
Abstract
Abstract
Background:
Traditionally, a laparoscopic approach is used for treatment of congenital hypertrophic pyloric stenosis (CHPS) in newborns and infants. The novel technique–Gastric Per Oral Endoscopic Myotomy (G-POEM) had been proposed as an alternative method. G-POEM is a procedure that is recently being used for treatment of gastroparesis in adults. For the first time, in this study, we demonstrate the performance of G-POEM in an infant and its short-term results.
Materials and Methods:
G-POEM was performed in the Center of Newborn Surgery in Irkutsk (Russia) in August 2018 for a 1-month-old infant, whose weight was 4,200 g. The patient had vomiting for 5 days before admission and a slight deficiency of body weight. The diagnosis of CHPS was confirmed by ultrasound examination of the abdominal cavity. The pyloric muscle thickness was 7 mm. The operative technique of the performed G-POEM was carried out by creation of a submucosal tunnel with a distance of 4 cm toward the pylorus and dissection of the hypertrophied muscle layer in a form of the Ramstedt's incision by using an electrocautery knife. At the end of the procedure, the mucosal membrane incision was closed by special clamps.
Results:
The operating time was 65 minutes. There were no intraoperative complications such as bleeding and/or mucosal perforation. The patient began to eat 6 hours after the procedure. The transition time to full enteral nutrition was 24 hours. The infant was discharged from the hospital the next day in good condition. We did not observe early or late postoperative complications such as recurrence of pyloric stenosis and incomplete myotomy during postoperative observation. There were not even minimal scars on the patient's body.
Conclusions:
G-POEM is a technically feasible, safe, and successful procedure for treatment of CHPS in newborns and infants. An additional study is needed to perform the comparison between this technique and laparoscopic pyloromyotomy.
Introduction
More than 100
During the time of its existence, the submucosal pyloromyotomy practically has not changed, except transformation of surgical access from an open laparotomy to a laparoscopic procedure. 3 This disease continues to fascinate and to excite pediatric surgeons, forcing many of them to look for alternative treatments, such as a single-port laparoscopic surgery hoping to find even a less invasive procedure than the current ones. 4
Recently, scientific discoveries have appeared in visceral surgery of adults, which clearly changed the course for development of modern gastroenterology. In 2008, Haruhiro Inoue, a Japanese surgeon, offered Per Oral Endoscopic Myotomy (POEM) as an alternative to Heller's laparoscopic myotomy. 5 POEM quickly gained popularity among adults gastrointestinal surgeons all over the world and demonstrated results comparable with the classical open myotomy, herewith possessing important qualities such as reduced postoperative pain and lack of scars. At the present time, the principle of endoscopic submucosal tunnel dissection (ESTD) has been extended to other parts of the digestive tract. In 2013, Khashab et al. reported the use of Gastric POEM (G-POEM) for treatment of gastric paresis in adult patients. 6 In this report, we demonstrate the first experience with G-POEM in a 1-month-old infant with CHPS.
Materials and Methods
The patient, a 1-month-old infant, with diagnosis of CHPS, was treated in the Center of Newborn Surgery in Irkutsk in August 2018. The patient's gestational age was 40 weeks. Weight at the time of birth was 3,600 g. This newborn was sick for 5 days and on admission he had a body weight of 4,200 g. The infant was 100 g underweight. The diagnosis of pyloric stenosis was confirmed by ultrasound examination of the abdominal cavity. The pyloric muscle thickness was 7 mm, with a length of 20 mm.
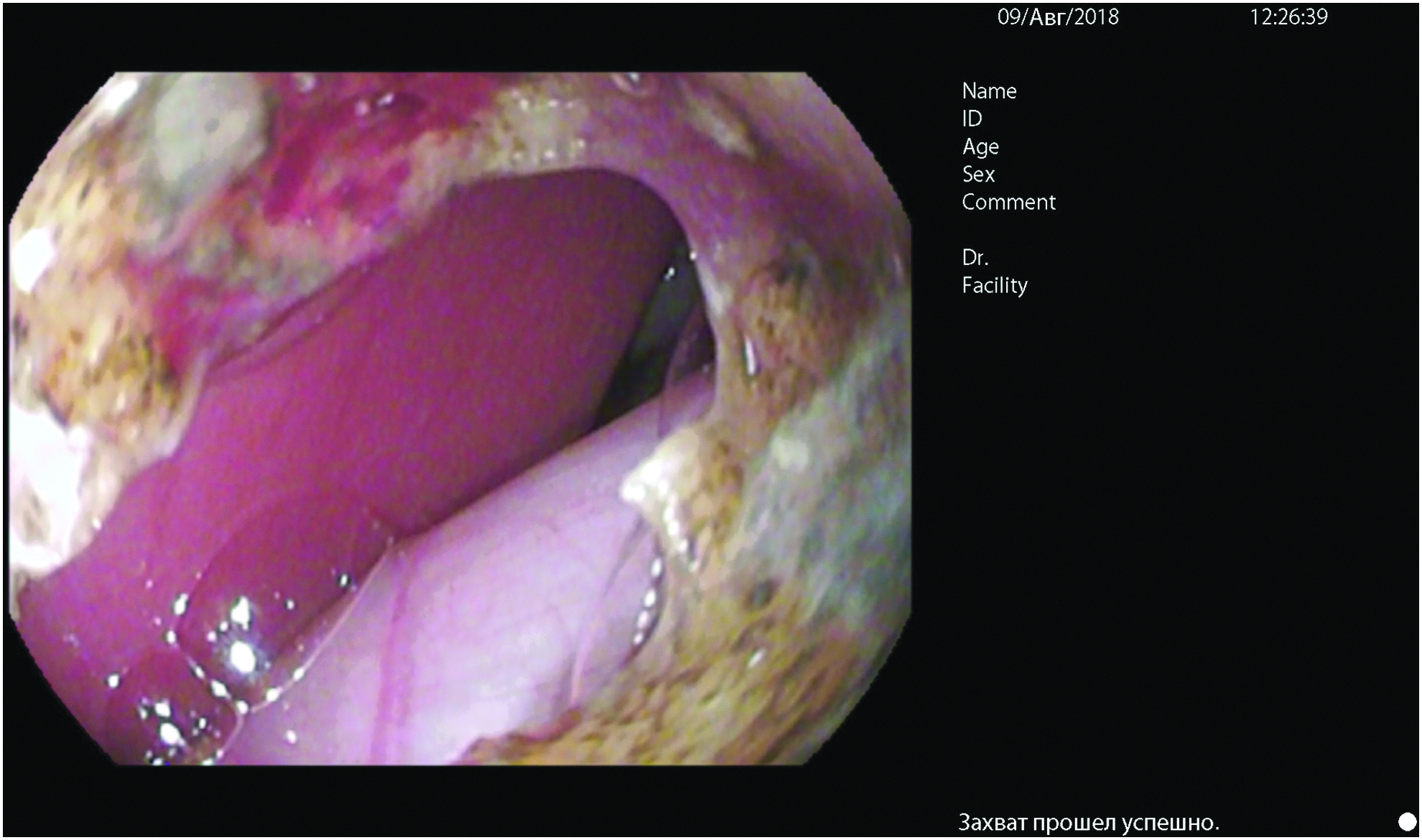
The infant underwent G-POEM. The technique of G-POEM and Esophageal-POEM is the same and consists of submucosal injection, incision of the mucosa, creation of a submucosal tunnel, myotomy, and closing of the mucosa. The procedure was performed under general anesthesia with tracheal intubation. The patient was placed on an operating table in a supine position. Pentax EG 16-K10 gastroscope with diameter of 5.4 mm and instrument channel diameter of 2.0 mm was used for peroral pyloromyotomy. Before the operation, remnants of infant formula and saliva were removed from the stomach by irrigation and aspiration. The pyloric canal was closed and did not open upon carbon dioxide (CO2) insufflation (Fig. 1).
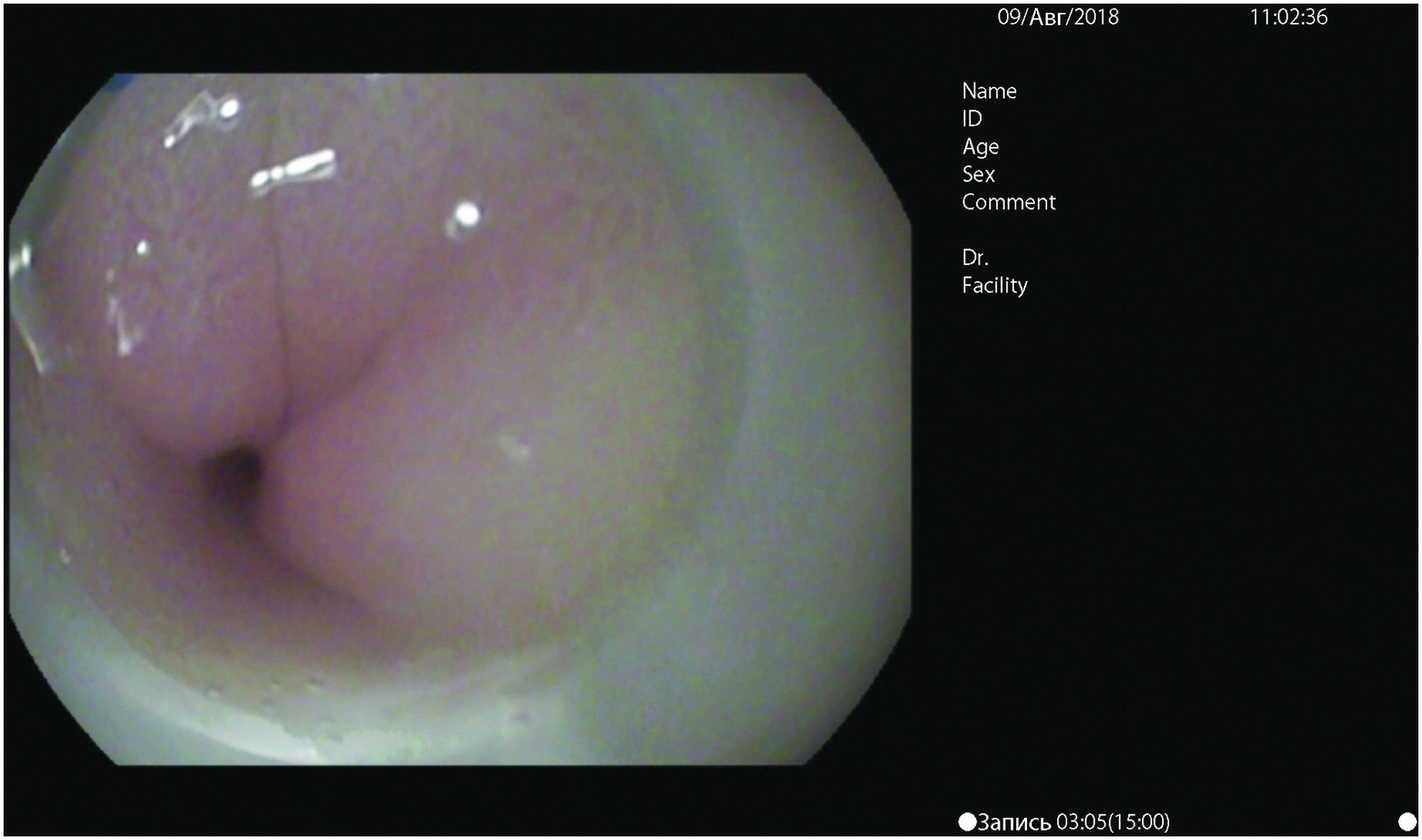
Pyloric canal before surgery.
CO2 insufflation was used during the procedure to minimize effect of pneumoperitoneum in case the peritoneum would be damaged and CO2 would enter into the abdominal cavity. A transparent cap, placed on an endoscope's end, was used for improvement of the image. Subsequently, submucosal injection of 3 mL of hypertonic saline solution mixed with 0.25% indigo carmine was made in an area of the greater curvature with a distance of 4 cm toward the pylorus (Fig. 2).
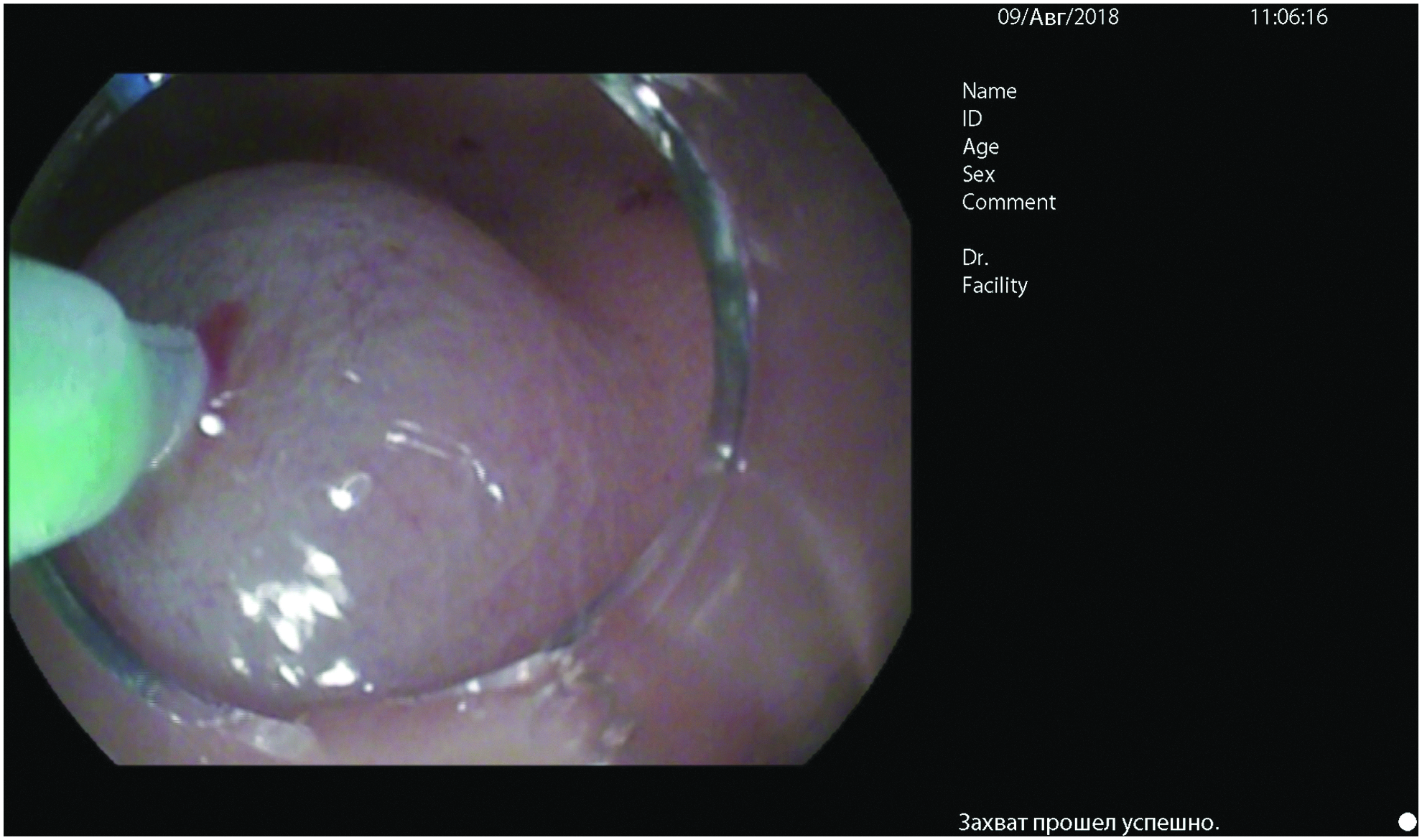
Submucosal injection of saline solution.
Like in a classic POEM, a mucosal incision about 8 mm long was performed at the site of the initial submucosal injection by using an Endoscopic Needle-Knife (Fig. 3).
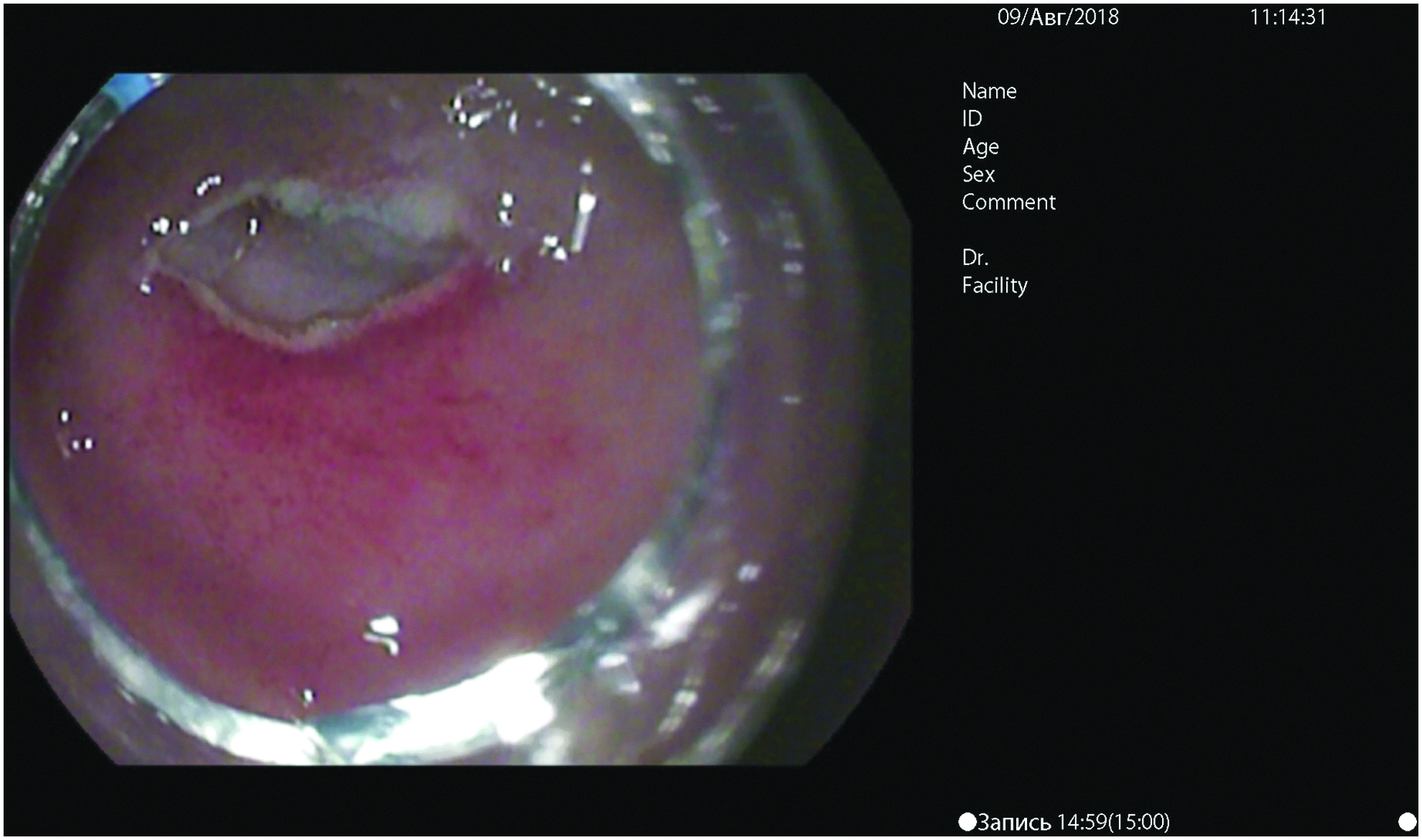
Dissection of gastric mucosa.
The initial electrosurgical mode (Setting 1) on the Electro Surgical Unit ERBE VIO® 300D (ERBE, Tübingen, Germany) was EndoCut® with preload parameters (2:3:3). After incision of the gastric mucosa, the endoscope was inserted into the submucosal layer. Initially, placement of an optical system into the submucosal layer could create difficulties, however, this should not be rushed to prevent bleeding or rupture of the mucous membrane, which would impede subsequent actions. After injection of additional fluid, a submucosal tunnel (Fig. 4) was created toward the pylorus by using the same electrosurgical mode Setting 1 or Setting 2—Soft Coagulation (Effect 2, Power40 Watts).
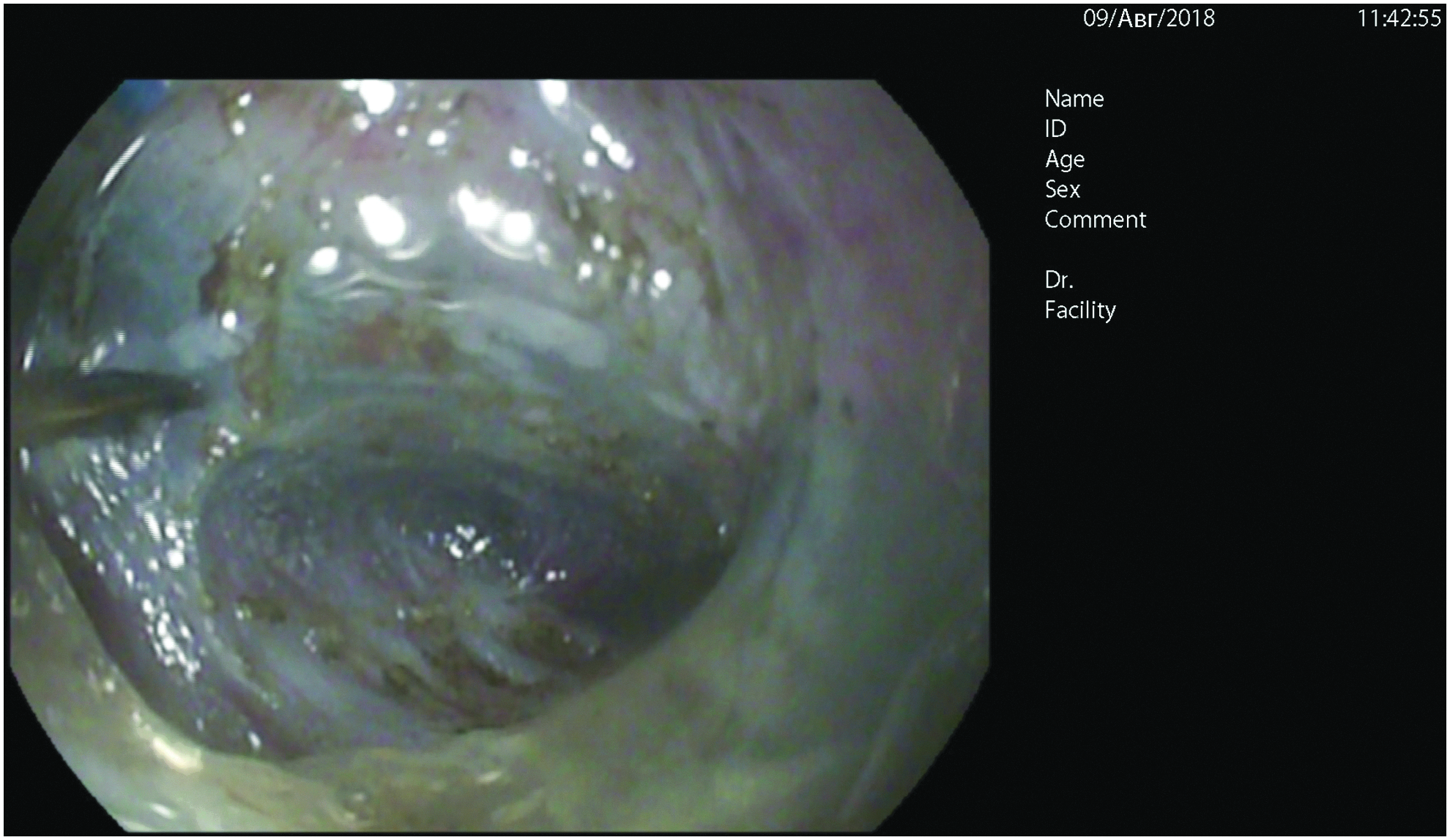
Creation of submucosal tunnel.
For safe and fast tunneling and for prevention of mucous membrane injury, an injection of a sufficient volume of solution was made, same like in POEM. Unlike tunneling in the esophagus, determination of the correct direction for a tunnel formation is not easy, and it may take several attempts to exit the tunnel and reenter it to recognize contours of the submucosal canal. The pyloric sphincter was identified as a whitish, dense bundle of circular muscle fibers. Myotomy was performed in the antegrade direction throughout entire length of the hypertrophied pylorus, on the length of 20 mm that was determined by ultrasound examination before the procedure (Fig. 5).

Dissection of pyloric circular muscle fibers.
To avoid injury of the longitudinal fibers or the visceral peritoneum, a pylorus muscle incision was limited by internal circular fibers. However, the margin was sufficiently thin. As a result, an incision was made through the entire thickness of the muscle layer (Fig. 6).
Complete dissection of pyloric muscle layer.
Then, the Pentax EG 16-K10™ gastroscope was replaced with a Pentax EG 29-i10™ gastroscope with a larger instrument channel with a diameter of 3.2 mm. Clips were applied to the edges of the gastric mucosal incision (Fig. 7). After the closing of the mucosal membrane opening, visualization of the enlarged lumen of the pyloric canal demonstrated the effectiveness of performed pyloromyotomy (Fig. 8).
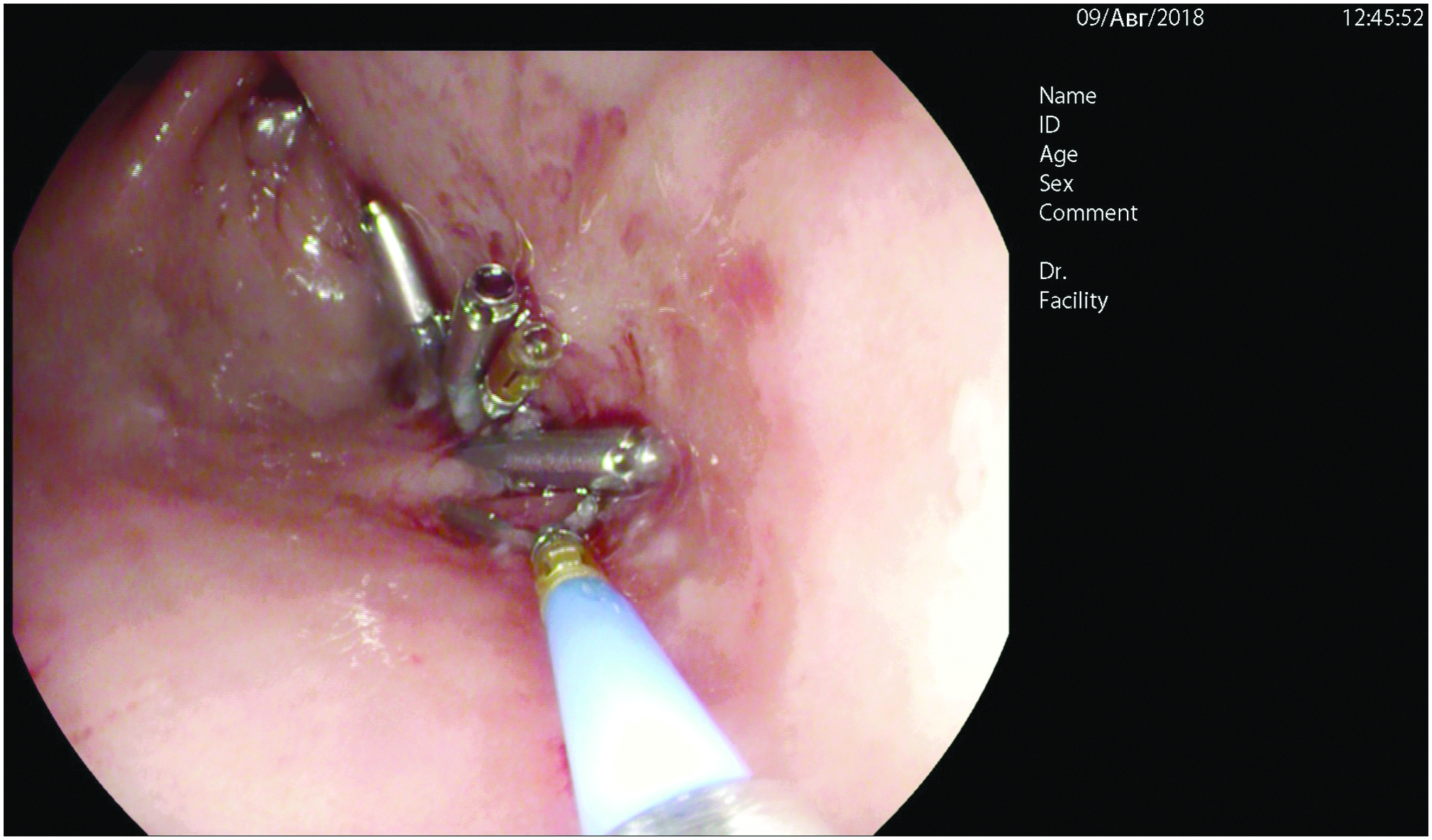
Closing of gastric mucosal incision by applying clips.

View of pylorus after performed G-POEM. G-POEM, Gastric Per Oral Endoscopic Myotomy.
Results
The operating time of the G-POEM was 65 minutes. There were no intraoperative complications such as bleeding and mucosal perforation. We did not identify adverse cardiorespiratory effects of this procedure on the infant. Normal rates of gas exchange and hemodynamic indicators were recorded during the procedure. The patient began to eat 6 hours after surgery. The transition time to full enteral nutrition was 24 hours. The patient was discharged from the hospital on the next postoperative day in good condition. During postoperative follow-up, we did not register early or late postoperative complications such as recurrence of pyloric stenosis and incomplete myotomy. There were not even minimal scars on the infant's body.
Discussion
For a long time, open laparotomy was the “gold standard” for operations performing on abdominal organs in children. But complications such as wound infection, ventral hernia, adhesions, postoperative pain, and slow recovery paved the way to laparoscopic operations. At the beginning of the 21-st century, laparoscopic procedures already had an advantage over open laparotomy, since the level of postoperative complications was much lower. However, even laparoscopic operations were not devoid from complications. But the novel endoscopic procedures, unlike laparoscopic operations, have a very low or almost zero complication rate.
A desire to perform any operation without a visible incision has always led to advanced surgeries. These expectations were partially fulfilled with the appearance of Natural Orifice Transluminal Endoscopic Surgery (NOTES). This method allows access to the abdominal organs through natural openings (oral cavity or rectum) without passing through the anterior abdominal wall and combines the skills in endoscopy, gastroenterology, and minimally invasive surgery. One of the major progresses in NOTES was the use of the ESTD technology, which allows surgeons to separate an entry to a tunnel into mucosal membrane and a place of manipulation, which prevents development of surgical infection. 7 This technique was quickly propagated and began to be used for treatment, including achalasia (POEM) 5 and gastroparesis (G-POEM). 6 Submucosal myotomy is the basic principle of these operations. However, widespread of submucosal myotomy in the pediatric population did not occur due to the rarity of these pathological conditions in children.
However, another disease–congenital pyloric stenosis, which is commonly treated with myotomy, is quite common in infants. The frequency of CHPS varies in the different geographic regions. The incidence rate of CHPS in the countries of Southeast Asia and China is 0.5 cases per 1000 newborns, while in the United States and in Europe the rate of CHPS is four times higher and consists from 2 to 4 cases per 1000 newborns.8–12 The main pathological element in occurrence for CHPS is fairly a fast development (during several days) of hypertrophy of the pyloric muscular layer, which leads to a gradual obstruction of its channel. 13 The etiology of muscle hypertrophy development, despite the large amount of scientific research, remains unknown.
The evolution of open surgical approach of CHPS underwent several stages: vertical midline incision, subcostal incision, 14 transverse laparotomy with dissection of the m. rectus abdominis, 15 cross-axillary incision with dissection of the muscular layer, 16 and umbilical incision 17 with preserving of the principle–nonmucosal dissection of the muscle layer of the pylorus, proposed by Ramstedt. 1
The introduction of endosurgical technology for treatment of CHPS was made possible thanks to Alain et al., 3 who published the first experience of laparoscopic pyloromyotomy in 10 children in 1991. Then, the operation technique was improved and detailed by Rothenberg. 2 The introduction of a single-port laparoscopic approach was an evolutionary step in treatment of CHPS. The first experience of using a single-port pyloromyotomy belongs to groups of surgeons from children's hospitals in Alabama and in Irkutsk (Russia).4,18–21
More than 25 years have passed since the first laparoscopic pyloromyotomy was performed. The potential benefits of laparoscopic pyloromyotomy have been described as shorter hospital stays, more rapid postoperative recovery, and improved cosmetic results.3,22–25
To prove that laparoscopic surgery is the best operating technique from the point of postoperative complications, Oomen et al. summarized the results of a randomized series devoted to comparison of endoscopic and open surgeries in hypertrophic pyloric stenosis, mainly focusing on complications such as perforated mucosa and inadequate myotomy, which required the surgical interventions to be redone. 26 The results of comparison did not show clear benefit of a laparoscopic procedure over an open operation. According to various authors, intraoperative injuries of mucous membrane during pyloromyotomy occur in about 3.7%–5% of cases.27,28
Also, many authors demonstrate a high failure rate in laparoscopic treatment of CHPS. There is no direct tactile contact with the enlarged pylorus in a laparoscopic procedure. As a result, assessment of the margins of the hypertrophy is difficult. According to Yagmurlu et al., incomplete myotomy was recorded in 2.2% of patients in a laparoscopic pyloromyotomy group, while in an open treatment group, successful dissection was achieved in 100% of cases. 29 Thus, during the long-term experience of laparoscopic surgeries of CHPS, it is clear that laparoscopic pyloromyotomy has advantages only with improved cosmetic results.
The idea to perform an endoscopic pyloromyotomy with creation of ESTD in patients with CHPS appeared in the authors of this study during observation of POEM, which was used in our hospital in teenagers with achalasia of the esophagus. The dominant factor of the pathological process—a narrowing of the lumen of the esophagus as a result of a prolonged contraction and hypertrophy of the muscle layer is common in these two diseases.
The research in literature has shown that recently endoscopic pyloromyotomy has been used for treatment of diabetic gastroparesis in adult patients. This operation is called G-POEM. Technically, G-POEM differs a little from esophageal POEM and consists in dissecting of circular muscle fibers that limit patency of the esophagus and stomach. G-POEM is more attractive for patients.
Peroral endoscopic procedure is a minimally invasive operation without incisions on the abdominal wall. This is a less painful surgery. Also, it is not accompanied by hemodynamic and respiratory effects on the child, which arise during CO2 insufflation.
Conclusion
This case report is the first performance of G-POEM for treatment of CHPS in infants. The study demonstrated that transfer from adult's surgery of the ESTD technology and submucosal pyloromyotomy is possible in pediatric patients of early age. The technical aspects of creation of a submucosal tunnel, dissection of the pyloric muscular layer, and closing of a mucosal incision require further discussion.
G-POEM is a technically feasible, safe, and successful procedure for treatment of CHPS in newborns and infants. An additional study is needed to perform a comparison between this technique and a laparoscopic pyloromyotomy.
Footnotes
Disclosure Statement
No competing financial interests exist.