
Abstract
Abstract
Background:
Congenital nonparasitic liver cysts in newborns are rare. Surgical excision of these formations is necessary to prevent complications. Reports of laparoscopic treatment of simple liver cysts in children are sporadic. We present a series of 3 patients with liver cysts treated laparoscopically in a single center. We added a short review of the literature.
Methods:
Data of 3 patients with nonparasitic liver cysts were collected at our center, from 2014 to 2019. Early and long-term results of laparoscopic operations were studied.
Results:
All patients were newborns, and of these, 2 were girls and 1 boy. The primary diagnosis was established during prenatal ultrasound examination. The laparoscopic approach was used in all patients. Complete resection of the cysts was achieved laparoscopically in all cases. Pathology reports were consistent with nonparasitic liver cysts. The early postoperative period was uneventful with prompt discharge. In the long-term follow-up period, there were no recurrences of the disease.
Conclusions:
The study presents one of the largest series of laparoscopic excision of nonparasitic liver cysts in newborns. We conclude that laparoscopy is a safe and effective method of treating of congenital hepatic cysts.
Introduction
Congenital hepatic cysts are rarely diagnosed in adult patients and are extremely rare in the pediatric population.1–4 Due to advances in antenatal diagnosis, this anomaly is diagnosed much earlier nowadays. 3 Surgical treatment is indicated in all patients to prevent complications and exclude the possibility of malignancy of cysts. Since 2006, 5 complete removal of a liver cyst is indicated as soon as safely feasible, as malignancy has been reported to develop in these cysts.
In previous times, enucleation of such cysts was performed via laparotomy with its consequent morbidity. Since the advent of minimally invasive surgery, including the pediatric population, the laparoscopic approach has widely replaced the open one in these cases.4,6,7 Since this anomaly is exceedingly rare, reports of the use of minimally invasive approach in the pediatric patient population are sporadic.
In this study, we present a group of patients consisting of 3 newborns who have successfully underwent a complete laparoscopic resection of a congenital nonparasitic hepatic cyst. We also reviewed the literature on epidemiology, origin, diagnosis, and treatment options for congenital liver cysts in children.
Materials and Methods
The case records of the 3 patients with nonparasitic liver cysts who were treated at the Newborn Surgery Center of Irkutsk were collected over time since 2014. The only criterion for inclusion of patients in the study was diagnosis of nonparasitic liver cyst. The initial diagnosis was based on prenatal ultrasound investigation findings. All patients underwent computed tomography (CT) (Fig. 1) before the surgery.

Computed tomography of the abdominal cavity—congenital nonparasitic cyst of the liver segment V (indicated by an arrow).
The operative technique used four laparoscopic ports, one of which was placed in a transumbilical way and served for insertion of the optical system into the abdominal cavity. Two other laparoscopic ports were set to the left and right of the optical system so that the principle of triangulation was adhered and used for the introduction of 3 mm instruments into the abdominal cavity. The fourth port was subcostal on the right and was intended for the liver retraction.
After inspecting and determining the cyst location in relation to the surrounding tissues, puncture and emptying of the cyst was carried out (Fig. 2). Complete resection of cyst membranes was performed with bipolar coagulation (Fig. 3). Plasma coagulation in the gas medium of argon of liver tissue in the area of the cyst bed was performed at the final stage of surgery (Fig. 4).

Appearance of congenital nonparasitic cyst of the liver segment V.
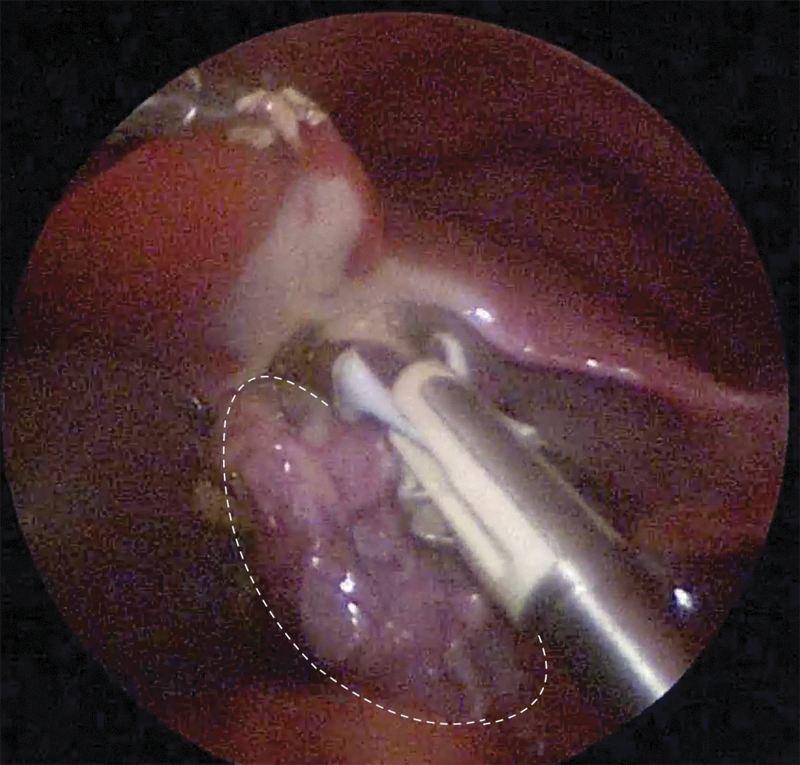
Enucleation of congenital nonparasitic cysts of the liver segment V.
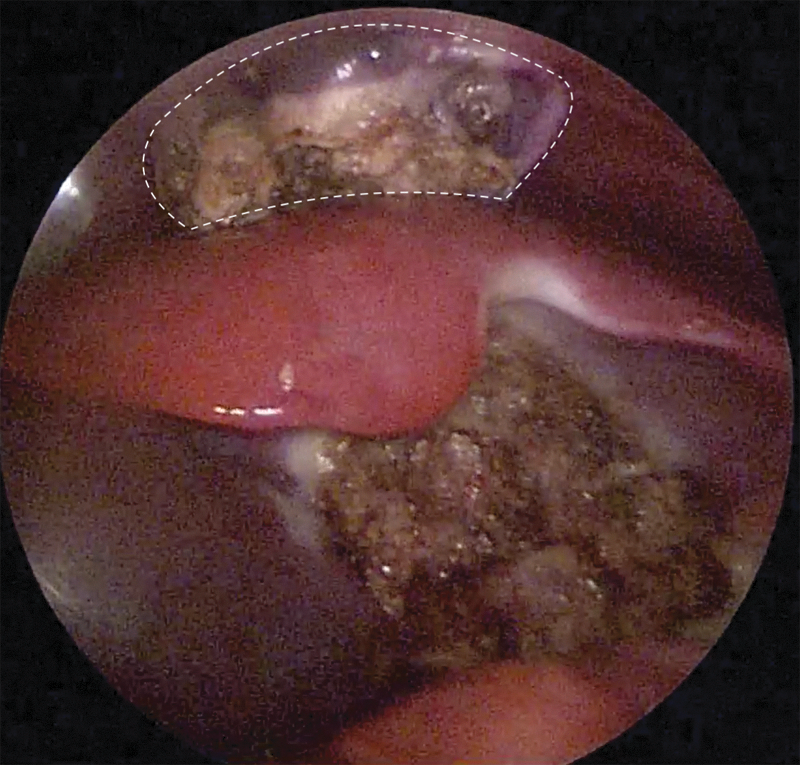
View of the liver after cyst removal.
On the next day after the surgery, ultrasound examination of the liver was performed. Depending on the clinical condition of the patient and ultrasound results, discharge was planned.
Results
Case no. 1
A newborn boy aged 2 weeks was admitted to the surgical center with complaints of malnutrition and mass lesion palpable in the right half of the abdomen under the liver. The prenatal screening showed that the child had a cyst in the projection of the lower edge of the liver. Ultrasound investigation found a cystic tumor that presumably was a cyst of common bile duct. CT showed that it was a cyst of the liver, its size being 5–6 cm. The hepatic cyst was localized in segment V of the right lobe of the liver, and it was completely removed using laparoscopy. The pathomorphological study revealed a benign lesion that was identified as a congenital nonparasitic liver cyst, the epithelium of which had a columnar (cylindrical) structure (Fig. 5). The follow-up of the patient for 1 year showed no signs of relapse.
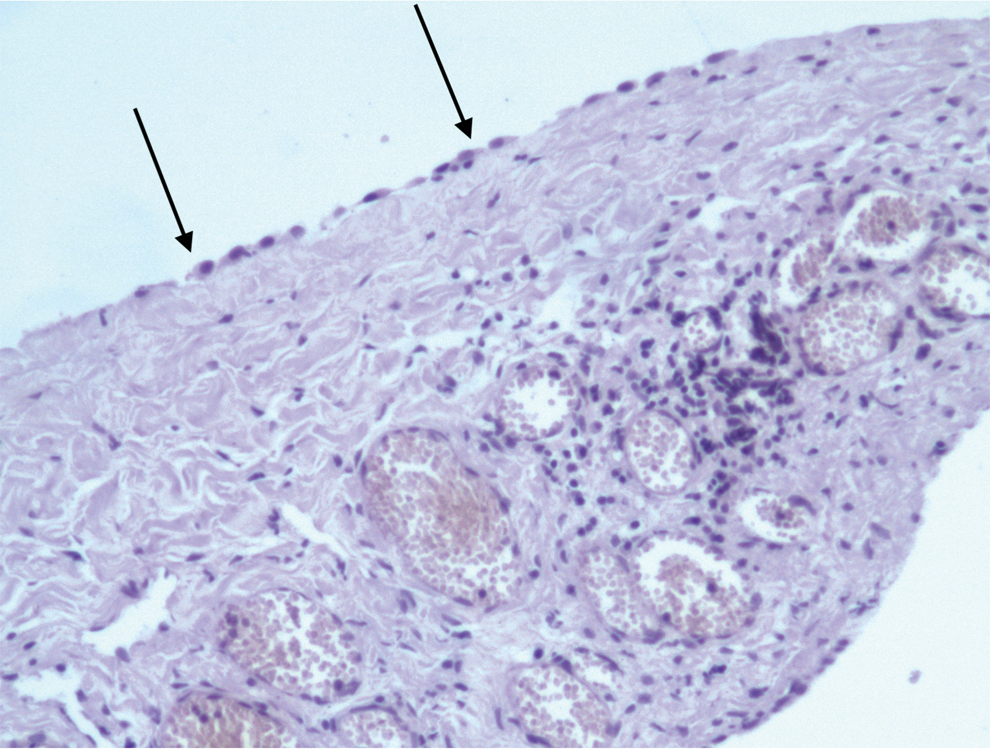
Morphological picture of the structure of the nonparasitic congenital cyst of the liver: microphoto—arrows indicate columnar epithelium of the cyst wall.
Case no. 2
A 10-day-old female was admitted to our center with a diagnosis of nonparasitic liver cyst. This was noted during antenatal ultrasound screening performed on the 32nd week of pregnancy and was confirmed in the maternity hospital. CT demonstrated a cyst connected with the liver tissue, measuring 4–5 cm. At laparoscopy, the cyst was in segment IV of the left lobe of the liver. The cyst was removed completely using laparoscopy. Histological examination revealed a benign single nonparasitic liver cyst lined with squamous epithelium. No evidence of recurrence was found during a 1-year follow-up.
Case no. 3
A 3-week-old female had a prenatal diagnosis of nonparasitic cyst of the liver. She was forwarded to our center after discharge from the maternity hospital. A CT determined a solitary liver cyst in the projection of segment V of the right lobe of the liver measuring 5.5 cm. A complete laparoscopic removal of the cyst was performed. Morphological study of pathological lesion determined a congenital nonparasitic liver cyst with capsule fibrosis. No sign of relapse was revealed during a 6-month follow-up of the patient.
Discussion
Epidemiology of the disease
Congenital nonparasitic liver cyst is a very rare disease. The review presented by Howard et al. reported 400 cases of the disease that were recorded in children among whom only 12 patients were aged younger than 2 years. 8
Congenital liver cyst occurs in the range of 0.1% to 2.5% among all cystic formations of the abdominal cavity,1,9 although the widespread introduction of ultrasound has shown that asymptomatic cysts are more common than originally expected. 10 It is difficult to estimate the exact frequency of this disease in the pediatric population since the symptoms of the disease appear and are usually detected in adult life. This statement is supported by data that only 10%–40% of congenital liver cysts are symptomatic. 11 A retrospective study based on the case records of children's hospital of Boston reported 30 cases of congenital nonparasitic hepatic cysts. In that series, symptoms occurred only in 40% of children while 60% were incidental findings on autopsies. 1 When detected in adulthood, hepatic cysts are mainly found at the age of 20–50 years.2,12 The ratio between women and men is 5:1.1,2
Classification and differential diagnosis
Hepatic cysts can be classified into two categories—congenital and acquired.13,14 They can be solitary or multiple (polycystic liver disease), simple, or complex. 14 Unlike polycystic liver disease, simple liver cysts do not have a genetic basis and do not show a connection with cystic lesions of other organs. 1 Acquired liver cysts may be parasitic (infectious) or nonparasitic (post-traumatic or tumor). 15 Parasitic cysts are usually represented by hydatid formations that occur as a result of infection of the body with the parasite Echinococcus granulosus. Most of the acquired nonparasitic liver cysts are post-traumatic pseudocysts. 15 Cystic liver tumors are rare. They include primary biliary cystadenoma, cystadenocarcinoma, and metastatic tumors of the pancreas or ovaries. 9
Asymptomatic hepatic cysts of small size (up to 1–2 cm) are considered benign; however, their growth should be observed to prevent the possibility of malignant degeneration. 10 Simple cysts, lined with squamous cell epithelium, may be more prone to metaplasia and malignant transformation, 16 and formation of adenocarcinoma or sarcoma on their site. 17 Septa, papillary structures, and multilocular formations increase the risk of malignancy. 18
Symptomatic liver cysts in infants and children can be quite large by contrast to a small abdominal cavity, so they can be difficult to distinguish from cystic lesions of other organs. Knowledge of differential diagnosis is important to choose the proper treatment strategy. Differential diagnosis of cystic lesions of the abdomen in young children includes cysts of the common bile duct, cystic form of intestinal duplication, macrocystic lymphangioma, cysts of the kidney, ovarian cysts, and mesenteric cysts. 19 The differential diagnosis of the older children also includes duplication of the gallbladder, cyst of the pancreas, mesenchymal hamartoma, hydronephrosis, Caroli disease, and metastases.1,20
Etiology
Congenital cysts are congenital anomalies originating from aberrant, often isolated bile ducts. They are usually lined with columnar epithelium of the bile ducts, although the squamous or cuboid type of epithelium can be determined. 15 Despite their origin, only 25% of cysts are connected with bile ducts. 15
The most common anatomical location is segment V of the right lobe of the liver. 20 The right lobe of the liver is affected twice as often as the left lobe. 1 Cysts can be both solitary and multiple affecting the entire liver (polycystic disease). They usually contain a clear liquid with a moderate amount of protein, cholesterol, blood cells, mucin, and epithelial cells. 20 The cause of cyst growth remains unclear; however, it may be assumed that it is associated with the accumulation of fluid as a result of secretion by bile epithelial cells or inflammation. 1 Thus, complete removal or destruction of the epithelium is the basis for the treatment of this disease.
Diagnosis
Most nonparasitic liver cysts are asymptomatic and are found in adult life. Only 10%–15% of hepatic cysts show signs of disease. 11 Hepatic cysts in infants are traditionally diagnosed when they become large enough to become visible through the thin abdominal wall. Widespread prenatal and postnatal ultrasound examination led to a rise in accidental discovery of accidental hepatic cysts in children of early age.
Symptoms of simple hepatic cysts are mainly associated with continuous secretion of epithelial cell fluid and the growth of lesion. Abdominal discomfort and upper abdominal pain are usually the first symptoms in adults. 20 In children, congenital liver cysts are most often detected during prenatal ultrasound screening. Later, CT or magnetic resonance imaging of the abdominal cavity is mandated to determine the precise location of the cyst. It determines the type of cyst and its location in relation to liver tissue. Symptoms associated with liver cyst in infants are due to its effect on adjacent internal organs and include abdominal pain, nausea, vomiting, signs of gastroesophageal reflux, shortness of breath, and respiratory distress.21,22 Most cysts are not connected with the bile ducts and blood vessels of the liver, but they can cause their obstruction or compression that result in obstructive jaundice, 15 cholangitis, 9 or portal hypertension. 11 Liver function is usually within normal limits with the exception of patients with obstructive jaundice. 10 Cases of acute complications of the cyst, including infection, ruptures, bile peritonitis, torsion, and intracystic hemorrhage, are described.1,11,18
Treatment
Surgery is indicated for both symptomatic (perforation, secondary infection, internal bleeding, torsion, malignancy) and asymptomatic forms. Small cysts (<1 cm) do not necessarily require treatment since the probability of their complications is believed to be lower than the risk associated with the operation. 23 These patients should be constantly monitored clinically and with sequential imaging studies to rule out cyst enlargement and malignant transformation.
Nonsurgical and surgical treatment options are available. Nonsurgical treatments include hepatic puncture with or without sclerotherapy. Surgical options include enucleation (cystectomy), fenestration, internal drainage, liver resection, and in exceptional cases, liver transplantation.
Since the treatment of hepatic cysts requires removal of the epithelial lining, a simple percutaneous puncture of the mass is ineffective and is accompanied by a 100% recurrence.11,12,19,23 Hepatic cyst puncture can only be used in certain conditions as a temporary measure to relieve severe or life-threatening symptoms, such as respiratory distress in a newborn.
Sclerotherapy is a minimally invasive procedure and is associated with fewer complications than surgery. However, it is accompanied by a higher frequency of relapses.19,23 The study of treatment of hepatic cysts in adult patients showed 100% recurrence of the disease after sclerotherapy. 24 There are several reports of the use of sclerotherapy in the treatment of hepatic cysts in children. 25 Ethanol injection was used in one newborn with a rapidly growing liver cyst without any evidence of recurrence during a 7-year follow-up. 26 Caution should be always used as sclerosant drugs (e.g., ethanol) can cause alcohol intoxication and sclerosing cholangitis. 14 The risk of these conditions in children is much higher than that in adults; for this reason, sclerotherapy is not widespread for the treatment of hepatic cysts in the pediatric population.
The basic principles of surgical treatment of congenital liver cyst include complete removal or destruction of its epithelium. The internal drainage of the cyst using cystojejunostomy on the Roux-en loop is performed in cases where the cyst is connected with the biliary ducts.
Until recently, fenestration was one of the most common methods of treatment of liver cysts. Lin et al. described the technique of wide opening of hepatic cysts in polycystic liver disease in 2 children and 3 adult patients. 26 Since then, this method has been successfully used by many surgeons to treat simple hepatic cysts. 10 Excision of the cyst wall that is outside the liver tissue leads to the formation of a large opening or window that makes possible to have free drainage of fluid into the abdominal cavity. Although the cyst wall continues to secrete fluid, the peritoneum reabsorbs this fluid. The recurrence rate after fenestration varies from 0% to 38%. 11 Omentoplasty reduces the recurrence rate to 14%. 11
Enucleation involves the complete removal of the epithelial lining of the cyst, often with a small fragment of liver tissue that results in a complete cure of patients. Complete removal of the cyst is considered as a method of choice for the treatment of congenital hepatic cyst. 19 Even a small amount of residual epithelium with incomplete resection can lead to relapse. Although enucleation leads to a lower rate of disease recurrence (4%), it is associated with a higher risk since the operation requires dissection of the liver parenchyma and may be accompanied by bleeding and leakage of bile. 27
Laparoscopic liver cyst resection in an adult patient was first performed in 1991. 28 Since then, the number of reports on the use of laparoscopy for the treatment of hepatic cysts has increased. However, treatment reports contain a small number of patients due to rare occurrence of the disease.10,16,22 The data available in the literature suggest that the recurrence rate after laparoscopic cystectomy is comparable to the number of recurrence of the disease after laparotomy. 11 In addition, laparoscopy proved to reduce pain and lead to rapid recovery of patients after the surgery. 19 Recurrence of the disease both after laparoscopy and with the open approach occurred when a part of the cyst epithelium was left on the surface of the liver, as well as due to the impossibility of complete resection of the cyst wall in case of intrahepatic location. 29
Laparoscopy is most often used for cystic lesions located in accessible areas, namely in the anterior and lateral segments of the liver. 14 Relative contraindications to the laparoscopic approach are hepatic cysts located deep within the liver parenchyma and connected with vascular structures as they increase the risk of massive bleeding or damage to the bile ducts.10,14
There are very few reports of the use of laparoscopy for the treatment of nonparasitic liver cysts in children. Several studies report the use of minimal invasive surgery in newborns.7,12 However, the experience of performing such operations in infants is limited. Nordin et al. 7 demonstrated 5 cases of laparoscopic treatment of nonparasitic cysts of the liver in infants, 2 of them consisting of the complete removal of the cyst and 3 being made with the principle of fenestration. Linden et al. reported the use of laparoscopy in 4 children, 2 of them were newborns. 4
Liver resection is mainly used for giant cysts, complex recurrent cysts, polycystic tumors, diffuse cystic liver damage, and cyst malignancy.14,15 Liver transplantation is performed very rarely and is intended for giant cysts or polycystic diseases in which resection will affect liver function.
We present a series of 3 neonates undergoing a laparoscopic surgery for simple congenital nonparasitic liver cysts. All 3 have a 6- to 12-month period of follow-up. The first patient was symptomatic, prompting us to perform the surgery in the neonatal period. Our series is small, but considering the rarity of the anomaly, it presents the largest single-center series of laparoscopic surgery for liver cysts in neonates. Therefore, although small, we may conclude that this approach is safe and feasible even in the neonatal period, in specialized centers. Imaging studies should include CT or magnetic resonance imaging to determine the location and type of the cyst before the surgery. Long-term follow-up is required to rule out recurrence.
Conclusions
Congenital nonparasitic liver cysts are rare in neonates and infants. They are considered a unique cause of abdominal tumors in the pediatric population. Although most hepatic cysts in children are asymptomatic, some infants may experience symptoms early in life and that often requires urgent surgery. Asymptomatic cysts also require surgical treatment because of the potential malignant transformation of these anomalies. Percutaneous puncture should be reserved only as a temporizing measure, and the risk of sclerotherapy is much higher than surgery. In specialized centers, the surgery may be performed safely even at the neonatal period.
Footnotes
Disclosure Statement
No competing financial interests exist.