
Abstract
Abstract
Background:
Laparoscopic distal pancreatectomy with splenectomy is the standard procedure for body and tail pancreatic tumors. Technical difficulties arising from the strict anatomical relationship between pancreas and splenic vessels generally impose a concomitant splenectomy. Previous retrospective studies have shown a reduced risk of postoperative complications and infections in spleen preserved patients, but this is still a debated issue. Aim of this systematic review and meta-analysis was to provide a more robust evidence on the effect of spleen preserving laparoscopic distal pancreatectomy.
Methods:
PubMed, MEDLINE, Embase, and Cochrane databases were consulted. Pooled effect measures were calculated using an inverse-variance weighted or Mantel–Haenszel in random effects meta-analysis. Heterogeneity was evaluated using I2-index and Cochran Q-test.
Results:
Ten observational studies were eligible, and 632 patients were included in the quantitative analysis. Overall, 296 (46.8%) patients underwent laparoscopic distal pancreatectomy with splenectomy (Group S), and 336 (53.2%) patients underwent spleen-preserving laparoscopic distal pancreatectomy (Group SP). In-hospital mortality was 0%. In the group S, the estimated pooled odds ratio of postoperative surgical site infection (SSI) and overall complications was 1.51 (95% confidence interval [CI]: 1.01–2.28; P = .048) and 2.30 (95% CI: 1.11–4.76; P = .024). The estimated pooled odds ratio of pancreatic fistula, postoperative bleeding, and reoperation was 1.64 (P = .094), 1.01 (P = .987), and 1.24 (P = .776), respectively.
Conclusions:
Spleen-preserving laparoscopic distal pancreatectomy may reduce postoperative SSI and overall complications. These results should be interpreted with caution but seem meaningful to establish a better evidence-based treatment for distal pancreatic tumors. Further studies are warranted to analyze the role of spleen preserving laparoscopic distal pancreatectomy on long-term outcomes.
Introduction
O
Splenectomized patients have also a lifetime risk of developing infectious complications and overwhelming postsplenectomy infection (OPSI). 6 Despite the intrinsic technical difficulties, spleen-preserving laparoscopic distal pancreatectomy has the potential to reduce the incidence of postoperative infectious complications and overall morbidity. 7
The aim of this systematic review and meta-analysis was to analyze perioperative outcomes of laparoscopic distal pancreatectomy with spleen preservation (Group SP) versus laparoscopic distal pancreatectomy with splenectomy (Group S).
Materials and Methods
The study was conducted according to the Preferred Reporting Items For Systematic Reviews and Meta-analyses (PRISMA) statement. We reviewed the literature between 2008 and June 2018 using PubMed, MEDLINE, Embase, and Cochrane databases to identify studies comparing laparoscopic distal pancreatectomy with or without splenectomy.
The search terms used were “laparoscopic distal pancreatectomy,” “splenectomy,” “spleen preservation,” and “spleen preserving.” The reference lists of all articles were consulted for additional studies. All articles comparing laparoscopic distal pancreatectomy with or without splenectomy and having a sample size ≥15 were included in the systematic review. Two authors (A.A., P.M.) independently extracted data from eligible studies. Data extracted included study characteristics (first author name, year, and journal of publication), number of patients included in the series, time frame, clinical and demographic characteristics of the patient population, type of surgical procedure (Warshaw's technique versus spleen vessel preservation technique), and postoperative outcomes. Disagreements between authors were solved by consensus; if no agreement could be reached, a third senior author (L.B.) made the decision.
Studied outcomes were the following: operative time, operative blood loss and number of patients requiring blood transfusions, overall complications, number of patients with pancreatic fistula defined according to International Study Group of Pancreatic Fistula, 8 surgical site infections (SSIs), postoperative length of stay, and 30-day mortality. SSI was defined as the development of superficial, deep, or organ/space SSI until patient discharge. All patients underwent preoperative antibiotic prophylaxis.
Two investigators independently assessed the methodological quality of the articles using the Newcastle–Ottawa Scale (NOS). 9 Each study is judged on a “star system” based on the selection of the study groups and the ascertainment of outcome of interest. Each study could earn a maximum of nine stars. Studies with low quality score (NOS <6) were excluded. The study protocol was registered at PROSPERO (International prospective register of systematic reviews), accessible at www.crd.york.ac.uk/prospero (Registration number: CRD42018108313).
Statistical analysis
The results of the systematic review were summarized qualitatively into Frequentist random effect meta-analysis of pooled odds ratio and raw mean difference. Inverse-variance method and DerSimonian–Laird estimator for variance of true effect size (τ2) were performed. 10 Heterogeneity among the studies was evaluated by I 2 -index and Cochran Q-test. 11 Statistical heterogeneity was considered significant when P < .10 or I 2 -index was >50%. 12 Wald type 95% confidence interval (CI) was computed for pooled measure, otherwise 95% CI for I 2 -index was calculated according to Higgins and Thompson. 13 In addition, meta-regression was performed to investigate heterogeneity. Prediction interval for treatment effect of a new study is calculated according to Borestein. 11 Mean and variance for continuous outcomes were estimated from range according to Hozo et al., 14 as appropriate. As sample size is not the same in all studies, we performed a sensitivity analysis by excluding one study each time and rerunning the analysis to verify the robustness of the overall results. Z-score test was performed. Two-sided P value was considered statistically significant when <.05. All analyses and figures were carried out using R version 3.2.2 software. 15
Results
Systematic review
Ten eligible studies published between 2008 and 2017 were included in the systematic review and meta-analysis (Fig. 1). The studies included a total of 632 patients: n = 296 (46.8%) in the S group and n = 336 (53.2%) in the SP group. Sample size of each study varied from 23 to 206 patients. Every study earned a NOS score of 6 or 7 (median 6.6), suggesting a good quality level. Studies included purely retrospective reviews (n = 9) and one retrospective review of prospectively maintained data (n = 1). There were no randomized controlled trials comparing the two surgical procedures.
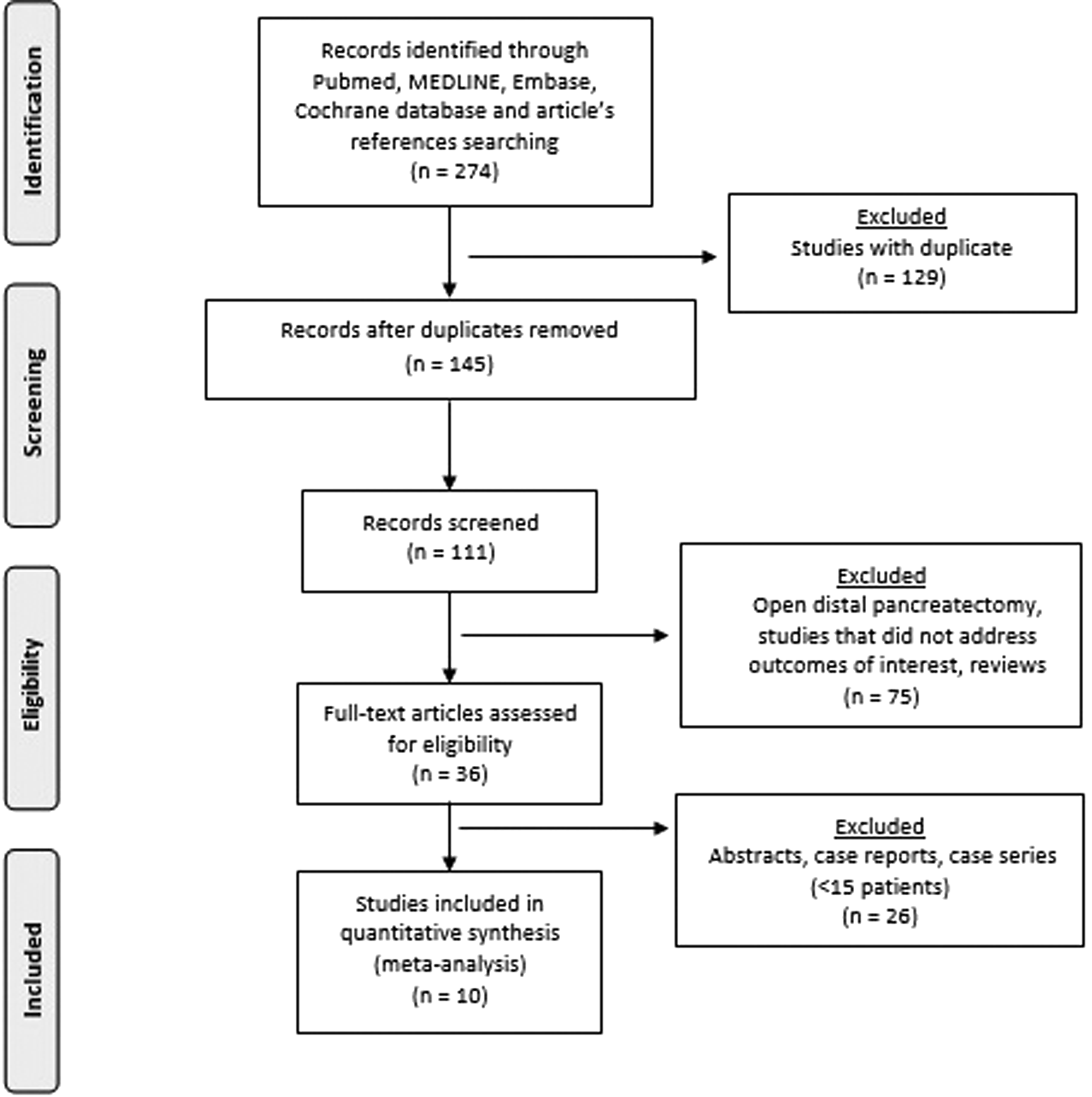
PRISMA diagram. PRISMA, Preferred Reporting Items For Systematic Reviews and Meta-analyses.
Demographic, clinical, and operative data of the patient sample are summarized in Table 1. Patients' age ranged from 43 to 64.5, and the majority was females (63.9%). The mean body mass index (BMI) reported by half of the studies was 25.1 kg/m 2 . Indications to treatment were different among the studies: the diagnosis of pancreatic adenocarcinoma was mentioned only in three studies,16,22,23 for a total of 27 patients (4.3%). Nine studies described the surgical technique for spleen preservation: four studies performed the Warshaw's technique, three studies the spleen vessel preservation technique, and two studies both. Conversion to an open procedure was reported in 25 patients (3.9%), 22 in group S and 3 in group SP.
BMI, body mass index; NA, not applicable; NR, not reported; S, splenectomy group; SP, spleen preserving group; SVP, spleen vessel preservation; WT, Warshaw's Technique.
The mean total procedure time was 199.7 minutes (range 90–310 minutes); for group S it was 185.2 minutes (70–304 minutes), and for group SP it was 214.2 minutes (85–310 minutes). Overall, 50 patients required blood transfusion, 28 (56%) in group S and 22 (44%) in group SP. Reoperation rate ranged from 0.8% to 14.3% in group S and from 2.5% to 16.7% in the group SP. Hospital length of stay ranged from 2 to 28 days in group S and from 3 to 22 days in group SP. In-hospital mortality was 0%.
Meta-analysis
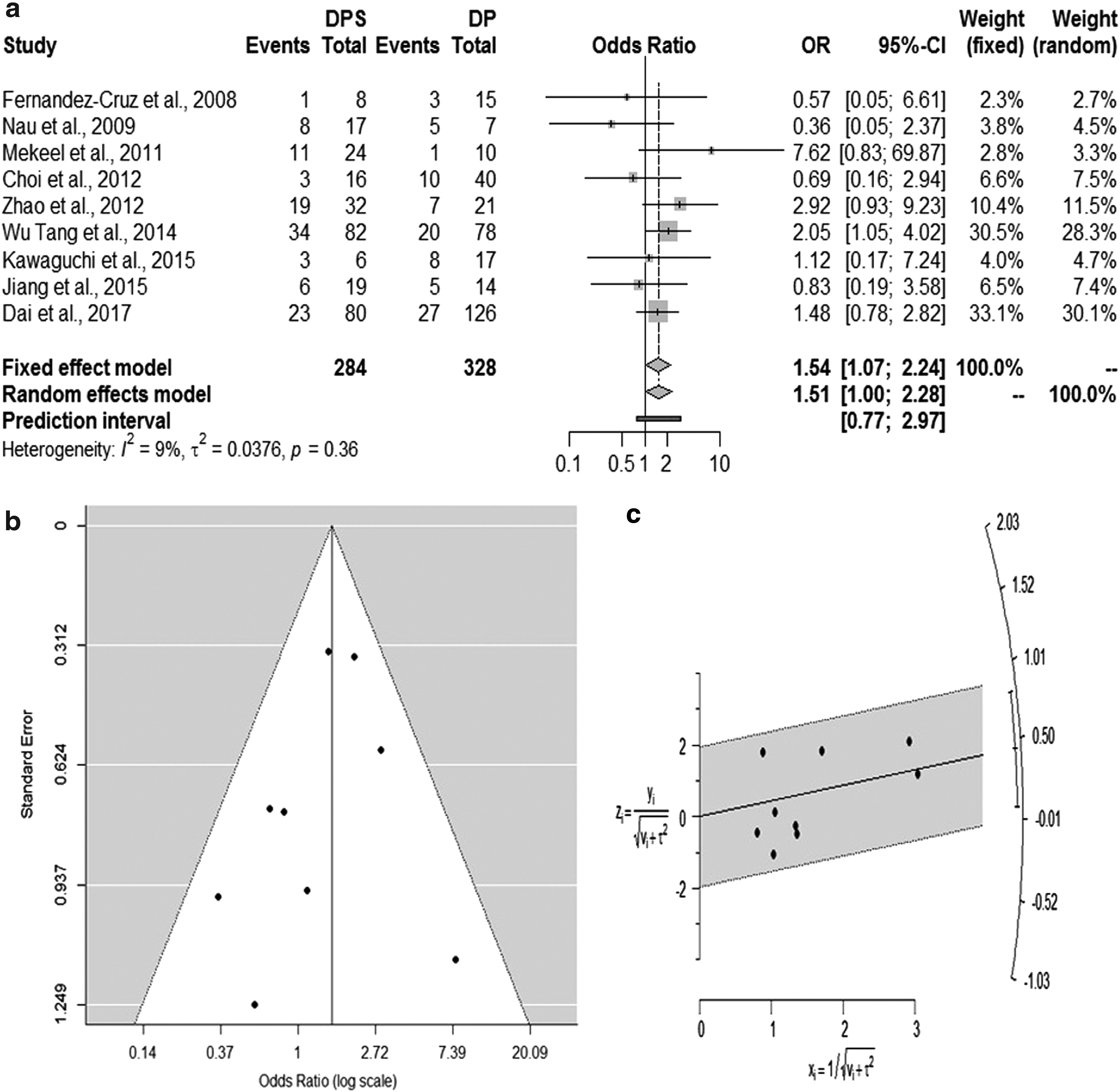
In addition to a systematic review, we performed a Frequentist meta-analysis. Considering random effect model, the estimated pooled odds ratio of overall complications, resulting from nine studies, which include a total of 612 patients, is 1.51 (95% CI: 1.01–2.28; P = .048). The prediction lower and upper limits are 0.77 and 2.97, respectively. The heterogeneity is not significant (I 2 = 9.2%, 95% CI: 0.0–68.0; P = .359) and τ2 = 0.04. Funnel plot shows do not show publication bias effect according to Egger test (P = .239). The adjusted Trim and Fill odds ratio is 1.66 (95% CI: 1.07–2.59) (Fig. 2). The sensitivity analysis yields a risk ratio estimation of 1.54 (95% CI: 1.07–2.23). The Galbraith plot confirmed the low heterogeneity level.
Forest
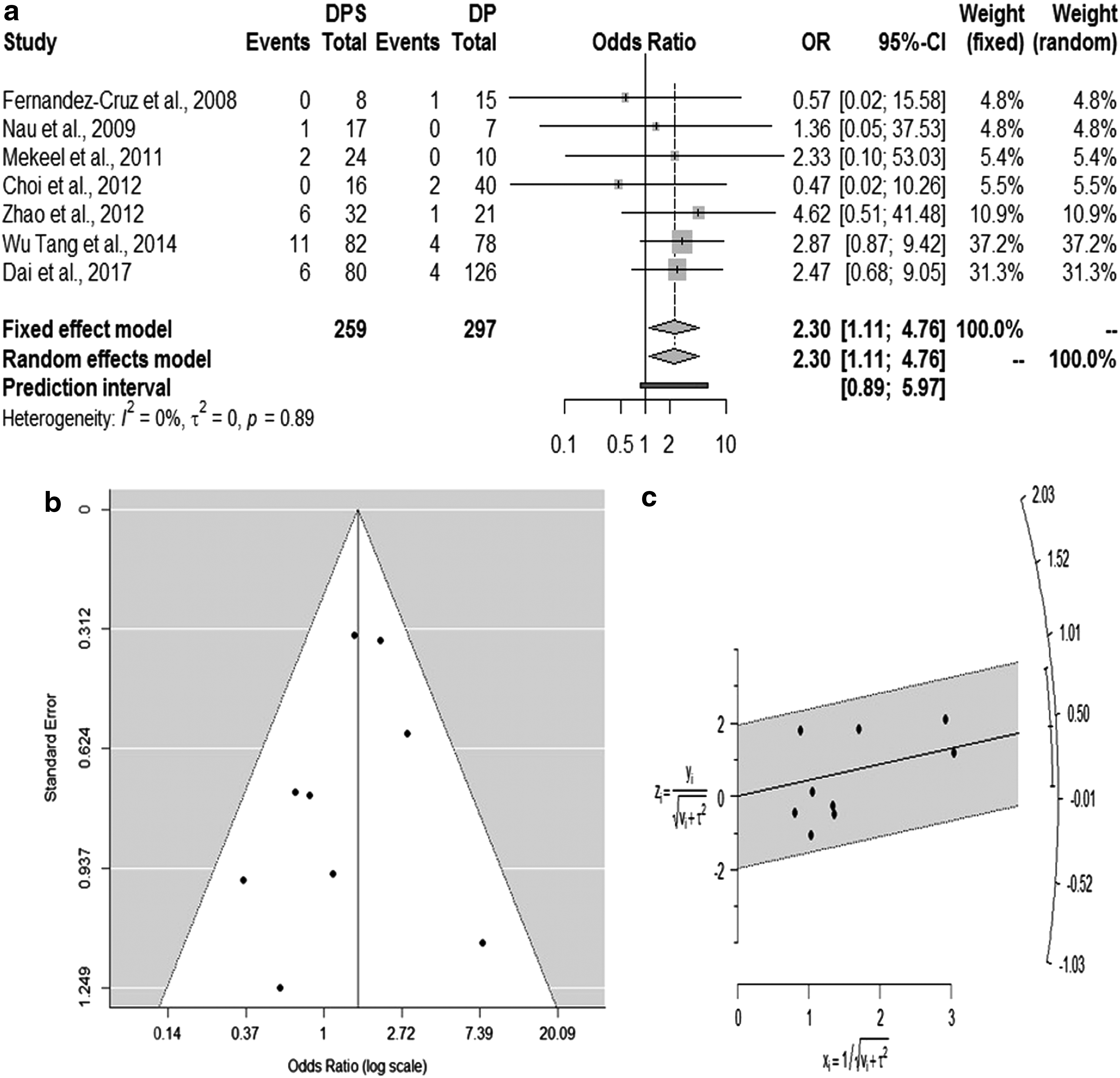
Considering random effect model, the estimated pooled odds ratio of SSIs, resulting from seven studies, which include a total of 556 patients, is 2.30 (95% CI: 1.11–4.76; P = .024). The prediction lower and upper limits are 0.87 and 5.97, respectively. The heterogeneity is zero (I 2 = 0.0%, 95% CI: 0.0–24.9; P = .887) and τ2 = 0.00. Funnel plot shows show that publication bias could not be excluded. However, the Egger test do not show evidence of publication bias (P = .269). The adjusted Trim and Fill odds ratio is 2.84 (95% CI: 1.45–5.60) (Fig. 3). The sensitivity analysis yields a risk ratio estimation of 2.31 (95% CI: 1.12–4.69). The Galbraith plot confirmed the low heterogeneity level.
Forest
Considering random effect model, the estimated pooled mean difference for hospital length of stay from nine studies, which include a total of 595 patients, is 0.89 (95% CI: −0.02 to 1.79; P = .055). The prediction lower and upper limits are −1.79 and 3.57, respectively. The heterogeneity is high (I 2 = 80.4%, 95% CI: 63.7–89.5; P < .001). Funnel plot shows do not show publication bias effect according to Egger test (P = .267) (Fig. 4). Meta-regression adjusted for age, BMI, complications, and type of tumor showed that these variables could not influence the hospital length of stay.

Forest
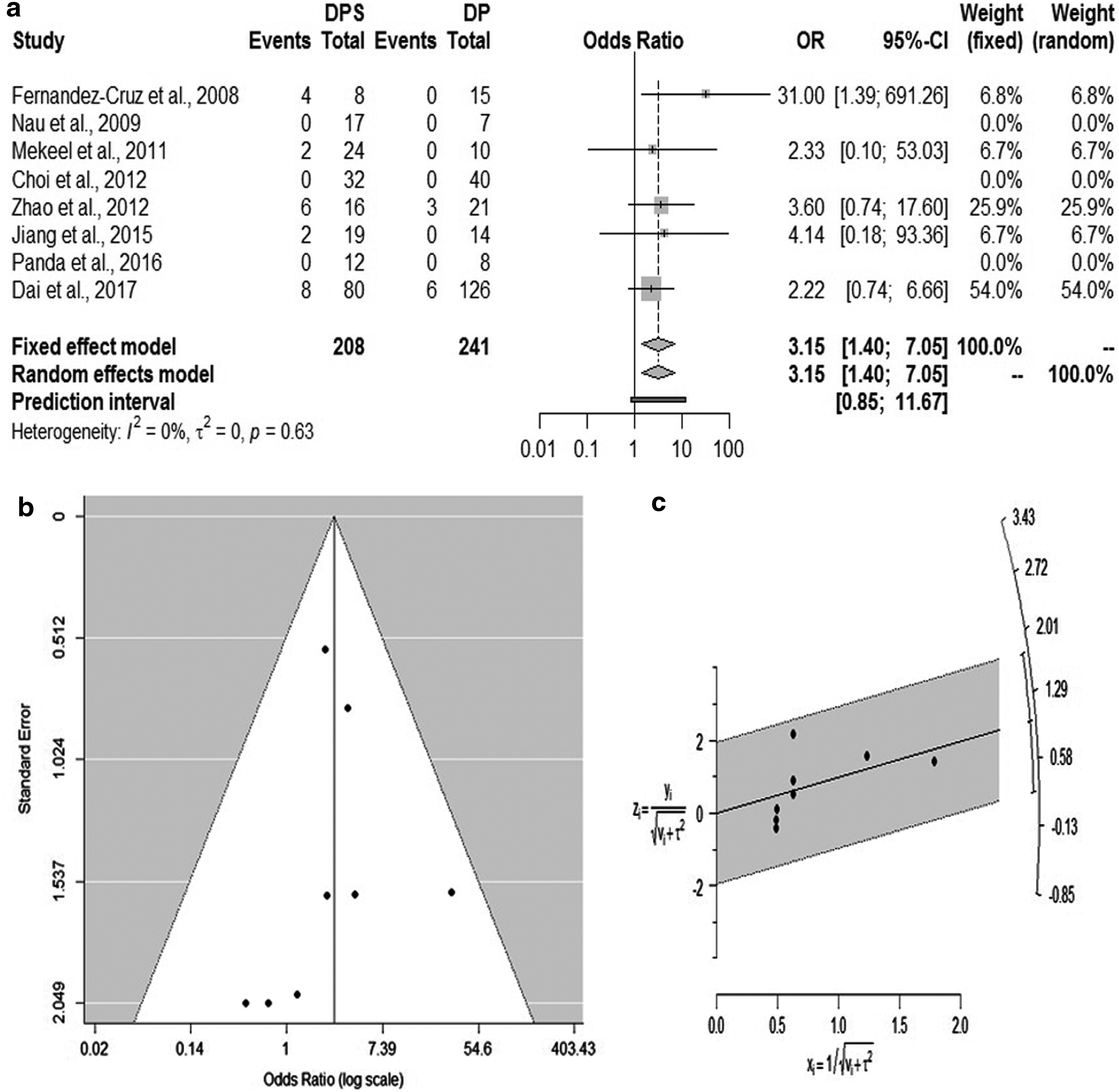
Considering random effect model, the estimated pooled odds ratio of conversion to open procedure, resulting from eight studies, which include a total of 449 patients, is 3.15 (95% CI: 1.40–7.05; P = .005). The prediction lower and upper limits are 0.85 and 11.67, respectively. The heterogeneity is zero (I 2 = 0.0%, 95% CI: 0.0–67.6; P = .633) and τ2 = 0.00. Funnel plot does not show publication bias effect according to Egger test (P = .247). The adjusted Trim and Fill odds ratio is 3.15 (95% CI: 1.40–7.05) (Fig. 5). The sensitivity analysis yields a risk ratio estimation of 3.14 (95% CI: 1.39–7.10). The Galbraith plot confirmed the low heterogeneity level.
Forest
Considering random effect model, the estimated pooled odds ratio of pancreatic fistula, resulting from eight studies, which include a total of 581 patients, is 1.64 (95% CI: 0.92–2.92; P = .094). The prediction lower and upper limits are 0.51 and 5.29, respectively. The heterogeneity is low (I 2 = 21.2%, 95% CI: 0.0–63.3; P = .261) and τ2 = 0.142. Funnel plot shows do not show publication bias effect according to Egger test (P = .312). The adjusted Trim and Fill odds ratio is 1.76 (95% CI: 0.95–3.12) (Fig. 6). The sensitivity analysis yields a risk ratio estimation of 1.74 (95% CI: 0.98–2.81). The Galbraith plot confirmed the low heterogeneity level.
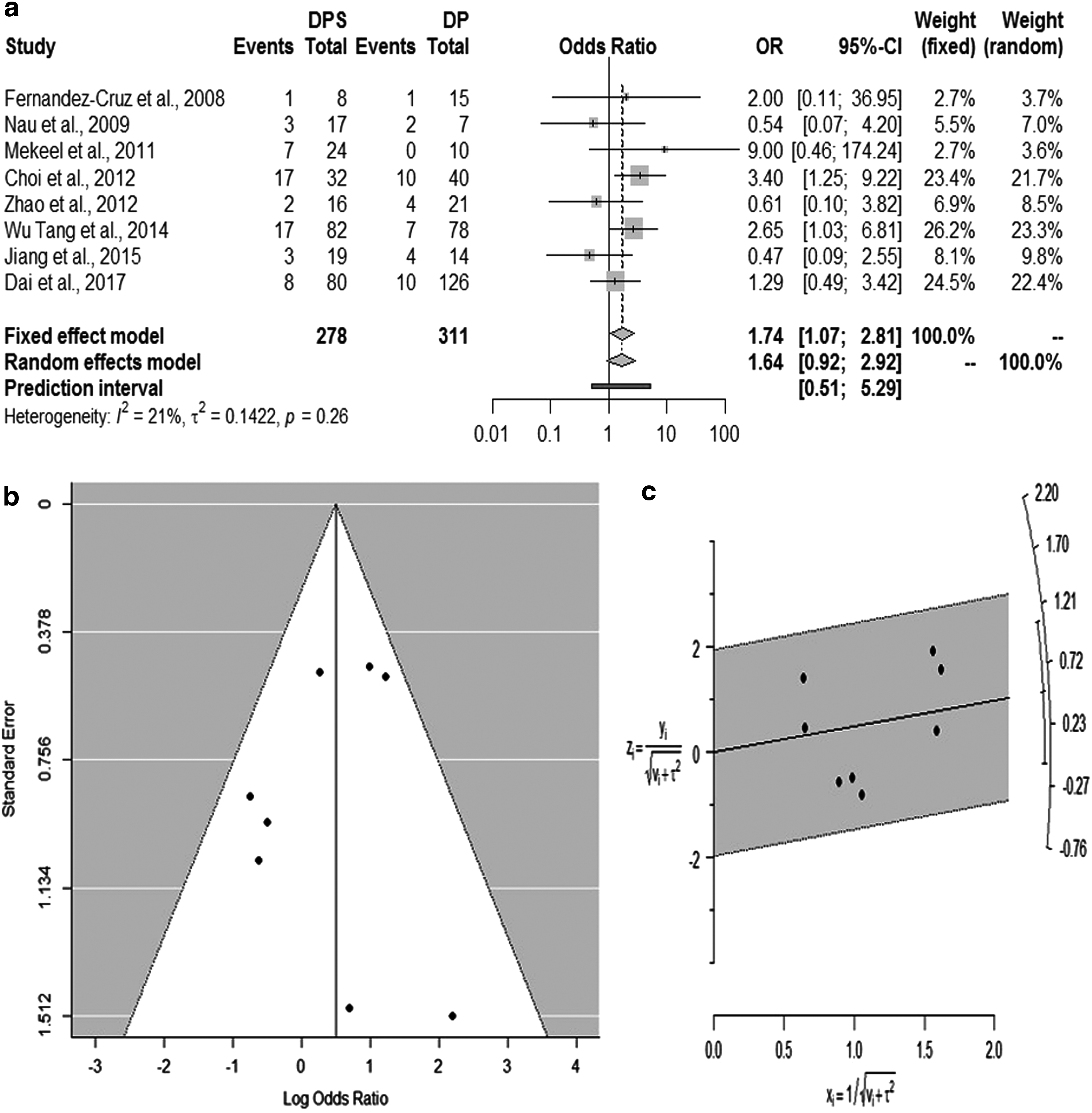
Forest
Considering random effect model, the estimated pooled odds ratio of postoperative bleeding, resulting from five studies, which include a total of 498 patients, is 1.01 (95% CI: 0.43–2.37; P = .987). The prediction lower and upper limits are 0.25 and 4.04, respectively. The heterogeneity is zero (I 2 = 0.0%, 95% CI: 0.0–38.6; P = .852) and τ2 = 0.00. Funnel plot shows do not show publication bias effect according to Egger test (P = .358). The adjusted Trim and Fill odds ratio is 0.98 (95% CI: 0.40–2.30) (Fig. 7). The sensitivity analysis yields a risk ratio estimation of 0.99 (95% CI: 0.42–2.36). The Galbraith plot confirmed the low heterogeneity level.
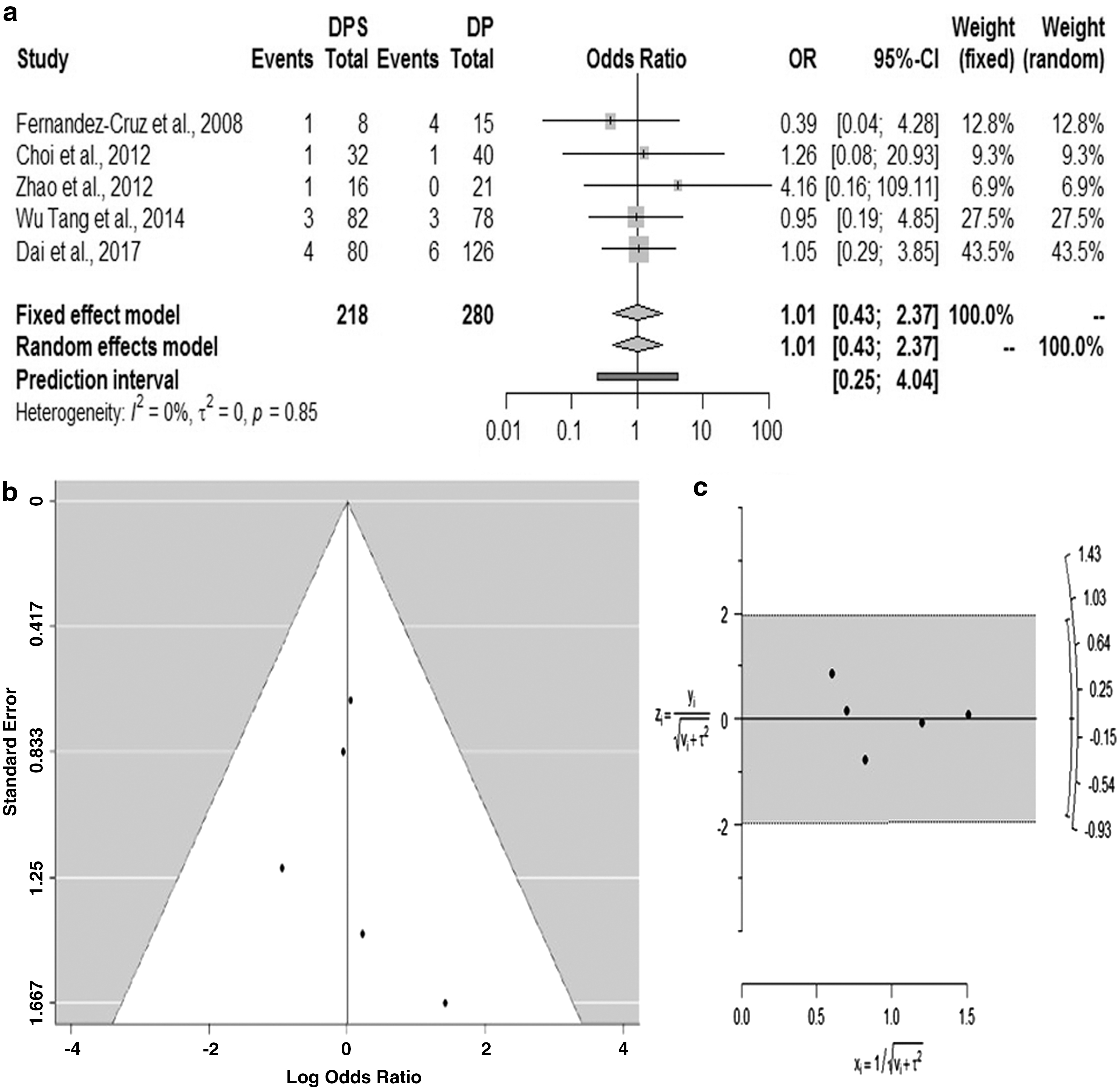
Forest
Considering random effect model, the estimated pooled odds ratio of reoperation, resulting from seven studies, which include a total of 363 patients, is 1.24 (95% CI: 0.29–5.33; P = .776). The prediction lower and upper limits are 0.04 and 38.88, respectively. The heterogeneity is low (I 2 = 3.8%, 95% CI: 0.0–85.3; P = .374) and τ2 = 0.086. Funnel plot shows do not show publication bias. The Egger test is significant showing that publication bias could not be excluded (P = .01). The adjusted Trim and Fill odds ratio is 1.86 (95% CI: 0.41–8.42) and confirms that publication and small study bias could not be excluded (Fig. 8). The sensitivity analysis yields a risk ratio estimation of 1.22 (95% CI: 0.26–5.30). The Galbraith plot confirmed the low heterogeneity level.
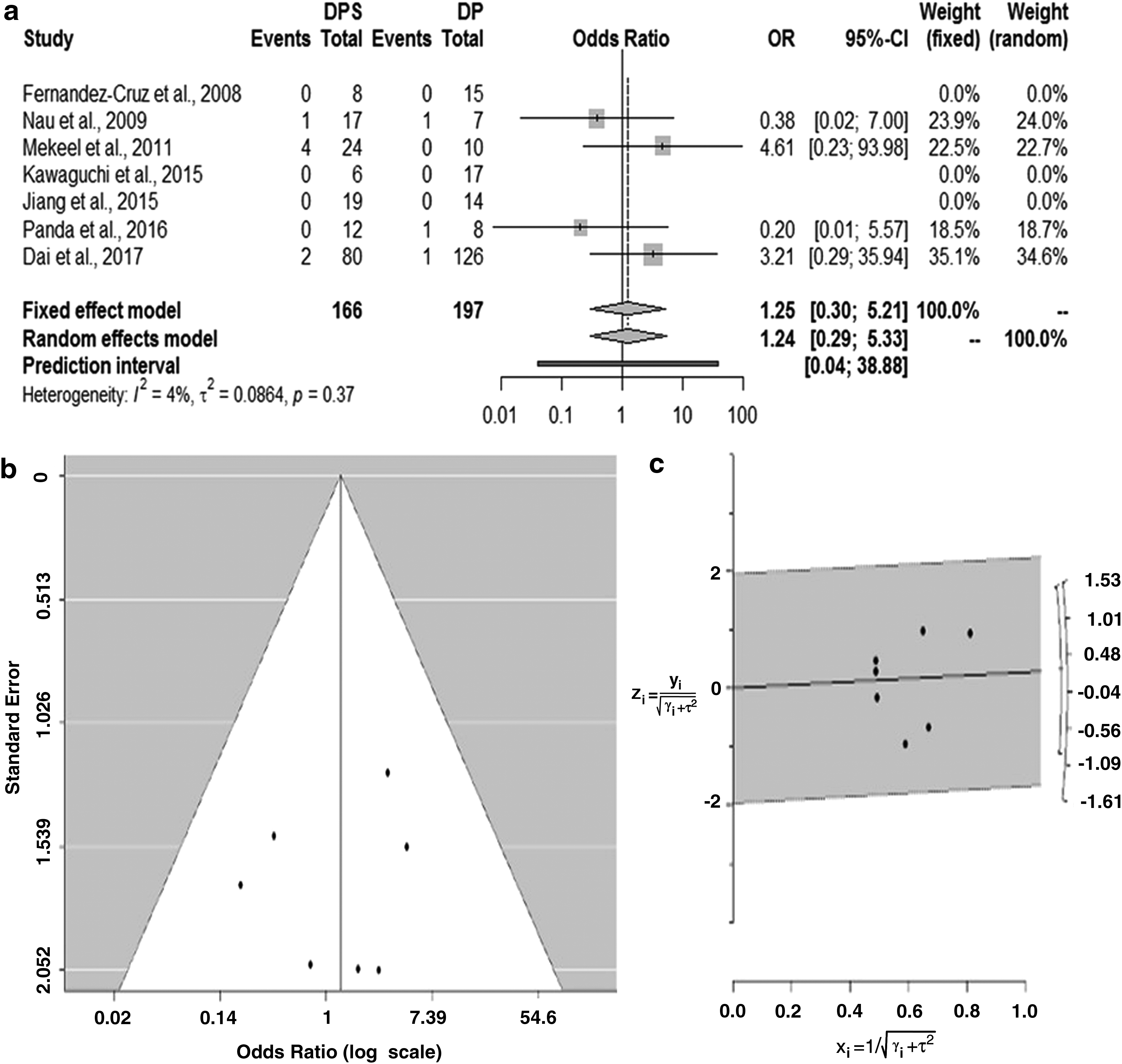
Forest
Discussion
The results of this meta-analysis suggest that patients undergoing laparoscopic distal pancreatectomy with spleen preservation have significantly lower risk of overall complications and SSI rate. The heterogeneity was low, ranging from 0% to 9.2%. These results suggest that the reduced rates of overall complications and SSIs in the immediate postoperative period in the spleen-preserving group may be attributed to preservation of the splenic immune function. This effect is likely to manifest not only in the immediate postoperative period but also probably in the long-term follow-up. It has been shown that the estimated lifetime risk of OPSI is ∼5% and the related mortality 50% in a population with low incidence of immunized subjects. 26 Interestingly, in the study by Choi et al., 19 the incidence of common cold or flu was significantly more frequent (P = .026) in the splenectomy group, but no data are reported regarding vaccination nor immunization. The other studies included in the meta-analysis do not report sufficient data about long-term follow-up, in particular about OPSI. Therefore, although avoiding splenectomy can be technically more demanding, there is probably an advantage in splenic preservation, both in the short- and long-term follow-up.
The pooled conversion rate to an open procedure was significantly higher in Group S patients (3.15 with 95% CI: 1.40–7.05), and the heterogeneity was zero. This could be related to the need of urgent laparotomy in case of ongoing bleeding and challenging vascular anatomy. In addition, surgeons could be less confident in performing spleen preserving laparoscopic techniques due to the perceived increased risk of vascular damage and longer operative time.
A higher incidence of postoperative complications could be associated with longer hospital length of stay, higher costs, and use of hospital resources. 27 In our study, the pooled hospital length of stay was similar for the 2 patient groups, but the heterogeneity was high. This could be related to the variability in the selected studies coming from different countries and different indications for distal pancreatectomy. All studies were retrospective, underlying the lack of standardized criteria for hospital discharge and differences in applying the enhanced recovery programs after surgery. 28 In addition, outpatient clinic visits, discharge with drain in place, and hospital readmission rates were not reported. Finally, the rate of postoperative pancreatic stump fistula, postoperative bleeding, and rate of reoperation were similar in both groups.
Lymphadenectomy is mandatory in the treatment of distal pancreatic adenocarcinoma; however, the extension of lymph node dissection has not been defined yet.29,30 Oncologic splenectomy allows complete removal of lymph glands at station 10 and 11, but its effect on the long-term survival is debated. The percentage of patients affected by distal pancreatic adenocarcinoma was 4% in the present series, and the analysis of long-term survival was not possible because data were not analyzed in the included studies.
The results of this study may not be generalizable since the included patients were from all over the world and surgery was carried out both in high-volume and low-volume centers. There were no randomized trials to include in the review, which opens the door for bias in selection of technique or for patient allocation. Since no specific data were reported on patients' comorbidities such as diabetes, no inferences could be done on the patient associated risk of infection. In addition, we focused on short-term outcomes, but further studies are warranted to analyze the role of spleen preserving laparoscopic distal pancreatectomy on long-term survival and OPSI.
Laparoscopic spleen-preserving distal pancreatectomy may reduce postoperative SSI rate and overall complications, which in turn may lead to decreased health care costs and enhanced recovery after surgery. These results should be interpreted with caution but may be useful to establish a better evidence-based treatment for distal pancreatic neoplasm. Further studies are warranted to validate the results of our meta-analysis in the long-term follow-up.
Authors' Contributions
P.M. and A.A. did the literature search. A.A. and L.B. formed the study design. Data collection was done by P.M., A.A., and E.R., and G.B. analyzed the data. P.M., A.A., E.A., and L.B. interpreted the data. P.M., A.A., and L.B. wrote the article. P.M., A.A., and L.B. critically reviewed the article.
Disclaimer
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Disclosure Statement
No competing financial interests exist.