
Abstract
Abstract
Background:
Appropriate tissue retraction is essential in laparoscopic surgery, and colorectal operations often require an additional incision and trocar that can disturb visualization and maneuverability. Each incision carries an increased risk for complications as well as increased pain and cosmetic issues. Magnetic devices have been developed for a less invasive retraction. The objective of this study is to report our initial experience using magnet retraction.
Methods:
Ten consecutive patients who underwent laparoscopic colorectal procedures by a single surgeon using a magnetic retractor (Levita Magnetics® Surgical System, San Mateo, CA) between October 2017 and June 2018 at Duke Regional Hospital in Durham, NC, were included.
Results:
The cases included four single-port right colectomies, one sigmoidectomy, and five rectopexies. Nine cases were completed laparoscopically, as one right colectomy required conversion due to adhesions and bulky specimen. Indications included adenocarcinoma, diverticular disease, and rectal prolapse. The magnet was successfully used for uterus, colon, or colonic pedicle retraction. No intraoperative or 30-day complications were observed.
Conclusion:
Magnetic surgical retractors are a safe, dynamic, and incision-less option for surgical field exposure during laparoscopic colorectal surgery. Reduced trocars decrease tissue trauma, enhances maneuverability, and potentially improves outcomes; however, further studies are required.
Introduction
Since the introduction of laparoscopic colectomy in 1991, 1 minimally invasive surgery has gained widespread adoption in colorectal surgery. Current estimates report that 59% of all elective colectomies today are performed laparoscopically 2 and as evidence of safety and efficacy emerges, other common colorectal procedures such as rectopexy, sigmoidectomy, and rectal resections are finding success with laparoscopic, single-port, and robot-assisted platforms. 3
The objective of a minimally invasive technique is to reduce the number of ports required to perform a surgical procedure without compromising safety or efficacy. 4 A reduction in surgical abdominal incisions, in theory, leads to decreased postoperative pain and wound complications. However, many less invasive techniques also introduce new challenges related to the limited working space, which include internal and external instrument collisions, suboptimal tissue retraction, and prolonged operative times.
To address these challenges, magnet-assisted surgery devices have emerged. Their use has been established to be safe, feasible, and helpful in abdominal procedures such as cholecystectomy and retraction in bariatric surgery.5–8 In colorectal surgery, this device includes a magnetic grasper tip that is deployed into the peritoneal cavity through one of the abdominal ports and an external handheld magnet controller that is placed on the abdominal wall for manipulation. The introduction of the device through an already existing port allows an incision-less retraction while preventing the need for additional instrumentation in the surgical field. The objective of this study is to report our first experience using this device for colorectal surgery at our institution.
Methods
Patients
The Institutional Review Board (IRB) at the Duke University Health System approved this study. The study population comprised 10 consecutive patients who were scheduled for a colorectal operation at Duke Regional Hospital (Durham, NC) between October 2017 and June 2018. All patients were screened to ensure that there were no metallic or electronic objects on or in their bodies that could interfere with the magnets. They were informed and consented to the procedure preoperatively. All operating room staff handling the magnets completed in-service training to ensure safe and appropriate use of the device. Study data were collected and managed using REDCap® electronic data capture tools hosted at Duke University. 9
Device
The magnetic retractor (Levita Magnetics®, San Mateo, CA) (Fig. 1) is the first magnetic surgical system to receive Food and Drug Administration (FDA) approval for use during laparoscopic cholecystectomy in June 2016. The system is composed of an internal metallic grasper with a detachable tip that couples with an external magnet controller. The external magnet is positioned using a standard bedrail mounted arm. Owing to its small size, it can be easily maneuvered across the abdominal wall and does not interfere with traditional port placement. The grasper tip is introduced through an existing 12 or 15 mm port at the end of a magnetized instrument and clamped to the desired organ or tissue. The external magnet is then placed over the abdominal wall, coupled to the detached grasper tip, and magnetic attraction allows for manipulation of the grasper tip to retract the desired organ or tissue. Once the procedure is complete, the external magnet is decoupled, and the grasper tip is retrieved from the abdominal cavity using the same introducer instrument (Supplementary Video S1, “Magnetic retraction in colorectal surgery”).
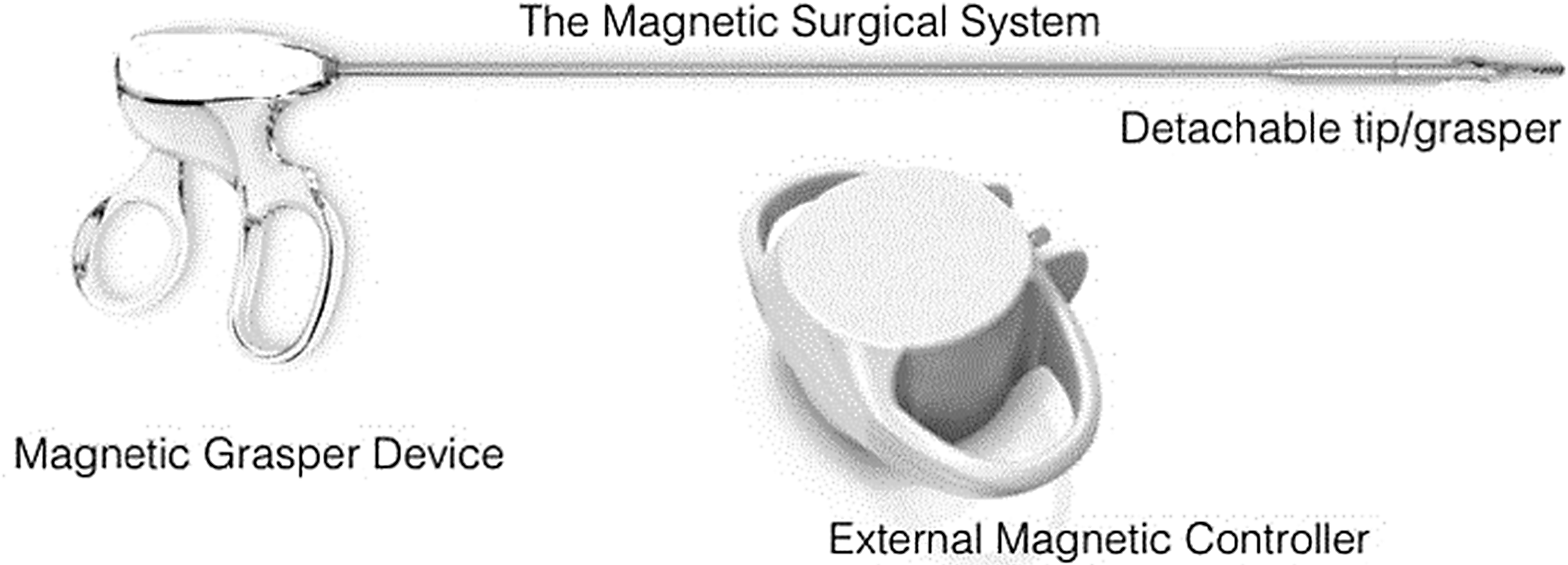
Levita Magnetics® Surgical System.
Procedures
Suture rectopexy
Entry into the abdomen is obtained through a 5 mm optical trocar in the left mid-abdomen along the mid-clavicular line. This trocar is eventually converted to a 12 mm port for introduction of the detachable magnetic grasper tip. One additional 5 mm trocar is placed ∼3 cm to the right of the umbilicus and another 5 mm trocar placed in the left lower abdomen cephalad to the anterior superior iliac spine. The three trocars are placed in a curvilinear inverted U-shaped alignment. The procedure is completed using the two left-sided ports for introduction of the suture and magnetic grasper. The magnetic grasper tip is used to retract the sigmoid colon anterolaterally and out of the pelvis for posterior dissection of the rectum. In addition, the magnetic grasper tip is placed on the uterine ligaments to retract the uterus anteriorly for better visualization in the pelvis (Figs. 2 and 3).
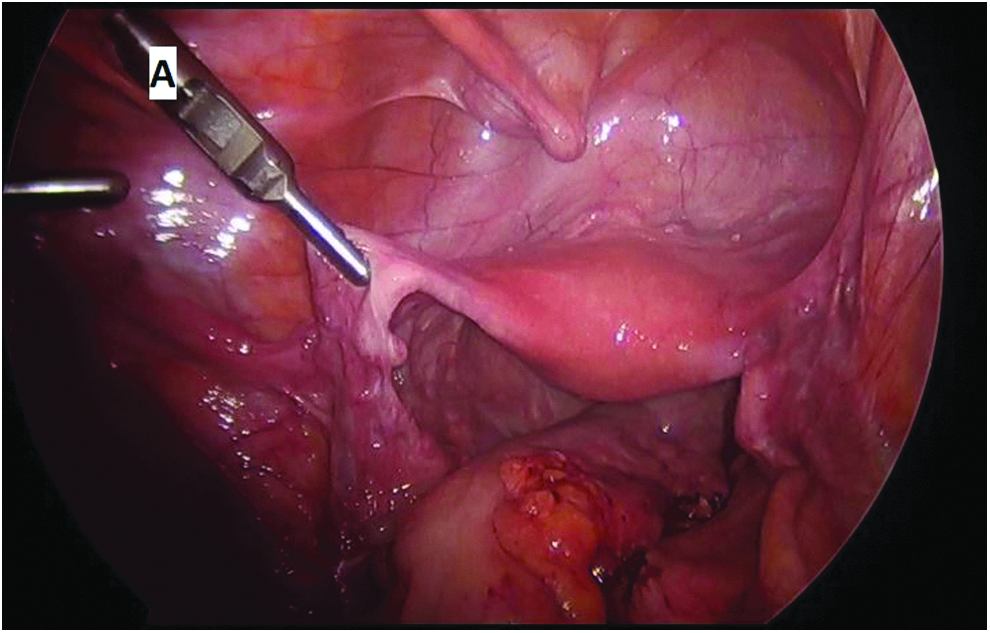
Magnetic device
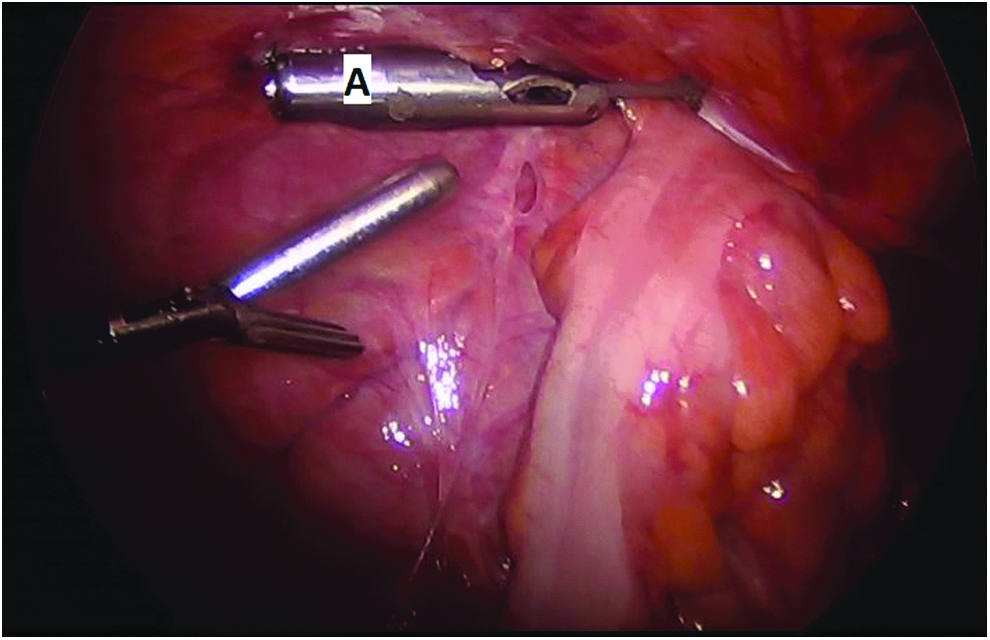
Magnetic device
Colectomy
Right colectomy
For single-incision cases, a vertical periumbilical 4–5 cm incision is made for entry into the abdomen. A single incision access platform (Gelpoint®; Applied Medical, Rancho Santa Margarita, CA) is placed with three 12 mm access trocars and a flexible tip laparoscope. For multiport cases, the abdomen is entered through direct cutdown in the periumbilical region for a 12 mm port. Additional 5 mm trocars are placed in the left upper and lower abdomen. The magnetic grasper tip is placed on the right colon epiploica or mesentery of the ileocolic pedicle for lateral retraction during medial to lateral mobilization of the right colon. The inferior dissection of the ileocolic pedicle and mesenteric window are created with the help of the magnetic device (Fig. 4).

Magnetic device medially retracting right colon mesentery.
Left colectomy and sigmoidectomy
Entry into the abdomen is obtained in a similar manner to a multiport right colectomy. A 12 mm port is placed in the right lower quadrant for introduction of the magnet grasper and a 5 mm port is placed in the left mid-abdomen. The case is completed using three trocars. The magnetic grasper tip is used to retract the descending/sigmoid colon anteriorly during medial to lateral mobilization of the left colon as well as to provide retraction of the left colon mesentery during isolation of the inferior mesenteric artery. The omentum is retracted anteriorly using the magnetic grasper tip during dissection of the omentum off the transverse colon. In addition, the magnetic grasper tip is used to retract the uterus anteriorly for better visualization into the pelvis.
Results
The 10 cases comprised 4 right colectomies, 1 sigmoidectomy, and 5 rectopexies. Nine cases were completed laparoscopically. One right colectomy case required conversion to open due to dense adhesions and a bulky specimen. Indications for surgery included four right colon adenocarcinomas, one sigmoid diverticular disease, and five rectal prolapses, respectively. In every case, the magnetic system was successfully employed for retraction of the colon, uterus, or colon mesentery. Mean operative times for rectopexies and single-port right were 157 and 176 minutes, respectively. Additional details of each procedure are presented in Table 1. No intraoperative or 30-day complications were noted or attributed to the internal gasper device or external magnet.
Patients' Demographic Information Who Underwent a Colorectal Procedure Using the Magnetic Retractor
Converted to open.
BMI, body mass index; F, female; LAP, laparoscopic; LOS, length of stay; M, male; OP, operative time; R, right; SP, single port.
Discussion
The use of magnets in surgery dates from the 19th century. 10 They have been used in multiple applications such as anchors, traction, intestinal anastomosis, and gastroesophageal reflux surgery. 11 As previously noted, countertraction is one of the key steps during open or minimally invasive procedures. Experimental studies have been published using magnets in animal models with positive outcomes. Scott et al. applied this technique in an animal model cholecystectomy for retracting the gallbladder fundus without complications. 12 A similar concept was described in an animal model nephrectomy, Choi et al. used a magnet fixed with sutures to the renal parenchyma to move the kidney with an external magnetic component located outside the abdomen. 13
Several methods have been described for retraction during laparoscopic colorectal surgery and magnets have been categorized as gravitational retractors. 14 Kume et al. first described using an intraluminally placed magnet coupled to an additional external magnet across the abdominal wall to retract the colon in a porcine model. 15 Subsequently, Uematsu et al. published a series of 7 human patients with colon cancer and single-port colectomies. They employed vascular forceps introduced into the abdomen to effectively pull the desired tissue with an external magnet positioned over the abdominal wall without any reported adverse events. 16
This same magnetic retraction system has previously been studied in other abdominal surgeries. Rivas et al. published the first experience in human application using this magnetic retractor in 50 cholecystectomies without any related complications. 7 Haskins et al. reported on 10 cholecystectomies using the magnetic retractor without adverse events—the first trial of this type conducted in humans in the United States. 6 Based on our personal experience and acquired capabilities regarding this particular device, we have observed various benefits for the patient such as fewer incisions and subjectively reduced postoperative pain. Recently, we successfully performed a single-port robotic cholecystectomy using magnetic retraction, making this the first case reported of this technique in humans. 5 The efficient movements achieved with the attached tissue and the external component facilitated our visualization and eliminated the need for an additional port for countertraction.
There are several direct patient benefits of magnetic retraction that reach beyond simple retraction and visualization, which stand to primarily aid the surgeon. The cosmetic benefits of fewer incisions may initially seem negligible, but is significant. Surgical scars are an important part of the preoperative discussion between surgeon and patient that is frequently neglected and undervalued.17,18 When given the choice, patients usually choose less-invasive approaches and clinicians often fail to consider these opinions.19,20 Fewer incisions naturally decrease the risk for surgical site infections (SSI), which is the most common hospital-acquired infection for surgical patients and a leading cause of morbidity and financial burden.21,22 SSI rates vary widely by the type of procedure performed with colorectal surgery among the highest with occurrences in up to 32% of cases.23–25 Although the actual risk reduction of one less incision has not been fully defined, the advantages to patient comfort and faster healing are in line with the principles of enhanced recovery after surgery. 26
One clear limitation of this study involves a lack of assessment of exposure and retraction. Although no specific objective data were collected, our experienced colorectal surgeon rated exposure and retraction as appropriate in all cases. Concern of tissue injury from the device when clamped to the various structures also warrants discussion. It is worth mentioning that although we did not experience any significant injury or tissue trauma, it is simply our observation that the device did not pose any additional risk when compared with conventional retracting methods. These findings are subjective and further investigations into quality of exposure and potential operative risks from device use would be of value.
The mean operating times for rectopexies and single-port right colectomies were marginally longer than times published by other authors.27–29 This may be related to the learning curve commonly seen with new device use. We believe that further experience with the device will allow for a decrease in future operating times that will be more consistent with national norms.
Another limitation of this study is its observational nature and narrow population application. Nevertheless, this initial experience encourages further use and development of this technique supported by positive outcomes, easy reproducibility, and effectiveness. Even though further analysis is needed to evaluate the real impact of this device in colorectal surgery, we believe it can prove to be useful for other surgeons.
Conclusion
The use of magnetic retraction systems provide a safe, dynamic, incision-less, and less painful option for organ retraction while offering improved visibility during laparoscopic colorectal procedures. The reduction of trocars decreases tissue damage and improves the surgeon's intra-abdominal maneuverability with potential patient benefits such as improved cosmesis and decreased SSI risk. Further investigations and trials should be performed to compare outcomes of magnetic retraction with more traditional methods.
Footnotes
Authors' Contribution
Each author provided substantial contributions to the conception, design, analysis, interpretation, drafting, revising, and critical feedback of important intellectual content. Each author has given final approval of the version to be published and agrees to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Disclosure Statement
G.D., R.D., L.K.W., B.L., and E.R. have no conflicts of interest. D.P. has received an education grant from Levita Magnetics®, has received an education grant from Gore, is a consultant and has received a research grant from Medtronic®, and is a consultant for Intuitive. A.D.G. is a consultant for Levita Magnetics, and a speaker for Gore and Medtronic. Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.