
Abstract
Abstract
Introduction:
Accidental thermal injuries are infrequent, nonetheless, dangerous complications in laparoscopic surgery. Burns are produced because of direct contact, lack of instrument insulation and capacitive coupling. Biological fluids on the surface of laparoscopic instruments behave as electric conductors on the sheath and may be responsible for accidental thermal injuries. Our hypothesis is that using an insulator device may prevent those injuries.
Materials and Methods:
After evaluating different materials for dielectric properties, costs, and temperature increase tolerance, we selected polytetrafluoroethylene (PTFE) to develop a sleeve that works as an electrical insulator when applied on the sheath of laparoscopic instruments. Efficacy of this PTFE cover in reducing conduction of electricity was tested on both reusable and disposable laparoscopic instruments.
Results:
Electric conduction of the laparoscopic instrument sheaths was tested using an ex vivo model that reproduces the abdominal environment in basal conditions and in presence of blood. Electric conduction of laparoscopic instruments was measured before and after the placement of the PTFE cover. We measured a significant difference in electric resistance on the sheath's surface without and with blood, revealing a weak electrical conduction: infinity versus a median value of 251.11 Mohm, respectively.
Conclusions:
This ex vivo study demonstrated that a PTFE sleeve may reduce electricity conduction of laparoscopic instruments. A pilot in vivo study is planned to test its safety and efficacy.
Introduction
Accidental thermal injuries during laparoscopic surgery are infrequent complications, but their consequences may be catastrophic. The reported incidence of laparoscopic accidental burns is between 2.3 and 4 cases every 1000 major operations. 1 According to Willson et al., 47% of the laparoscopic incisions, where the active electrode was inserted, showed histologic evidence of thermal injury due to capacitive coupling. 2 Almost 18% of general surgeons and 33.3% of gynecologists have experienced direct or indirect burns 3 ; moreover, many injuries could be clinically uneventful, thus unreported.
Thermal injuries during laparoscopy may be produced with three different mechanisms: (1) energy is transferred through a physical contact between two conductors, usually due to human error; (2) lack of insulation due to a defect of the instrument's surface sheath determining an electric dispersion; and (3) capacitive coupling, 4 caused by the electrical charge stored between two conductors separated by an insulator.
Blood and other extracellular fluids can be considered electrolytic solutions due to the imbalanced distribution of electrons resulted from chemical dissociation. We hypothesize that the presence of biological fluid on the surface of laparoscopic instruments may work as an electric conductor thus exposing to the risk of a thermal injury due to lack of insulation or to capacitive coupling. We have developed a reliable and cost-effective tool that helps preventing accidental thermal injuries during laparoscopic surgery in form of a cover to be applied on the sheath of laparoscopic instruments that is capable of separating the ions of an electrolytic solution eventually present on the instruments, while providing insulation.
Materials and Methods
The study was divided in three phases.
In the first phase, we analyzed the heat/energy dispersion on laparoscopic instruments through different mathematical models based on morphology created via the MATLAB (MathWorks, Inc., Natick, MA) software (Fig. 1). Those algorithms are capable of detecting erosions, tears, and dilation of an instrument from the analysis of a 2D image shot with a D80 Digital SLR Camera equipped with 18–135 mm f/3.5–4.5G IF-ED lens (Nikon Corp., Tokyo, Japan). We used this technique to test 63 laparoscopic instruments coming from two sets of 37 disposable and 26 reusable tools. Instruments were discarded and removed from the data analysis only if gross damage was present on their surface. We then validated those results by performing the analysis of the infrared emissions of each instrument detected with a thermographic camera (Fluke Ti32; Fluke Electronics Corporation, Everett, WA). We tested both instrument sets for three times, each one to detect thermal dispersion, utilizing three different power intensity settings for the active electrode: low, medium, and high.

In the second phase of the study, we aim to identify an absorbing material capable of preventing electrical conduction. For this purpose, we took the following materials into consideration: Poly(methyl methacrylate) (PMMA), Polyvinyl chloride (PVC), Polytetrafluoroethylene (PTFE), and Polyesters. We compared their peculiar characteristics in terms of absorption capability, low dielectric constant and high dielectric strength, resistance to cutting, banding, torsion, and compression. A cost analysis of each material was performed as well. Due to its characteristics, we deemed PTFE to be the most adequate material for our purpose and created a prototype of insulating cover for the laparoscopic instruments. To verify the ability of PTFE to maintain intact its characteristics over time, we submerged the PTFE prototype for 22 hours in 60 mL of a solution obtained from pig blood and standard saline (ratio 2:3) with the addition of 5 mL of Anticoagulant Citrate Dextrose Solution and then measured the electric resistance of the device with a multimeter (Tektronix dmm914; Tektronix, OR). Blood was our model of a weak electrolytic solution, partially composed of dissociated molecules and capable of transferring electric current through its ions.
For the third phase, we utilized a simulation model capable of reproducing the physical conditions expected into the abdominal cavity. Testing of the electrified laparoscopic equipment was performed after extensive use of the instruments on ex vivo porcine tissues (kidney, bowel, and liver). First, using the same multimeter used during phase 2, we measured the electric resistance on the surface of the dry sheath, then in presence of pig blood on its surface. We repeated the tests applying the cover on the instruments and using electrocautery on tissue while recording the electrical conduction on the instrument's surface. We repeated the test twice for each instrument, both in dry and wet conditions (pouring 2 mL of blood on the instrument).
Results
In Phase (I), we tested, for three consecutive times, a series of 63 reusable and disposable laparoscopic instruments—two instruments were excluded from the sample because they presented sheath damage recorded at least twice by the thermographic camera analysis. Other undamaged instruments initially showed microscopical defects on their surface at the mathematical morphological analysis. However, the evaluation with the thermographic camera did not show any kind of electric conduction on the sheath for each power setting of the electrode (low, medium, and high). The absence of electric dispersion was proved by the infinity value of resistance recorded by the multimeter in each performed measurement. This proved our hypothesis that, in case of proper instrument insulation, the presence of biological fluid on the surface of laparoscopic instruments may work as an electric conductor through the phenomenon of capacitive coupling.
In Phase (II), we compared different materials supposed to have adequate insulating properties: PTFE, PMMA, and Gore-tex® (Table 1). 5 We designed a PTFE insulating cover (Fig. 2), in the shape of a hollow cylinder that slips on the existing insulating sheath of the instrument. The device measures 5 mm (inner diameter) × 50 mm (length) × 1 mm (thickness), weighing 2.07 g at a cost of ∼0.06$ per unit. We chose PTFE because its degradation point is over 260°C. The coefficient of friction for plastics is usually measured against polished steel and PTFE's coefficient of friction ≤0.1 is the second lowest of any known solid material. 6 It has excellent dielectric properties and combines high-performance with acceptable costs (Table 2). Our PTFE cover is 1 mm thick and does not hinder the use of conventional laparoscopic instruments through 5 mm trocars. The device has been patented. 7
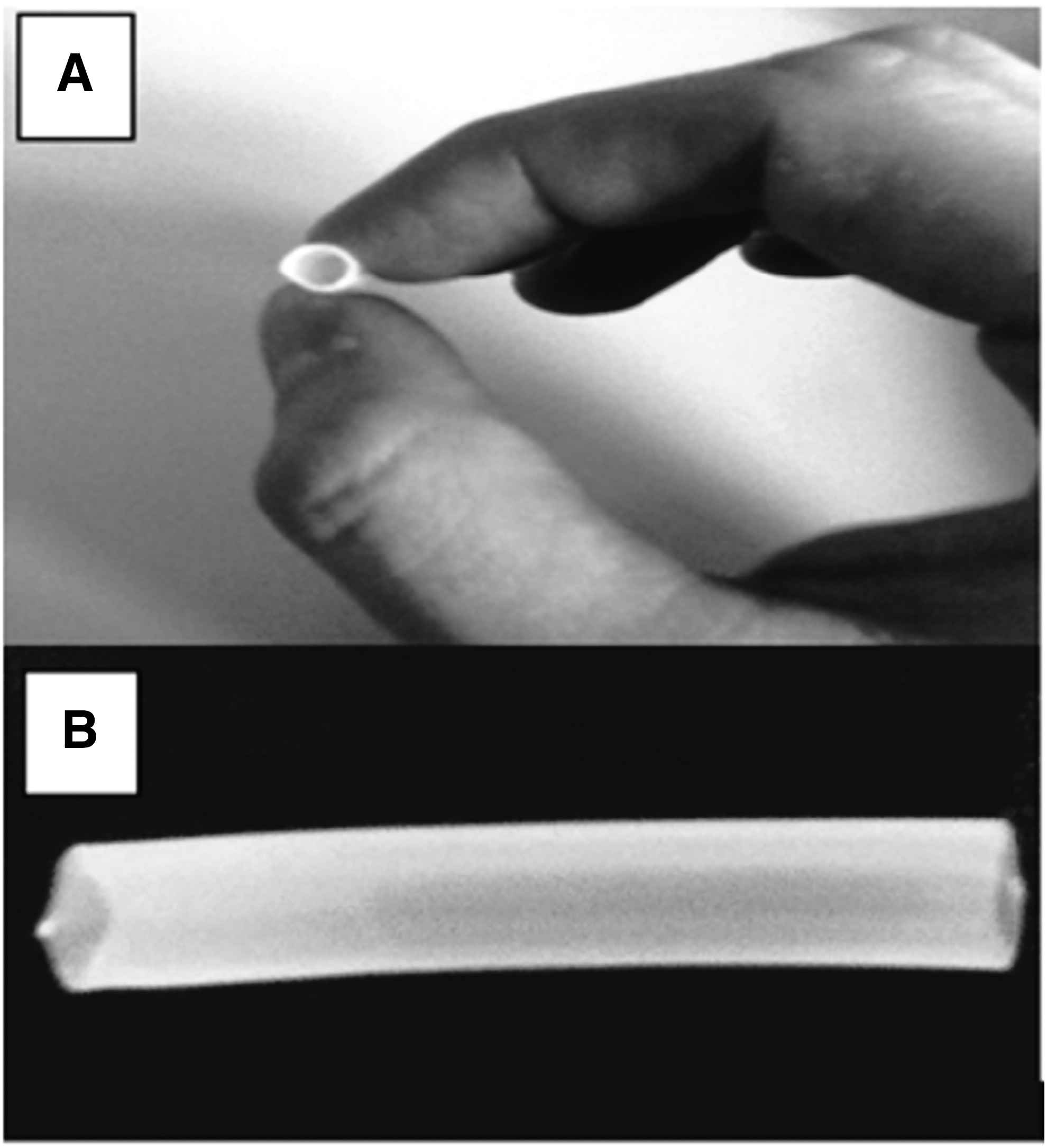
Cover filter device.
Electrical Properties of Different Tested Materials a
Coleman et al. 5
Physical, Thermal, and Electrical Features of Polytetrafluoroethylene
In Phase (III), following the exclusion of two damaged instruments, we tested the remaining 61 instruments reproducing the conditions expected in an abdominal cavity. We measured a significant difference in electric resistance on the sheath's surface without and with blood, revealing a weak electrical conduction: infinity versus a median value of 251.11 Mohm, respectively. We repeated the same tests after the application of the PTFE cover on the laparoscopic instruments measuring exponential changes in electric resistance compared to the previous test results (Figs. 3 and 4). Through ionic separation and the increase of the dielectric constant, the PTFE cover prevented the capacitive effect and no electrical dispersion could be measured with the cover on.
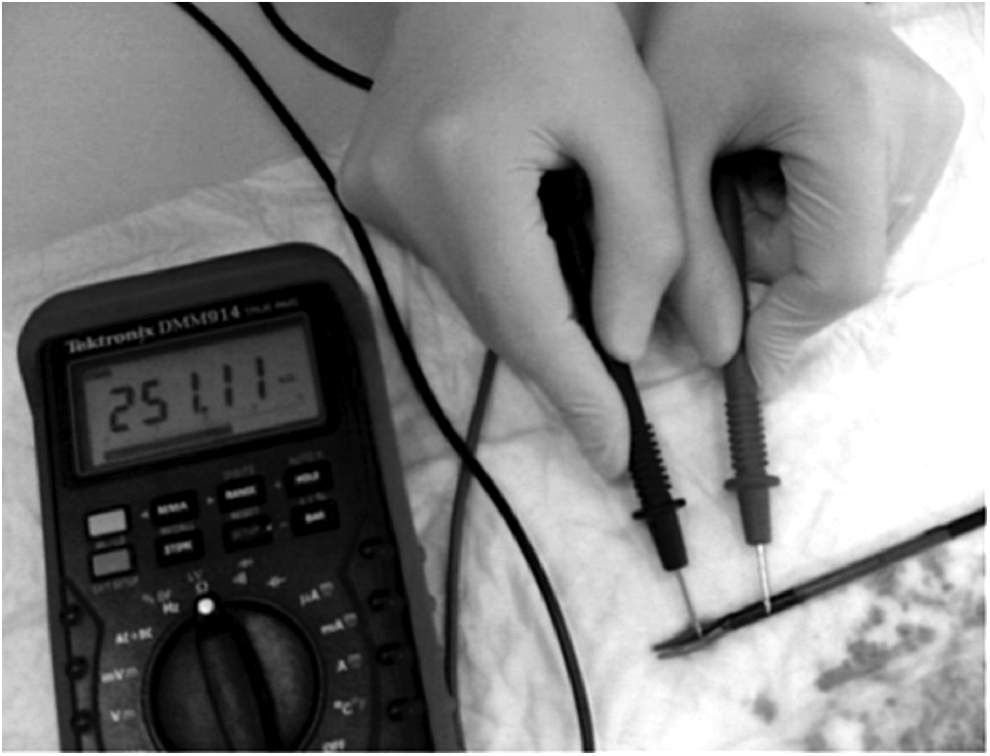
Electric resistance on wet sheath (no cover device) = 251.11KΩ.

Electric resistance on wet sheath (with cover device) = ∞. The symbol 0.L stands for infinite resistance.
Discussion
Accidental thermal injuries during laparoscopic surgery are rare complications; however, they can have serious repercussions on patient's health, can prolong the postoperative time of recovery and, as a consequence, determine an increase in health care costs. 1 Several studies on the safety of laparoscopic instruments were focused on the integrity of the plastic sheath. Insulation failure is the most common electrosurgery injury and has the highest probability of causing an irreversible, full-thickness, intestinal thermal injury. Recent studies have estimated a prevalence greater than 20% of instruments with insulation defects, with over 50% of the defects being undetectable with the naked eye. 8 However, thermal injuries can occur even in case of undamaged sheaths. In this case, our hypothesis is that the occurrence of accidental burns is related to the electric conduction generated by the presence of biological fluids on the instrument's sheath, functioning as a conducting electrolyte solution that increases the electric dispersion over the length of the instrument. We developed a PTFE cover with filtration and adsorption properties that can separate ions and decreasing the capacitive effect on the surface of the instruments.3,9 The capacitive effect can be neutralized using an electrical filter with low dielectric constant and high dielectric strength.
The performed experiments confirmed that the use of adsorbing material applied on the surface of the sheath acts in two ways: avoiding the transfer of electric current, thanks to the ionic separation, and by increasing the dielectric constant to avoid the capacitive effect. 9 The first mechanism involved is adsorption. It is a process in which atoms or molecules move from a bulk phase (solid, liquid, or gas) into a solid or liquid surface. Adsorption must be distinguished from absorption, a process in which atoms or molecules move into the bulk of a porous material, such as the absorption of water by a sponge. At the molecular level, adsorption creates a film of the molecules or atoms accumulated on the adsorbent's surface. The physical process of adsorption is a consequence of surface energy. 10 Our measurements clearly show an increase of the electric resistance when the blood gets in contact with the adsorbing material, meaning that the electrical transfer to the near tissue is more difficult than in standard conditions.
The second mechanism involved, known as capacitive effect, is the transfer of electric current between two conductors, despite the presence of an intact insulation between them. This effect can be neutralized using a material that works as a filter with low dielectric constant and high dielectric strength. More in depth, a low dielectric constant explains how effective a dielectric is at allowing a capacitor to store more charge, depending on the material the dielectric is made from.9,11 The capacitance is maximized if the dielectric constant is maximized; if a metal was used for the dielectric instead of an insulator, the field inside the metal would be zero, corresponding to an infinite dielectric constant. The capacitive coupled current completes the circuit by finding a pathway to the patient's return electrode.12,13 The charge is stored in the capacitor until the generator is deactivated or a pathway completing the circuit is achieved. Capacitive coupling is greatest in the “coagulation” mode of the electrified instrument, when there is no load on the circuit (open circuit).14–17 The PTFE cover filter solves this problem because its low dielectric constant and high dielectric rigidity make it difficult to store electrical charge and prevent the transfer of electric charges to the surrounding tissues.
Our experiments demonstrated the efficacy of the PTFE cover to prevent thermal injuries from electrical conduction in presence of biological fluids that behave as electrolyte solutions. However, our study presents some limitations as well. First of all, the use of the sleeve will not prevent injuries from accidental contact with the working tip of the instrument. Second, the number of tests performed is relatively limited, in consideration of the incidence of the event that we aim to prevent (4/1000 procedure). A larger sample of procedures, as well as a wider adoption of the device in the routine surgical practice, would also be required to assess the complete efficacy of the PTFE device in vivo, test for eventual design pitfalls that prevent the device from slippage or rupture after prolonged and continuous use. Also, the length of the cover device was chosen to lower the costs and increase its usability, with the assumption that covering the first 5 cm tract of the instrument from the active electrode extremity would be adequate enough to prevent electrical current dispersion as well as capacitive coupling. For this reason, different sizes of the device might provide different performances.
Conclusions
Accidental thermal injuries during laparoscopic surgery may be produced by a low electrical dispersion from the active instrument when in contact with blood or other biological fluids. The standard electrical insulation of the laparoscopic instruments may not always be sufficient to prevent this risk, due to the lack of adequate adsorbance capabilities of the materials used. We demonstrated that a PTFE cover is a reliable and cost-effective tool for the prevention of accidental thermal injuries during laparoscopic surgery. In vivo case–control studies are needed to obtain definitive data. We demonstrated that our solution is reliable and cost-effective for the prevention of accidental thermal injuries during laparoscopic surgery.
Footnotes
Disclosure Statement
Francesco Maria Carrano (F.M.C.), Marcovalerio Melis (M.M.), and Silvia Quaresima(S.Q.) have no conflicts of interest and/or financial ties to disclose. Luca Iezzi (L.I.), Achille Lucio Gaspari (A.L.G.), and Nicola Di Lorenzo (N.D.L.) own the intellectual property of the device tested in the article and have no financial ties to disclose.