
Abstract
Abstract
Purpose:
The study was performed to analyze the learning curve of performing uniportal video-assisted thoracoscopic surgery (uVATS) for lobectomy and lymphadenectomy, and to evaluate the possible disadvantages in outcomes during the course of learning.
Materials and Methods:
This is a prospective study of 52 consecutive patients undergoing uVATS lobectomy by a single surgeon from January 2016 to December 2017. Operation time (OPT) and the number of harvested lymph nodes (LNs) were evaluated by means of cumulative sum control chart by assessing efficiency (refinement in procedure to reach decreasing OPT and increasing number of harvested LNs) and mastery (absence of outliers). Failure rate, blood loss, and complications were retrospectively compared with the last 52 patients undergoing “classical” VATS lobectomy in the period before this study from January 2014 to December 2015.
Results:
Efficiency in OPT for uVATS was reached after 27 cases and mastery after 39 procedures (M1st = 172 ± 39 minutes; M2nd = 138 ± 34 minutes; p1–2 = 0.022; M3rd = 120 ± 25 minutes; p1–3 = 0.00; p2–3 = 0.65). Efficacy in the number of harvested LNs was reached after 26 cases and mastery after the 42nd procedure (MED1st = 17, IQR 12–19; M2nd = 21, IQR 16.25–29.75; p1–2 = 0.018; M3rd = 18, IQR 16–22; p1–3 = 0.004; p2–3 = 0.8). There were no significant differences in the failure rate (uVATS = 7.7%, VATS = 5.8%; P = .7), blood loss (MEDuVATS = 250 mL, IQR 200–387.5; MEDVATS = 225 mL, IQR 200–300; P = .77), and complications between the groups (uVATS = 13; 25%; VATS = 11; 21.2%; P = .41). Finally no significant differences could be found in OPT (uVATS = 151.36 ± 41.55; VATS = 156.69 ± 40.08; P = .52) or LNs (uVATS = 18, IQR 16–22; VATS = 19, IQR 14.25–20; P = .71) between the groups.
Conclusions:
Assuming a surgeon is skilled in “classic” VATS lung resections, achieving efficiency and mastery in uVATS is possible after sufficient experience even without dedicated education in this procedure, without measurable disadvantages throughout the course of learning. This study created a benchmark for already experienced VATS surgeons who are novices in uVATS, elucidating the number of operations required to reach both efficiency and mastery.
Introduction
The introduction of a new surgical method should be bounded with an analysis of the outcomes and also, if possible, an understanding of the learning curves.
Uniportal video-assisted thoracoscopic surgery (uVATS) for major lung resections has already been established as a valuable approach with results similar to those obtained in conventional three-port VATS. 1
One of the impediments for a wider acceptance might be insufficient financial resources preventing attendance at specialized uVATS courses and workshops, as well as employment of proctor supervisors. Even after successful attendance at a (hands-on) workshop, an absence of an uVATS experienced clinician in a novice's thoracic department might make implementation of this “acquired” knowledge difficult.
The aim of this retrospective cohort study is to analyze the learning curve, as well as outcomes for patients undergoing thoracoscopic lobectomy, by a single surgeon experienced in open surgery and conventional three-port VATS who is completely naive regarding uVATS.
Competence in various procedures has already been examined by means of cumulative sum (CUSUM) analysis,2–4 yet there is no published evidence for uVATS. With CUSUM analysis, one can continuously observe performance and identify improvement regarding a predefined level of accomplishment.
Materials and Methods
This is a single-center and single-surgeon retrospective cohort study involving patients undergoing lobectomy and systematic lymph node (LN) dissection by means of minimally invasive surgery. During the period from January 2016 to December 2017, a total of 52 consecutive lobectomies were performed by means of uVATS by a single surgeon previously unexperienced in this method. The surgeon had not attended any kind of dedicated education, but solely based on his prior surgical experience in thoracoscopic lung resections switched from the “classic” three ports to uniportal thoracoscopic approach.
Uniportal VATS was performed with an anterolateral single incision of 3–4 cm in the fourth or fifth intercostal space. Systematic LN dissection was performed in every case. An intercostal injection of 20 mL of 0.5% bupivacain was administered at three consecutive intercostal levels—at the level of incision as well as one above and one below, followed by placing a chest tube (24F) through the same incision before the closure.
Assuming the operating surgeon was already proficient in minimally invasive surgery such as VATs, the goals were to determine “efficiency” defined as refinement of the performance to reach decrement in mean operation time (OPT), and “mastery” defined as the point at which the operative time becomes consistent, without further changes in terms of mean operative time.5,6
The number of resected LNs was assessed in the same way with “efficiency” defined as improving performance to reach an increase of mean resected LNs and “mastery” defined as a point at which the number of removed LNs became consistent.
Both variables were analyzed by means of CUSUM.7,8
Frequency of complications, failure rate, defined as either conversion rate and/or a need for an extra incision, and blood loss were statistically analyzed and together with the number of removed LNs and operative time, compared with those extracted from the last 52 patients undergoing lobectomies by means of “classic” three ports approach (VATS group) by the same surgeon in the period before use of uVATS. Moreover, the same variables extracted solely from the cases in the first phase (first 27 procedures) of the learning curve were also compared with the VATS group to understand potential untoward patient outcomes in the very beginning of the learning curve.
Comparisons of the variables by means of methods of inferential statistics with bootstrap analysis having 1000 samples and using Mersenne Twister random number generator were conducted in IBM SPSS Statistics v.23. and Minitab v17.
Ethical committee on human research of the Heidelberg University approved the evaluation of the data in anonymous manner (S-331/2018).
Results
Operative time was defined as time from skin incision to skin closure. Operative time was assessed by means of CUSUM curve to estimate efficiency and mastery.
Basic CUSUM curve for the length of uVATS operations (Fig. 1) shows clearly the first point of interest “efficiency,” which was reached at the 28th operation.
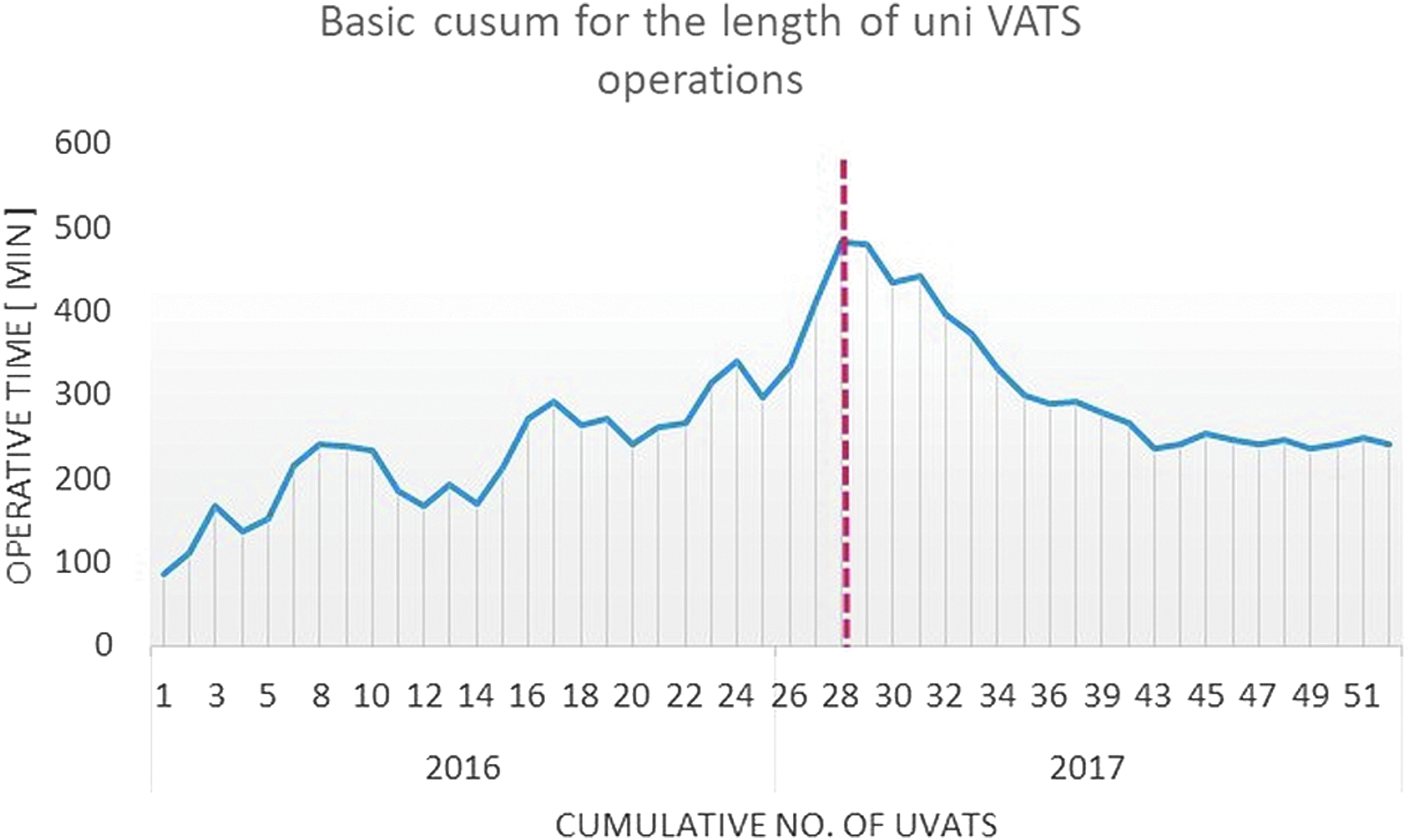
Basic CUSUM curve for the length of uVATS operations. CUSUM, cumulative sum.
“Mastery” was reached after 39 cases. Operative time, evaluated by one-way analysis of variance with post hoc Bonferroni test, showed significant differences between first (1–27 cases) and second (28–39 cases) as well as first and third phases (40–52 cases), but not between second and third phases (M1st = 172 ± 39 minutes; M2nd = 138 ± 34 minutes; p1–2 = 0.022; M3rd = 120 ± 25 minutes; p1–3 = 0.00; p2–3 = 0.65) (Fig. 2).
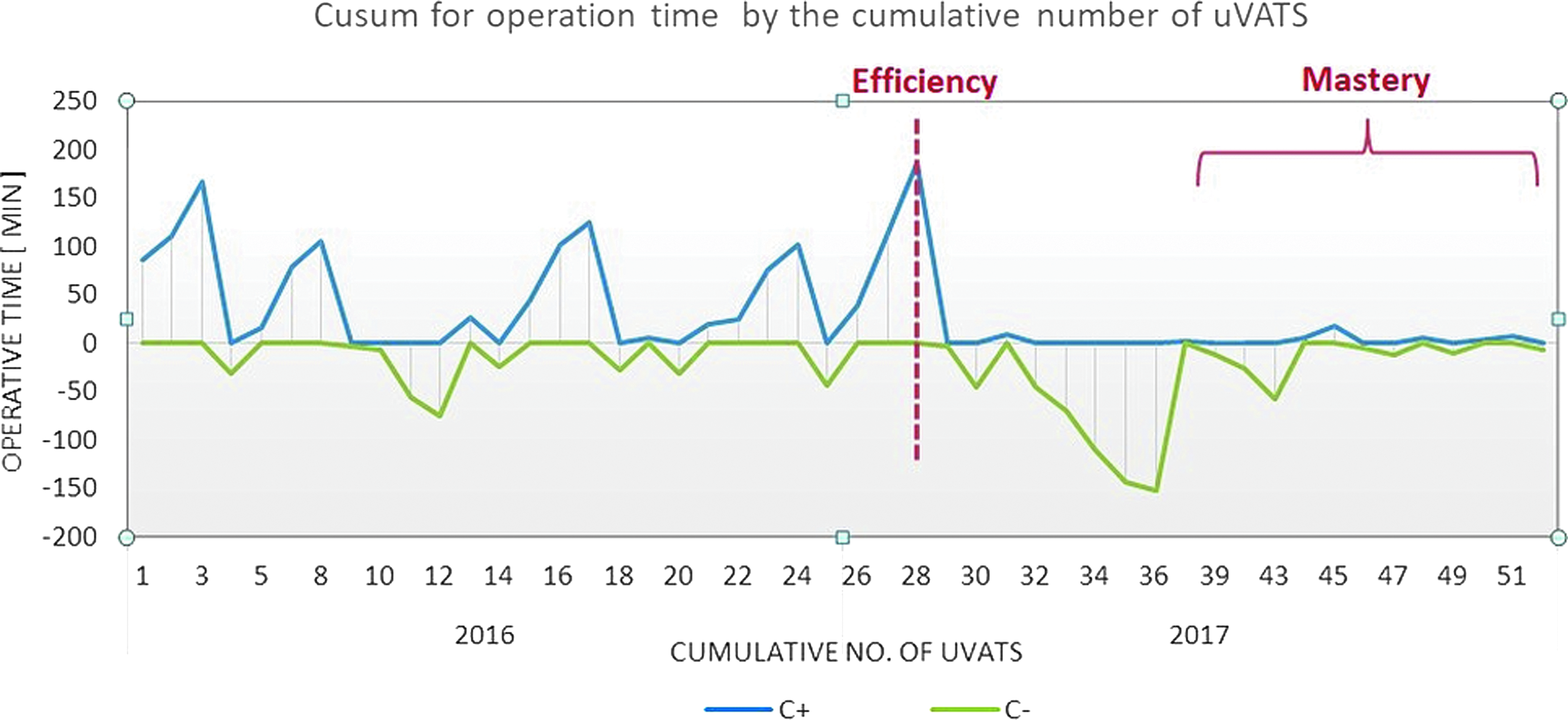
CUSUM for the time of surgery by the cumulative number of uVATS x axis—average time of operation; C+(blue line)—OPT above average; C− (green line)—OPT below average. OPT, operation time; CUSUM, cumulative sum.
The number of harvested LNs rose with experience, reaching the efficiency level at the 26th operation (1st phase 1–26 cases). After that point, the median number of resected LNs became higher than average overall (Fig. 3), reaching the level of mastery after the 42nd operation (2nd phase 27–41, 3rd phase 42–52 cases). The median number of resected LNs (IQR), evaluated by Kruskal–Wallis, as well as with Mann–Whitney test, showed significant differences between the phases (MED1st = 17, IQR 12–19; M2nd = 21, IQR 16.25–29.75; p1–2 = 0.018; M3rd = 18, IQR 16–22; p1–3 = 0.004; p2–3 = 0.8).

CUSUM for the number of removed LNs by the cumulative number of uVATS x axis—median number of harvested LNs; C+(blue line)—the number of harvested LNs above median; C− (green line)—the number of harvested LNs below median. LNs, lymph nodes; CUSUM, cumulative sum.
Preoperative patient variables observed at both uVATS and VATS groups are presented in Table 1. Five patients from uVATS group and 7 from VATS group underwent preoperative neoadjuvant chemotherapy (P = .38), whereas 1 in each group underwent preoperative radiation as well (P = 1).
Baseline Characteristics of the Groups a
According to the results of an unpaired t-test, there is a significant difference on a level of 0.05, confirmed by the 95% bootstrap confidence interval (if the interval does not contain 0, the result is statistically significant).
ACCI, adjusted Charlson's comorbidity score; BMI, body mass index; DLCO, diffusion capacity for carbon monoxide; FEV1, forced expiratory volume in 1st second; FEV1/VC, Tiffeneau index; SD, standard deviation; uVATS, uniportal video-assisted thoracoscopic surgery; VATS, video-assisted thoracoscopic surgery.
Operative data of both uVATS and VATS groups are presented in Table 2, showing, in particular, no significant differences in any variables. Failure rate was similar, having three conversions in VATS group (one for bleeding and two for technical reasons) and four in the uVATS group: three conversions (two for technical reasons, one for stapler failure), and one due to establishing an extra port (uVATS = 7.7%; VATS = 5.8%; P = .7).
Peri- and Postoperative Data a
According to the results of an unpaired t-test, there is a significant difference on a level of 0.05, confirmed by the 95% bootstrap confidence interval (if the interval does not contain 0, the result is statistically significant).
LNs, lymph nodes; OPT, operation time (skin incision to skin closure); pT, pathological size of the tumor; SD, standard deviation; uVATS, uniportal video-assisted thoracoscopic surgery; VATS, video-assisted thoracoscopic surgery.
Complications are detailed in Table 3. There were no significant differences in complications between the groups (uVATS = 14, 27%; VATS = 14, 27%; P = 1).
Complications in the Cohort
Dx, diagnosis; AKIN, acute kidney injury; LE, pulmonary embolism; NSTEMI, non-ST elevation myocardial infarction; STEMI, ST elevation myocardial infarction; PAL, prolonged air leak (>5days); uVATS, uniportal video-assisted thoracoscopic surgery; VATS, video-assisted thoracoscopic surgery.
When comparing only the 1st phase (first 27 patients) of the uVATS group with the whole VATS group, no significant differences could be found either preoperatively, perioperatively, or in short-term outcomes (Table 4).
Comparison Between Phase 1 of the uVATS Group and VATS Group
Median values were used, instead of mean.
DLCO, diffusion capacity for carbon monoxide; FEV1, forced expiratory volume in 1st second; FEV1/VC, Tiffeneau index; LNs, lymph nodes; OPT, operation time; SD, standard deviation; uVATS, uniportal video-assisted thoracoscopic surgery; VATS, video-assisted thoracoscopic surgery.
Comparison of the complications rate and failure rates by means of Fisher's test yielded the statistically nonsignificant results (uVATSphase1 = 9, 33%; VATSall = 14, 27%; P = .61) and (uVATSphase1 = 4, 14.8%; VATSall = 3, 5.8%; P = .22), respectively.
Discussion
The aim of this study was to present a single-operator learning curve for uVATS, with no previous experience and/or dedicated education specific to uVATS.
Based on CUSUM analysis, after 27 uniportal VATS lobectomies with average time of 172 minutes, the efficiency point was reached. After 12 additional cases (with average of 138 minutes), the mastery point was reached. That is, at the 39th case, the average OPT decreased to 120 minutes and minimum variations in operative time were recorded for the next 13 cases.
This finding was supported with CUSUM analysis of the number of harvested LNs by achieving efficiency point after 26 cases and mastery after the 42nd operation.
Compared with the previous 52 VATS consecutive cases performed in 2015 and 2014, there was no significant difference in complication rate, failure rate, or blood loss even for the first phase in the learning curve (first 27 cases).
The vast majority of thoracic surgeons who consider themselves proficient in terms of VATS lobectomy found VATS courses, fellowships, and animal laboratories much less beneficial than the training in their thoracic residencies. 9
If training for uniportal VATS is not included in thoracic residency programs, we see by this single-operator experience that it is feasible to start learning the uniportal method after training proficiency is reached in minimally invasive thoracic surgery in the residency program. In this case, self-training alone demonstrated an appropriate learning curve, mimicking the learning curve of VATS. In fact, uVATS learning curve may be even observed, to certain extent, as an elongation of the VATS curve.
Our study has several limitations. Having only 1 surgeon already experienced in minimally invasive surgery makes generalizability potentially prone to underestimation of the threshold for primary measured outcomes efficiency and mastery. Moreover, as a retrospective study, a selection bias cannot be avoided.
However, the use of a CUSUM analysis with a single-surgeon experience limited variations due to differences among surgeons, which allowed for a cleaner picture of learning curves to achieve efficiency and mastery. Indeed this analysis could be used as a benchmark for future training programs.
Conclusion
Assuming a surgeon is skilled in “classic” VATS lung resections, achieving efficiency and mastery in uVATS is possible after sufficient experience even without dedicated education in this procedure and without measurable disadvantage even for the initial patients throughout the course of learning. This study established a benchmark for the number of operations to reach both the level of efficiency and mastery when transitioning from VATS to uVATS procedures.
Footnotes
Acknowledgments
I am deeply thankful to Mrs. Peggy McLaughlin for her contribution in editing this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
No competing financial interests exist.