
Abstract
Abstract
Background:
Robot-assisted surgical techniques have been introduced in recent years as an alternative minimally invasive approach for colorectal surgery. In practice, we found that the monopolar electrosurgical scissors had its unique advantages in preservation of the pelvic autonomic nerves. We performed a retrospective review of short-term results between using monopolar electrosurgical scissors and harmonic scalpel in robotic anterior resection (using the da Vinci® Surgical System) in rectal cancer patients.
Method:
Forty-six patients who underwent robotic anterior resection of rectal cancer from June 2016 to January 2018 were retrospectively analyzed and compared. Twenty-two cases underwent resection using monopolar electrosurgical scissors and 24 cases underwent resection using the harmonic scalpel. Patient characteristics, perioperative clinical results, complications, and pathological results were compared between two groups.
Results:
There were not significantly different patient characteristics between the two groups. The mean operative time was lesser in the monopolar electrosurgical scissors group than in the inharmonic scalpel group [95.59 ± 21.44 minutes versus 81.45 ± 13.89 minutes, P < .01]. The mean estimated blood loss was lesser in the monopolar electrosurgical scissors group than in the inharmonic scalpel group [48.64 ± 19.35 mL versus 61.82 ± 24.23 mL, P = .03]. The complication rate was 18.2% in the monopolar electrosurgical scissors group and 16.7% in the harmonic scalpel group (P = .89). The mean time of postoperational urinary catheter was lesser in the monopolar electrosurgical scissors group [3.73 ± 1.16 days versus 4.59 ± 1.71 days, P = .02]. The day to first passing flatus [3.45 ± 0.80 days versus 3.59 ± 1.14 days, P = .67], feeding time [4.50 ± 1.00 days versus 4.05 ± 1.87 days, P = .35], hospital stay [8.18 ± 3.74 days versus 8.68 ± 3.44 days, P = .52], and the mean number of harvested lymph nodes of detection [13.59 ± 1.71 versus 13.77 ± 1.41, P = .67] were comparable between procedures.
Conclusion:
Monopolar electrosurgical scissors were used safely and effectively in robotic anterior resection of rectal cancer (using the da Vinci Surgical System). The use of monopolar electrosurgical scissors has benefits in performing blunt and sharp separation in narrow pelvic and cheaper hospitalization expenses.
Introduction
Nowadays, laparoscopic colorectal surgery has been popularized because it results in decreased postoperative pain, shorter length of hospitalization, and earlier return to normal functioning, and increased demand for laparoscopic surgery from patients. 1 Rectal cancer surgery, which is performed in the narrow pelvic cavity, is a more technically demanding procedure than colon cancer surgery. Despite this, there are intrinsic disadvantages of conventional laparoscopic instruments such as an assistant-dependent unstable camera platform, two-dimensional view, limited dexterity of instruments inside the patient, and fixed instrument tips.2,3 The robotic system was mainly designed to allow precise dissection and movements in deep and narrow space to allow precise movements, careful dissection, and suturing in small confined spaces. 4
Robotic anterior resection of rectal cancer has been popularized and performed because of the benefits of the robotic system. 5 It could not only ensure the safety of operation and radical tumor resection, but also offer better postoperative urological and sexual outcomes. 6 Recently, the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) has been widely equipped in China. Our hospital adopted the robot system for rectal cancer in September 2014.
Harmonic scalpel usage had added more precision and speed in dissecting, homeostasis, and cutting the tissues especially the pelvic peritoneum. 7 Because of precise tissue cutting and coagulation control, it was widely used in laparoscopic surgery for rectal cancer and was also one of the main anatomical tools for robotic surgery. However, with the development of robotic anterior resection of rectal cancer in our hospital, the surgical team found that the monopolar electrosurgical scissors had its unique advantages in operations. We found that monopolar electrosurgical scissors have effects in preservation of the pelvic autonomic nerves. Therefore, this study was designed to evaluate the difference in the short-term outcome after using monopolar electrosurgical scissors or harmonic scalpel in robotic anterior resection for rectal cancer patients.
Methods
Data collections
A retrospective comparative study was carried out in 46 consecutive rectal cancer patients who underwent robotic anterior resection of rectal cancer by 1 surgeon (M.Z.) from June 2016 to January 2018 in the Department of Gastrointestinal Surgery at Shanghai Renji Hospital. Among these patients, 22 patients underwent robotic anterior resection of rectal cancer with monopolar electrosurgical scissors and 24 with harmonic scalpel.
Patients with clinical T4 stage, anemia, distant metastases, significant lateral pelvic nodes, and tumor infiltration into other organ were excluded from this study. Patients older than 75 years with history of previous abdominal surgeries and severe cardiac and pulmonary dysfunction were likewise excluded. The protocol was approved by the medical ethics committee of our hospital, and written informed consent for diagnosis and treatment was obtained from all patients before the procedures.
Preoperative and perioperative clinical results were collected from the database. Preoperative clinical results include the tumor location that was measured by rigid sigmoidoscopy. Perioperative clinical results include day to the first passing flatus, feeding time, time of postoperational urinary catheter stay, hospital stay, and complications. Pathology results included a number of harvested lymph nodes. This study was approved by the Institutional Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine (Approval No. 2018027).
Operative techniques
All patients underwent mechanical bowel preparation (polyethylene glycol and electrolyte powder) the day before surgery.
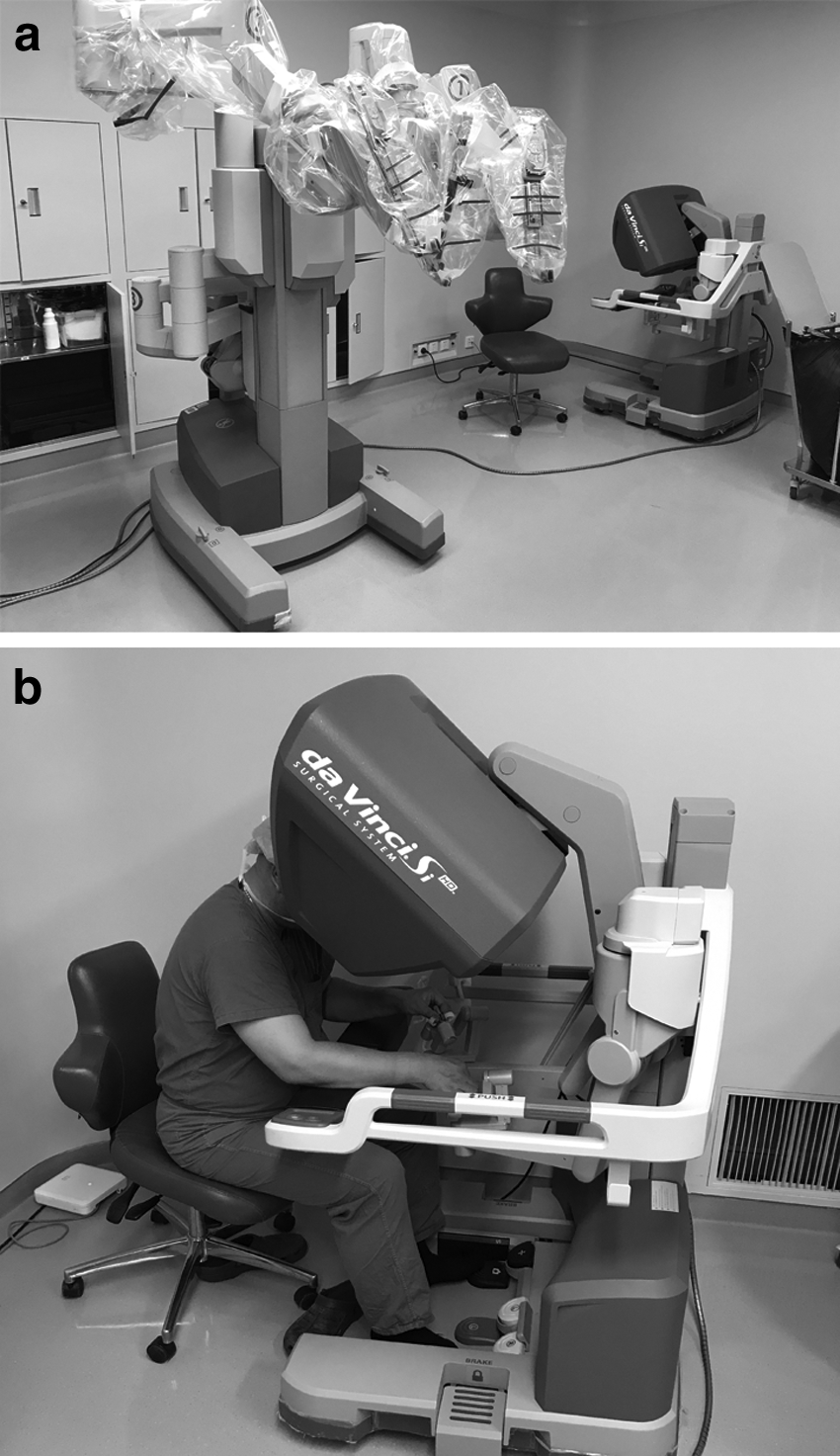
We used the da Vinci Surgical System (Intuitive Surgical) for the robotic procedure. Figure 1 shows the robotic arms and the surgeon's console used throughout this study.
The patient was placed supine with lithotomy position and 15° right down. Five holes were used in the operation and the trocar location (as shown in Fig. 2) as follows: the lens hole C: a 10-mm trocar was placed in the right upper quadrant, 4–5 cm upper right of the navel. Operational hole R1: an 8-mm trocar was placed on the right side of the Mcburney point. Operational hole R2: an 8-mm trocar was placed on the left side of the Mcburney point. Operational hole R3: an 8-mm trocar was placed on the intercostal clavicle midline across the level of hole C. Assistant hole A: a 12-mm trocar was placed on the same vertical curve as R1 across the level of the navel.

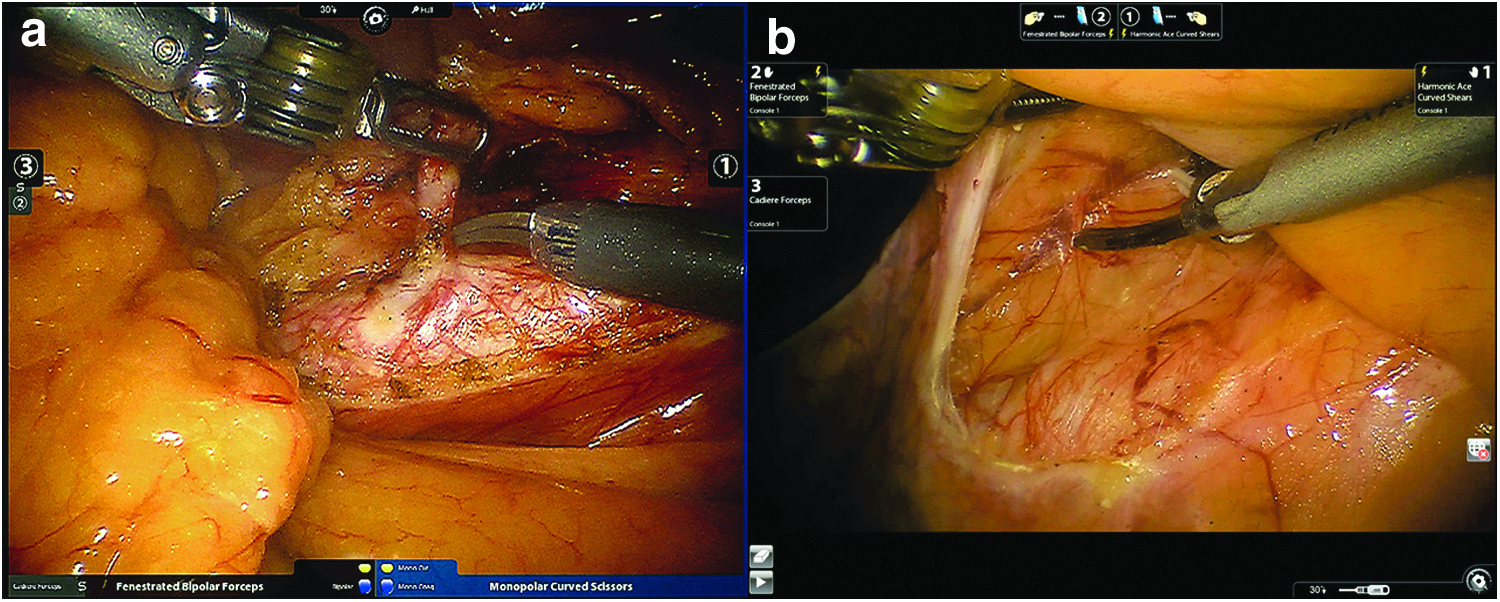
First, the inferior mesenteric artery and vein were divided proximally using clips. Second, the rectum was dissected in the mesorectal plane with total mesorectal excision principles. Third, the rectum was split using an Endo-GIA. Twenty-two cases underwent resection using monopolar electrosurgical scissors and 24 cases underwent resection using the harmonic scalpel (as shown in Fig. 3).
The robotic instrument was then disengaged. The specimen was extracted through the R2 trocar incision, which was enlarged to ∼4 cm. The wound was covered with a plastic wound protector. An end-to-end anastomosis (EEA) anvil was then placed in the proximal colon and secured with a purse-string suture. The colon was placed back into the abdomen and the port site was closed. Pneumoperitoneum was restored, and an EEA stapler was used to create an EEA under monitoring.
Statistical analysis
All analyses were conducted using IBM SPSS 16.0 software (SPSS, Inc., Chicago, IL). The chi-squared test for categorical variables and Student's t-test for continuous variables were used for statistical comparisons of patient characteristics, perioperative clinical results, and pathologic details between the two groups. P values <.05 were considered to be statistically significant.
Results
Patient characteristics
Patient characteristics were analyzed by comparing the monopolar electrosurgical scissors cases (n = 22) and the harmonic scalpel cases (n = 24) (Table 1). Gender ratio, mean age, distribution of the tumor-node-metastasis stage, and tumor distance from anal verge were not significantly different between the groups.
Patient Demographics
SD, standard deviation.
Three patients in the monopolar electrosurgical scissors group underwent neoadjuvant chemoradiotherapy and 4 patients in the harmonic scalpel group underwent neoadjuvant chemoradiotherapy.
Perioperative clinical results between groups
The mean operative time was significantly lesser in the monopolar electrosurgical scissors group than in the harmonic scalpel group [95.59 ± 21.44 minutes versus 81.45 ± 13.89 minutes, P < .01] (Table 2). The mean estimated blood loss was lesser in the monopolar electrosurgical scissors group than in the harmonic scalpel group [48.64 ± 19.35 mL versus 61.82 ± 24.23 mL, P = .03]. As for postoperative clinical characteristics, the complication rate was 18.2% in the monopolar electrosurgical scissors group and 16.7% in the harmonic scalpel group (P = .89) (Table 3). The mean time of postoperational urinary catheter was lesser in the monopolar electrosurgical scissors group [3.73 ± 1.16 days versus 4.59 ± 1.71 days, P = .02]. The day to first passing flatus [3.45 ± 0.80 days versus 3.59 ± 1.14 days, P = .67], feeding time [4.50 ± 1.00 days versus 4.05 ± 1.87 days, P = .35], hospital stay [8.18 ± 3.74 days versus 8.68 ± 3.44 days, P = .52], and the mean number of harvested lymph nodes [13.59 ± 1.71 versus 13.77 ± 1.41, P = .67] were comparable between the procedures. The circumferential resection margin involvement was not found in both groups.
Comparison of Operative Clinical and Pathologic Results Between Groups
SD, standard deviation.
Comparison of Postoperative Complications Between Groups
Discussion
Minimally invasive surgery has become the gold standard of care for elective colonic surgery. 8 As the ideas of operation concept changes, surgeons focus more on postoperative function preservation. 9 Pelvic autonomic nerve preservation in narrow pelvis is essential for colorectal surgeons to obtain good functional outcome after rectal cancer surgery. 10 Developments in robotic technology have been gaining popularity over the past few years, which enable overcoming these difficulties caused by complex pelvic anatomy. 11 With superior three-dimensional views, tremor filtering, and angulated instruments, robotic surgery enables precise dissection in narrow surgical space, therefore, enabling better preservation of the pelvic autonomic nerves. 12
In our hospital, there were three types of anterior resection of rectal cancer: open, laparoscopic, and robotic. The surgical fees were same but the equipment fees were not. Patients who underwent robotic surgery would pay $4390 for the da Vinci Surgical System (Intuitive Surgical). Owing to the high price of the robotic system, the number of patients was limited.
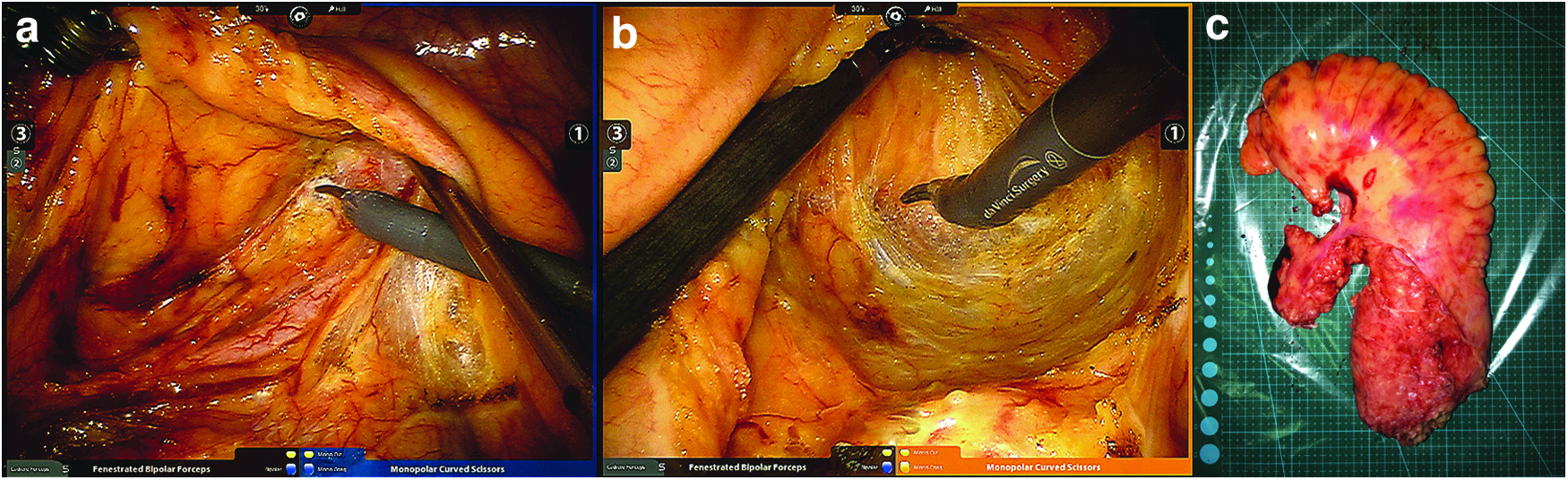
The cost of robotic monopolar scissors was included in the robotic cost as a standardized surgical instrument, while the cost of a harmonic scalpel was not included. Patients would pay ∼$205 in addition for using harmonic scalpel in the surgery. Originally, we used monopolar scissors instead of harmonic scalpel to help patients save money. In practice, we found that the monopolar electrosurgical scissors had its unique advantages in preservation of the pelvic autonomic nerves. We thought that the monopolar electrosurgical scissors would be more beneficial in rectal cancer surgery than harmonic scalpel. First, monopolar electrosurgical scissors can do blunt and sharp separation in surgical operations (as shown in Fig. 4a). Second, the technique of blunt and sharp separation combined with high magnification of robotic lens can improve the accuracy of pelvic autonomic nerve preservation (as shown in Fig. 4b), which is associated with postoperative sexual and voiding functions. Third, surgeons can also reduce the energy level of monopolar electrosurgical scissors for patients with very low BMI according to thin abdominal adipose.
In this study, operative time and estimated blood loss of the monopolar electrosurgical scissors group were less than those of the harmonic scalpel group. The 360° free rotation arm enables the monopolar electrosurgical scissors to do sharp separation and monopolar cutting in the mesenteric avascular area within the narrow pelvic, whereas the long-handled harmonic scalpel has to adjust the lens and change direction frequently, which may not only increase bleeding but also extend the duration.
The result showed less indwelling urinary catheter time in the monopolar electrosurgical scissors group, which indicated that monopolar electrosurgical scissors have advantages in urological function preservation and may be related to better pelvic autonomic nerve preservation. However, this study did not apply any functional estimate for the assessment of hyperfunction, leaving it open to observation bias.
As for complications, conversion did not occur in both groups, owing to Dr. M.Z. who has a great technological advantage in laparoscopic surgery. The overall complication rate, which included anastomotic leakage, intraluminal bleeding, ileus, pleural effusion, and pelvic infection, was not statistically different between the groups. There were also no statistical differences in feeding time, days of first passing flatus, and length of stay between the groups.
It is a remarkable fact that the quality of the resected specimen is related to oncologic outcomes. 13 Adequately, lymph node dissection and macroscopic completeness of resected rectal specimen are two main factors that show the quality of the resected specimen. In this study, the harvested lymph nodes were comparable between groups. As a result, the quality of the resected rectal specimen in the monopolar electrosurgical scissors group was fine (as shown in Fig. 4c). There was no statistical difference in pathologic results between the groups.
This study has several limitations. The first is that this study is based on a single-institution experience. Choosing monopolar electrosurgical scissors or harmonic scalpel was decided by the surgeon according to the intraoperative situation, retrospective nature of our investigation is prone to selection bias. We minimized this bias by choosing the same surgeon and met the selection criteria during the defined study period. The second limitation is that this study did not apply any functional estimate for the assessment of urological function preservation. The third limitation is that there were not enough patients with rectal cancer who could afford to pay the fee for the robotic surgical system to be included in this study. Despite these limitations, this study presents significant findings that underscore the need for future randomized prospective trials.
Conclusions
This study demonstrated that the monopolar electrosurgical scissors were used safely and effectively in robotic anterior resection of rectal cancer (using the da Vinci Surgical System). The use of monopolar electrosurgical scissors has advantage in performing blunt and sharp separation in narrow pelvic and lower hospital expenses.
Footnotes
Acknowledgments
This work was supported by grant from National Natural Science Foundation of China (No. 81672347 to M.Z.), National Natural Science Foundation of China (No. 81702300 to M.H.Y.), and the grant from Municipal Commission of Health and Family Planning of Shanghai, China (No. 201640290 to H.Z.).
Disclosure Statement
No competing financial interests exist.