, 3.8%) was observed mostly after PD (n = 18, 9.7%), as was hemorrhage (overall incidence, n = 34, 5.6%; for PD, n = 21, 11.3%). Bile leak was only observed in PD (9 of 186, 4.8%). For PDTP, three patients suffered severe glucose variability, but no other complications were observed in this cohort. Ninety-day mortality was observed only in the cohort of patients undergoing PD (n = 4). The mean hospital stay was 13.4 ± 10.1 days (range 3–92 days) for the entire cohort. It was longer in CP (15.8 ± 9.0 days, range 7–39 days) and PD (19.5 ± 13.6 days, range 6–92 days).
Postoperative Complications and Recovery
CR-POPF, clinically relevant pancreatic fistula.
Discussion
With procedures that are difficult and take a long time to be accepted, particularly in specific units, laparoscopic pancreatic resections demand a high degree of specialty. The first laparoscopic DPS in our cohort was performed in 2003, while the first laparoscopic SPDP was also approached in later 2003.3,4 Initially, only distal pancreatectomies were selectively attempted intracorporeally since LPs were still considered an innovative technique. As years passed and experience accumulated, skepticism ultimately turned into enthusiasm and more cases were considered eligible for laparoscopy. Now, LDP was routinely performed for neoplasms located on left side pancreas.
At the same time, years of establishment of the parenchyma-sparing principle have made it possible to approach the lesions in the proximal body of pancreas or the pancreatic neck by means of more conservative resections instead of major resections, which will yield better postoperative results. The treating benign or borderline pancreatic tumor located in these areas is a tough issue. 5 Both PD and DP would increase the risk of postoperative pancreatic deficiency and the complicated gastrointestinal reconstruction inevitably harm the long-term health-related quality of life. 14 Meanwhile, the latest development in imaging technology and people's growing awareness of their physical health have led to the increasing incidence of borderline malignant and benign pancreatic tumors. 15 As a result, patients now have access to metabolic function-preserving or parenchyma-sparing technologies, such as CP and EN, which can not only reduce the risks of exocrine insufficiency of the pancreas and diabetes but also ensure that a larger part of the normal pancreatic parenchyma can be preserved.16,17
EN is recommended to be the standard method to treat endocrine tumors. 18 There are also other indicators, such as benign conditions, SPTs, and serous and mucinous cystadenoma. 18 However, in our institution, EN is not adopted for IPMNs, mainly due to the latter's lack of a distinct negative resection margin and the risk of malignancy. In addition, it is believed that, compared with EN, standard resections can lead to a superior disease-free postoperative course. Importantly, EN is only recommended for benign endocrine neoplasms, while these when diagnosed as malignancy at histopathological examination, re-standard operation with lymphadenectomy should be replenished. 18 The main problem after EN remains the high incidence of pancreatic fistula, with reported rates ranging 13%–26% for laparoscopic surgery,2,17,18 which was comparable to the rate of 20.0% in this series. Reduced operative time compared to open EN is one of the advantages of LEN, which was demonstrated in previous studies.11,19,20 This could be mainly due to the simple steps of EN, and quick management of trocar incision could save time in contrast to incision management in open surgery. Because laparoscopic surgery lacks manual palpation, laparotomy was reported to seek the neoplasms. 21 In our center, intraoperative ultrasonography was used to guide the EN if necessary.
The benefits of CP can be seen from its ability to not only eliminate the risks of hematologic disorders and postsplenectomy sepsis but also keep a larger part of the normal pancreatic tissue, thus making it a viable choice of treatment when it comes to the borderline or benign lesions in the neck of pancreas, despite its inability to realize EN.22,23 However, whether CP experiences similar operative risk to that of conventional pancreatectomy is controversial, which is mainly because of the high POPF rates, as it generates two cut surfaces following segmental resection. The clinically significant pancreatic fistulas (grades B and C, defined as CR-POPF in the 2016 update ISGPF version) in our study were 23.3%. This is comparable to other studies of LCP, which have reported POPF rates in the range of 33.3%–69.0%.2,24–26 Cohort studies also demonstrated that LCP had comparable rates of clinically relevant POPF in relation to open surgery.12,16 However, POPF after DP and PD, including this study, is well below that of CP. 27 However, the severe complications, reoperation, and mortality of CP were reported not inferior to that of DP. 28 Furthermore, the biggest merit of CP lies in its ability to keep a larger part of the normal pancreatic tissue, which ensures that the long-term endocrine and exocrine functions of patients can be preserved. Considering the fact that pancreatic islets are mostly located in the end section of the pancreas, it is believed that, compared with the highly destructive PD and DP that are likely to affect the pancreas' endocrine function, CP, although with its slow-recovery process and POPF risks, is still the best option for young patients who have low-grade and benign tumors for they could expect a long life ahead.
PD is one of the most complex procedures in abdominal surgery. The number of this procedure has been increasing in recent years, thanks to improved diagnostic capabilities, expanding indications, and the formal development of pancreatic surgery training. However, the progress in the LPD technology has been quite slow, for its procedure is much too complex, restricting its practitioners to merely veteran surgeons in referral centers. In contrast, the development of LDP is rapid, due to its low technical requirements and reconstruction-free procedure. We began performing LPD in September 2012, when we believed our team had already got enough experience obtained from other laparoscopic abdominal surgeries. That was almost 8 years after we initially attempted LDP. The technical difficulty of lymphadenectomy for perigastric and peripancreatic lymph nodes and en bloc resection of specimen is one of the major obstacles to obtain LPD for malignancy. The stomach and pancreas are upper abdominal organs with closely related anatomical structure and lymph node distribution. We performed laparoscopic radical gastrectomy for gastric cancer as early as October 2004.29–31 As mentioned above, the experience also obtained from LDP with or without spleen-preserving for various pancreatic neoplasms.3,13 Worrying about the safety of intracorporeal anastomosis is another obstacle of LPD. We believe intracorporeal hand-sewn technique is crucial and learning curve of PJ, HJ, and gastrojejunostomy (GJ) should be completed, respectively, before combined using for LPD. Our initial experience of intracorporeal PJ gained from LCP, 5 and the HJ and GJ obtained from laparoscopic choledochotomy 32 and totally laparoscopic distal gastrectomy.30,33 Meanwhile, intracorporeal hand-sewn technique was obtained from esophagojejunostomy after laparoscopic total gastrectomy.33,34 The main indications of LPD in this series were adenocarcinomas (73.7%): PDAC (32.3%), ampulloma (26.3%), distal third common bile duct adenocarcinoma (10.8%), and duodenal adenocarcinoma, excepting ampullary location (4.3%). The median operative time was 365 minutes and mean blood loss was 240 mL, which were comparable to the reported operative time range from 340 to 510 minutes and blood loss range from 250 to 590 mL.2,35–39
TP is an aggressive approach that needs to be carefully considered in view of complete loss of pancreatic exocrine and endocrine function. IPMN is now well recognized as a benign or premalignant lesion, but due to the potentially widespread nature, partial pancreatectomy is selected unless negative resection margin of intraoperative frozen-section biopsy is achieved. Three cases of IPMN were forced to conduct TP due to diffuse type in this study. Considered the favorable prognosis, spleen-preserving procedures were used to maintain the immunological functions in these three cases, two conservation of the splenic artery and vein (Kimura's technique) and one segmental resection of both splenic vessels (Warshaw's technique). Interestingly, the indication for another three TPs was multiple or unfavorable location PDAC. For such aggressive malignancy, resection of splenic vessels with splenectomy was recommended.
Conclusions
In conclusion, we report here our experience during the 15 years with 605 laparoscopic pancreatic resections. As long as the circumstances meet the demands, the methods to reproduce the laparoscopic pancreatic surgery can be demonstrated by means of its evolution discussed above. In comparison, the results of laparoscopic pancreatic resection that involves reconstruction, especially PD, are relatively undesirable. Further research to evaluating comparative effectiveness with open surgery is required.
Footnotes
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.