
Abstract
Background:
In this article, we report our experience on laparoscopic pneumovesical Cohen approach for vesicoureteral junction (VUJ) stricture in children and compared it with traditional open Cohen approach.
Patients and Methods:
Ninety-eight children (114 ureters) with VUJ stricture were involved in this study who were treated from January 2008 to December 2017. Forty-eight patients (56 ureters) treated with open Cohen approach from January 2008 to December 2011 were marked as Group 1 and 50 patients (58 ureters) treated with laparoscopic pneumovesical Cohen approach from January 2012 to December 2017 were marked as Group 2. The preoperative data, operative details, and follow-up outcomes were studied and compared between two groups to discuss the advantages of the laparoscopic pneumovesical approach. Statistical comparison was made with unpaired t-tests, χ2 tests, and Fisher exact probabilities, with P value <.05 was considered significant.
Results:
To bring less related effect during comparison, patients with similar preoperative data were selected. The time of operation of Group 2 was longer than that of Group 1, and the operation of Group 2 was completed with the laparoscopic pneumovesical approach in all but 1 patient (1 ureter), which was converted to open surgery. However, the postoperative gross hematuria duration, antibiotics consumption, retention time of urinary catheter, and hospital stay after surgery were shorter in Group 2 with less intraoperative blood loss, less postoperative complications, and less drainage catheter. All patients were followed up by ultrasonography, excretory retrograde urography, and magnetic resonance urogram for 3–24 months (mean 15.6 months) and the recovery and improvement were better in Group 2.
Conclusions:
Compared with open surgery, the laparoscopic pneumovesical approach has many benefits and was effective for the treatment of obstructive megaureter in children.
Introduction
Primary obstructive megaureter (OM) and vesicoureteral reflux (VUR) are the two most common anomalies affecting the vesicoureteral junction (VUJ), 1 and OM is mainly caused by VUJ obstruction (VUJO) in pediatric urology (such as VUJ stricture, ectopic ureter, and ureteroceles), which can lead to irreversible renal damage, if left untreated. Recent studies have demonstrated that the majority of children with congenital ureterovesical junction obstruction can be managed conservatively. 2 However, there are several reports indicating that conservative management has not been successful in children with Grades III and IV hydronephrosis, and ureteral diameter more than 1.33 cm. 3 Thus for VUJO, the only effective cure is surgical treatment in the form of ureteral reimplantation. 4 Of the numerous published techniques, the Cohen vesicoureteral reimplantation 5 has gained wide acceptance, and with the development of pediatric laparoscopic techniques, pneumovesical laparoscopic Cohen procedure, which copies the reliable open Cohen procedure in a carbon dioxide-insufflated bladder, has been applied in the treatment of VUR and VUJO. 4 In this article, we report our experience on the laparoscopic pneumovesical Cohen approach for VUJ stricture in children and make a comprehensive and detailed comparison with open Cohen procedure to discuss the advantages of this minimally invasive laparoscopic surgery.
Patients and Methods
Patient data
From January 2008 to December 2011, 48 cases (comprising 56 ureters) were diagnosed as VUJ stricture and were treated with open Cohen procedure, of which 26 were boys (54.2%) and 22 were girls (45.8%). Their mean age was 22.6 months (range from 5 to 80 months). Twenty-six cases were unilateral left sided (54.2%), 14 cases were unilateral right sided (29.2%), and 8 were bilateral (16.6%). These patients were marked as Group 1.
From January 2012, the pneumovesical laparoscopic Cohen procedure was used in our department, and by December 2017, 50 VUJ stricture cases (comprising 58 ureters) were treated and marked as Group 2, of whom 28 were boys (56%) and 22 were girls (44%). Their mean age was 24.1 months (range from 5.5 to 84 months). Twenty-seven cases were unilateral left sided (54%), 15 cases were unilateral right sided (30%), and 8 were bilateral (16%).
According to “Society for Fetal Urology grading system” and the grade of hydronephrosis, we divided all the cases into four grades. And also all the ureters were divided into four grades according to the ureteral diameter as described by Bi. 6 Detailed data of all patients are given in Table 1 and there was no statistical difference in all the indexes between these two groups.
Preoperative Patient Information of Pneumocystoscopy Group and Open Surgery Group
Society for Fetal Urology grading system was used.
SD, standard deviation.
Ultrasonography scans, excretory retrograde urography, and magnetic resonance urogram (MRU) were the main imaging techniques used to master the preoperative and postoperative ureteral diameter, degree of hydronephrosis, and recovery condition (Fig. 1A).

Surgical techniques
The open Cohen approach
A 4–5 cm transverse incision above the pubic symphysis along the ventral stripes was needed in the traditional open Cohen procedure and the bladder should be opened and exposed. An annular incision was performed along the ureter bladder mucosa, and a part of the distal ureter with 2–3 cm should be dragged into the bladder. Excisional tapering was needed to be performed if the ureteral diameter was >10 mm so as to make it <5 mm. A submucosal tunnel to the contralateral ureter should be separated with the length of 1.5–2.5 cm opening to the ureter orifice, from which the ureter was dragged. A suprapubic catheter, drainage tube, and urethral catheter were needed.
The pneumovesical laparoscopic Cohen approach
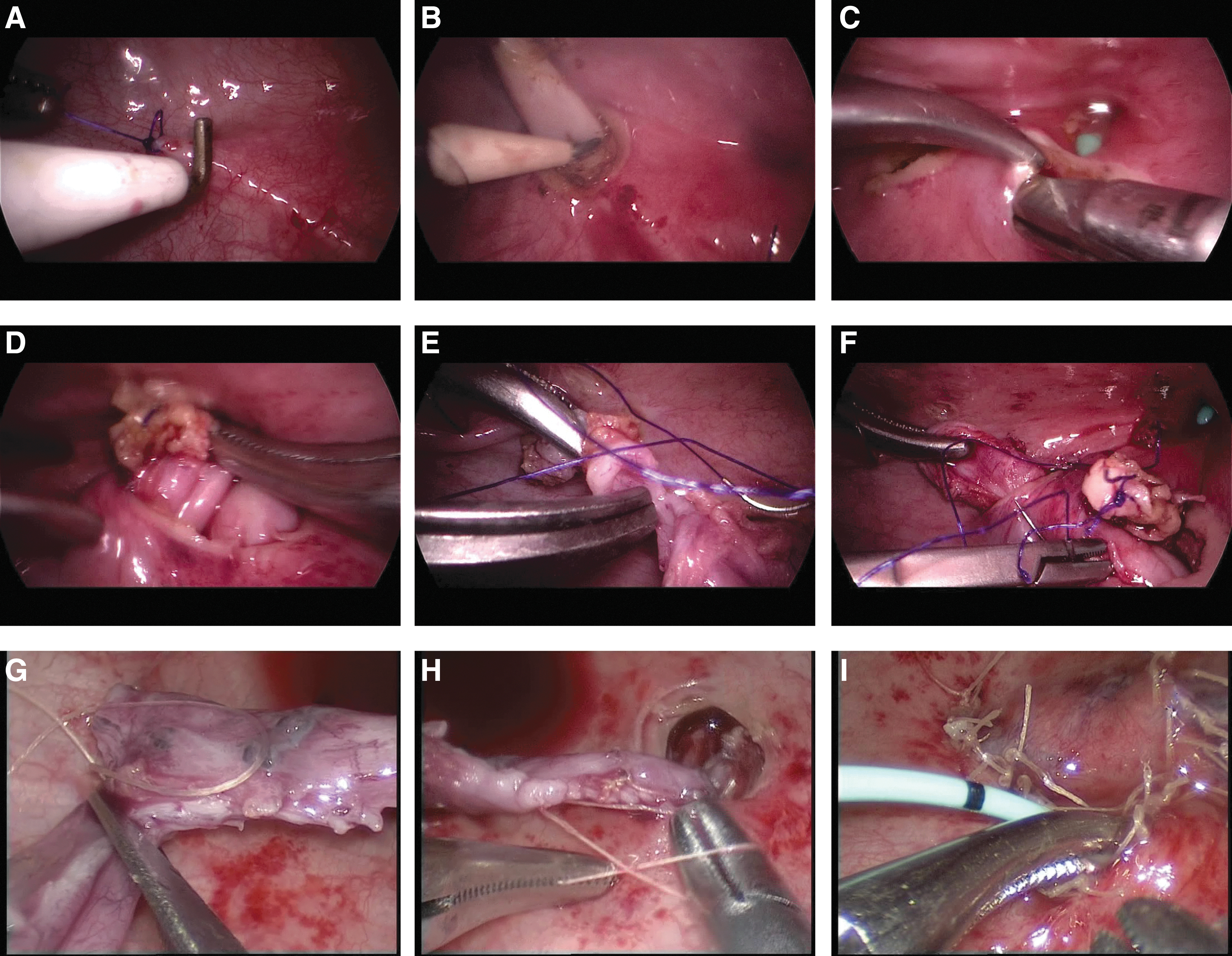
The surgical technique was mainly performed as described by C.K. Yeung 7 and the main operative key points were similar to those of the open approach. To begin the procedure, the bladder was first catheterized by a dual-lumen catheter and saline was used to distend the bladder. The three-port approach (5-mm ports in older and 3-mm ports in younger children) was performed. The first port was supraumbilical, by which pneumovesicum was created with carbon dioxide gas (the pressure was between 8 and 10 mmHg), and the other two working ports were inserted into the bladder at the level of the anteriorsuperior iliac spine after the saline was withdrawn through the dual-lumen catheter. The dual-lumen catheter was left in situ as a suction catheter. After the ureter was marked by a silk bladder, mucosa was annularly incised surround the ureteral orifice (Fig. 2A) and the proximal dissection was carried out by electrocautery until 3 to 5 cm distal ureter was dissected into the bladder (Fig. 2B). Then a submucosal tunnel with quadruple length of ureteral diameter was isolated from the ureter opening to the point 2 cm above the contralateral ureter (Fig. 2C), through which the ureter was dragged (Fig. 2D) and the abnormal distal ureter was cut off (Fig. 2E). The external wall of the ureter was interruptedly sutured by 6/0 absorbable suture with the surrounding mucosa (Fig. 2F). For ureteral dilatation >10 mm, excisional ureteral tapering was necessary and identical to open surgery suppported by the ureteral stent. Before tapering, the tip of the ureteral opening was sutured to the lateral bladder wall on the opposite side for better fixation and more precise excision (Fig. 2G). After tapering, the side of the ureter was closed by a running 5-0 absorbable suture (Fig. 2H). Then a Double-J tube was usually inserted for stenting (Fig. 2I) and was removed 2 months later by cystoscopy. For bilateral cases, one side of the ureter was opened through the submucosal tunnel to the top of the contralateral ureter, and the other side of the ureter was opened 1 cm outside of the contralateral ureter. Finally, indwelling catheter should be completed as a rule.
Statistical analysis
Statistical comparison was made with unpaired t-tests, χ 2 tests, and Fisher exact probabilities, with P value <.05 considered significant.
Results
All procedures were successfully completed and there was no death. One patient (one ureter) was converted to open surgery because of too small bladder volume.
For comparison of Group 1 and Group 2 during and after operation (Table 2), operative time of Group 2 was longer than that of Group 1 (P < .05) on unilateral cases (138.6 ± 14.7 versus 109.7 ± 17.2), but similar to bilateral cases (208.4 ± 27.2 versus 189.2 ± 21.8). Many other indexes of Group 2 were much better than those of Group 1 (P < .05), including intraoperative blood loss (3.8 ± 1.4 versus 15.4 ± 3.7), postoperative gross hematuria duration (2.21 ± 1.24 versus 4.11 ± 1.32), antibiotics consumption (7.15 ± 2.56 versus 13.33 ± 2.23), retention time of urinary tube (8.83 ± 1.73 versus 12.12 ± 1.96), rate of wound infection (1/49, 2% versus 3/49, 6.1%), rate of urinary extravasation (1/49, 2% versus 4/49, 8.2%), rate of urinary tract infection (0 versus 2/49, 4.1%), and hospital stay after surgery (7.1 ± 1.4 versus 11.3 ± 1.6). Also suprapubic catheter and drainage tube were not needed in pneumocystoscopy, which is different from open surgery.
Comparison of Pneumocystoscopy Group and Open Surgery Group During and After Operation
SD, standard deviation.
After follow-up by ultrasonography, excretory retrograde urography, and MRU for 3–24 months (Table 3 and Fig. 1B), the ureters complicated with VUR and anastomotic stricture in Group 2 patients were less than those of Group 1 patients (1/57, 1.8% versus 3/57, 5.2%; 1/57, 1.8% versus 4/57, 7%; both P < .05). The improvement rate of hydronephrosis (ratio of postoperative reduced Grade III/IV cases and preoperative Grade III/IV cases) was higher in Group 2 than in Group 1 (42/44, 95.5% versus 36/43, 83.7%, P < .05). There was no statistical difference in other follow-up indexes between these two groups such as grade of ureteral diameter and improvement rate of ureteral diameter (ratio of postoperative reduced Grade III/IV ureters and preoperative Grade III/IVureters).
Long-Term Follow-Up Comparison of Pneumocystoscopy Group and Open Surgery Group
Society for Fetal Urology grading system was used.
SD, standard deviation.
Discussion
Although Gill et al. 8 described endoscopic transvesical cross-trigonal Cohen ureteral reimplantation in 2001 after Atala et al. 9 first introduced laparoscopic extravesical reimplantation in a pig model, limited space within the bladder and bladder contraction during the operation represent big problems that disrupt the surgical field, until carbon dioxide pneumovesicum up to a limited pressure was introduced by Yeung et al., 7 which has the advantages of providing clear vision inside the bladder without disturbance from the fluid inside and no change on the body's physiology.4,10
In OM, the affected ureter is usually distended and tortuous, which poses a difficult task for dissection, especially if ureteroceles are complicated with extra time for dissection and reconstruction of the defective detrusor muscle is required. The traditional open Cohen procedure with disadvantages of severe wound, high blood loss, and long duration of hematuria has been replaced gradually by the laparoscopic pneumovesical Cohen approach. However, detailed comparison of operative details, recovery condition, and long-term follow-up condition between open and laparoscopic procedures is still limited in the literature.
Ninety-eight children (114 ureters) were involved in our series and treated by different approaches. MRU was used for the assessment instead of MAG3 to avoiding radiation. All the cases of Grade I and Grade II according to the ureteral diameter were suffering from recurrent urinary tract infection and needed operation to prevent the aggravation.
For surgical techniques, we summarized the following points: (1) the submucosal tunnel should be four times as long as the ureteral diameter to prevent bladder–ureter reflux. (2). Excisional ureteral tapering should be supported by the ureteral stent. (3) It should be done carefully and slowly when the operating instruments are in and out of the trocars in case of slippage of trocars.
By scientific analysis we found that the laparoscopic approach needed a little longer operative time for unilateral and ureterocele cases. For the bilateral cases, the operative time was similar to that of the open approach. Because once the operating space was set up by the pneumovesical approach, the laparoscopic operation and tissue exposure were much easiser than the open approach. The laparoscopic approach also had the advantages of less trauma (no open bladder, no suprapubic catheter), quicker postoperative recovery (shorter gross hematuria duration, shorter antibiotics consumption, and shorter hospital stay), and less postoperative complications (less wound infection, less urinary extravasation, less urinary tract infection, less VUR, and less anastomotic stricture). As we all know, bladder incision needs a suprapubic catheter, and the suprapubic catheter needs longer duration of antibiotics consumption and hospital stay, which could be avoided by the laparoscopic approach.
Besides these, improvement of hydronephrosis was also better and the improvement of ureteral diameter was similar to the open approach.
Therefore, the features of the laparoscopic pneumovesical Cohen approach could be concluded as follows: (1) carbon dioxide pneumovesicum provides clear vision inside the bladder without disturbance; (2) because the ureter was dragged through the submucosal tunnel and was interruptedly sutured with the surrounding mucosa, VUR could be prevented; and (3) new ureteral orifice was not anastomosed with bladder mucosa, which could prevent anastomotic stricture.
In our experience, laparoscopic transvesical ureteral reimplantation is suitable for OM. And we believe that in view of the incomparable advantages and development of laparoscopic techniques, more valuable experience will be obtained.
Conclusions
Compared with open surgery, the laparoscopic pneumovesical approach has many benefits and was effective for the treatment of OM in children. It should be considered as the preferred operative method for this disease.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.