
Abstract
Abstract
Background:
Our previous study demonstrated that lower level of education was associated with increased rates of postoperative hospital visits following bariatric surgery, potentially secondary to decreased understanding of postoperative expectations. Our follow-up study seeks to evaluate whether patients with lower level of education and health literacy have decreased weight loss success and resolution of comorbidities after bariatric surgery.
Methods:
Bariatric surgery patients presenting between October 2015 and December 2016 were administered a preoperative questionnaire, which reported education level and contained the Rapid Estimate of Adult Literacy in Medicine–Short Form (REALM-SF) health literacy test. The percentage of excess weight loss (EWL) and improvement of hypertension and diabetes mellitus at 6 months were compared across education level (≤12th grade versus >12th grade) and health literacy score (≤8th grade versus high school level) using Fisher's exact and Wilcoxon tests.
Results:
Seventy-eight patients were followed until their 6-month postoperative appointment (median 7 months, range 4–12 months); 6 scored ≤8th grade for health literacy on the REALM-SF (8%); and 21 had a ≤12th grade level education (27%). Patients with ≤8th grade on REALM-SF health literacy test lost 35% EWL versus 44% EWL by those with high school level health literacy score (P = .03). There was no significant difference in EWL compared across education level (44% versus 43%, P = .63). There were no significant differences in comorbidity improvement.
Conclusions:
The few patients in our cohort with a low health literacy level had a significantly lower EWL following bariatric surgery, and no differences were seen across education level. Increased vigilance in patients with low health literacy may be warranted to ensure excellent outcomes.
Introduction
Obesity affects 35% of the adult US population, while obesity related health care costs $200 billion and directly accounts for 21% of annual health care spending in the United States.1,2 Bariatric surgery has been widely accepted as the most effective treatment of obesity. Bariatric surgery is cost-effective with a 3-year break-even point due to decreased medical expenses following bariatric surgery attributed to resolution of obesity related comorbidities. 3
While the effectiveness of bariatric surgery is widely accepted, only a small percentage of the eligible obese adult US population will be treated with bariatric surgery annually. There are ∼78 million obese adults in the United States, but only 228,000 bariatric surgeries were performed in 2017.4,5 Certain socioeconomic factors associated with obesity may make the obese population more prone to disparities in access to bariatric surgery. Obesity is associated with lower socioeconomic status, while those actually undergoing bariatric surgery are more likely to have higher incomes. Martin et al. found that patients who are eligible for bariatric surgery in the United States (body mass index [BMI] >40 or 35–40 kg/m2 with obesity related comorbidities) were more likely to be nonwhite, underinsured, have lower family income, and have lower education levels than nonbariatric surgery eligible patients. However, patients who actually receive bariatric surgery were more likely to be white, have private insurance, and have above median incomes. 6
The disparity in access to bariatric surgery among those with lower socioeconomic status calls for exploration of these topics to maximize effective delivery of high-quality care to at-risk U.S. populations. The effect of health literacy and education level on outcomes in bariatric surgery has not been well documented in the literature as these patient characteristics are not well represented in national databases popular for outcome research. We previously showed that patients with a high school education or less were thrice more likely to have postoperative hospital visits at our center compared with the cohort obtaining higher levels of education. 7 We sought to follow this same cohort of patients to determine whether lower level of education and health literacy was associated with poorer weight loss success or improvement in obesity-related comorbidities after bariatric surgery.
Materials and Methods
Patient recruitment
All patients undergoing bariatric surgery at our center from October 1, 2015 to December 27, 2016 were offered voluntary participation in this study at their final preoperative clinic visit and followed prospectively. Five patients who were initially enrolled did not go on to have bariatric surgery and were ineligible for the study. Our initial analysis of this cohort investigated readmission rate at 30 days and enrollment ceased after 14 months as we found statistical significance in readmission between groups by education level on review at this point. 7 This cohort was then followed postoperatively with review of postoperative weight and diabetes/hypertension medications at their 6-month follow-up clinic visit. When a clinic visit at 6 months was not available, data from the nearest available visit were used. Patients with no postoperative visits between 4 and 12 months postoperatively were excluded. Institutional Review Board (IRB) approval was obtained from the University of North Carolina.
Education and health literacy testing
During the final preoperative clinic visit, enrolled patients completed a questionnaire. Patient education level was interpreted and dichotomized as ≤12 years of education (those without a high school degree or those with no post-high school education) and >12 years of education (those with post-high school education). GED was considered the equivalent of a high school degree.
Enrolled patients were also administered the Rapid Estimate of Adult Literacy in Medicine–Short Form (REALM-SF) assessment during the same visit to measure health literacy. Briefly, the REALM-SF is a 3-minute proctor-administered assessment. The patient is asked to pronounce seven health-related words, and the number appropriately pronounced is scored. The maximum score of 7 suggests high school level health literacy and that the patient would be able to read and understand most instruction materials. A score <7 implies less than high school level of health literacy and suggests that the patient would benefit from low-literacy materials. This test has been validated with three other standardized reading tests, including the Peabody Individual Achievement Test-Revised (PIAT-R), the Wide Range Achievement Test-Revised (WRAT-R), and the Slosson Oral Reading Test-Revised (SORT-R). 8 For this study, the REALM-SF was chosen for its ease of use, free access, and validation compared with more time consuming literacy tests. Patient literacy scores were also dichotomized into high school level (a score of 7) and less than a high school level (a score ≤6).
Data collection
Data were collected from review of the electronic medical record. The primary outcomes of interest were the percentage of excess weight loss (EWL), number of antihypertensives, number of oral diabetes medications, and whether insulin was still utilized 6 months after bariatric surgery. Improvement of comorbid conditions was classified as either a reduction in the number of overall medications or switching from insulin to oral diabetes medications. In addition, patient age, sex, BMI, excess body weight before surgery, procedure performed (laparoscopic sleeve gastrectomy or laparoscopic Roux-en-Y gastric bypass [RYGB]), and preoperative use of antihypertensives, diabetes medications, or insulin were abstracted.
Statistical analyses
Patient demographics and preoperative medication usage were described using univariate analyses. Potential differences in patient demographics and medications were compared across health literacy score and education level using Fisher's exact and Wilcoxon tests, where appropriate. A P value <.05 was considered significant. Fisher's exact and Wilcoxon tests were also used to assess differences in 6-month EWL and hypertension and diabetes improvement (among patients taking antihypertensives, diabetes medications, or insulin preoperatively).
All analyses were performed using SAS® 9.4 (SAS, Inc., Cary, NC).
Results
Of the 104 patients who agreed to participate (out of 110 eligible), 78 were included in the current analysis. Of the 22 excluded, 4 did not go on to have surgery, 11 were lost to follow-up at 6 months, 10 had their follow-up visit >12 months after surgery, and 1 patient was pregnant at her 6-month follow-up visit. See Figure 1 for summary of patients excluded. Median follow-up time was 7 months (interquartile range 6–8 months, range 4–12 months). Twenty-one patients (27%) had below or equivalent to a high school education, and only six patients (8%) had less than high school level health literacy. Of 21 patients, 4 (19%) with less than high school level education had low health literacy compared with 2/55 (4%) patients with at least high school level education (P = .04). No difference in follow-up time was seen across health literacy (P = .99) or education level (P = .63).
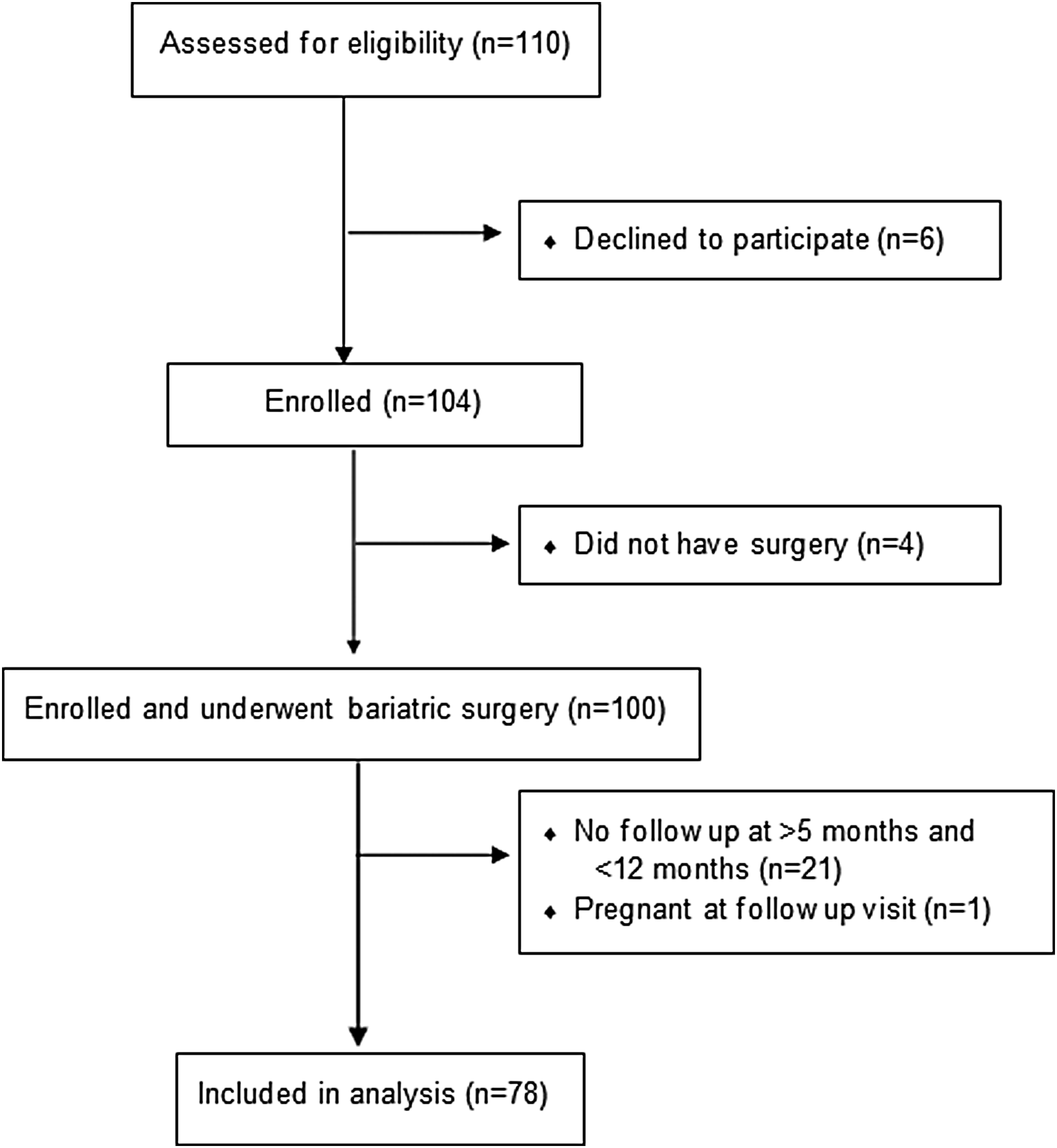
Summary of patients excluded.
Patients with lower health literacy were more likely to be male (50% versus 14%, P = .05), and patients with less than or equivalent to a high school education had significantly higher preoperative median excess weight (median weight 78 kg versus 66 kg, P = .04) (Table 1). No other differences in patient demographics or preoperative characteristics were seen across literacy or education level.
Patient Demographics and Preoperative Characteristics, n = 78
≤12 year includes “some high school,” “GED,” and “12th grade”; >12 years includes “some college,” “Bachelor's degree,” and “graduate degree.”
One laparoscopic sleeve was converted to open surgery.
GED, high school equivalency certificate; IQR, interquartile range; RYGB, Roux-en-Y gastric bypass.
Patients with less than high school level literacy level lost less weight than those with at least high school level literacy (35% versus 44% EWL, respectively, P = .03) (Table 2 and Fig. 2). There was no difference in weight loss between the low and high education cohorts (44% versus 43% EWL, P = .63). There was no significant difference in improvement in hypertension and diabetes mellitus between groups. All nine patients on insulin preoperatively saw improvement after surgery; at their follow-up visit, eight were no longer using insulin and one was using fewer units.

Distribution of estimated weight loss, %, stratified by health literacy and education level. Dots represent values outside the 5th and 95th percentiles.
Six-Month Postoperative Outcomes, Stratified by Health Literacy and Education Level
Only among patients on antihypertensives or diabetes medications or insulin preoperatively.
Bold font denotes statistical significance.
IQR, interquartile range.
Discussion
Several studies have previously sought to describe preoperative demographic factors that are correlated with weight-loss success or failure following bariatric surgery. Sillén and Andersson found earlier onset age of obesity, high preoperative BMI, psychiatric disorders, diabetes, and hypertension to be predictors of unsuccessful weight loss following RYGB. 9 Lutfi et al. found that single patients had greater weight loss than married patients following RYGB, while smoking, parent status, and employment status had no significant effect on weight loss. 10 One study that sought to identify psychological factors associated with poor weight loss outcomes found that patients who were more impulsive showed lower frustration tolerance or were more anhedonic, pessimistic, and introverted evidenced higher BMIs at the 5-year outcome than patients who did not evidence these symptoms/behaviors. 11
Several prior studies have examined the effect of socioeconomic factors on bariatric surgery outcomes. Medicaid patients have been shown to have less excess weight loss following RYGB compared to non-Medicaid patients. 12 Patients living in zip codes with lower median incomes were found to have a decreased excess body mass index loss after RYGB in a Veteran's Affairs population. 13 However, the effect of level of education and health literacy on postoperative weight loss has not been well described in the literature. This may be because patient education and health literacy levels are not easily available in outcome databases or retrospective chart review.
We found that patients with less than a high school level of health literacy in our cohort had statistically less weight loss than those with higher level of health literacy while there was no difference in EWL by education level. EWL in our cohort was similar to Fischer et al. who found a 44% EWL in 12 reports of 6-month follow-up of sleeve gastrectomy with over 100 patients. 14 We previously found that low education patients in this cohort were more likely to have postoperative emergency department visits and readmissions, 7 which is similar to prior studies that have found factors associated with low socioeconomic status such as Medicaid status to be associated with increased readmission rate.15–18 We hypothesized that low education level may lead to increased readmissions due to poorer understanding of postoperative expectations. Similarly, it may be that patients with low health literacy have decreased weight loss success due to lack of understanding of dietary changes necessary for successful weight loss outcomes. However, it is unclear whether low health literacy level itself is entirely responsible for decreased excess weight loss or if low health literacy is just a surrogate for other low socioeconomic status or psychosocial factors that could lead to decreased weight loss such as lack of access to healthy foods, exercise, and social support.
Strengths of this study include its prospective model and clearly defined objectives. Few studies in the bariatric surgery literature have obtained patient education and health literacy level. Limitations include the single-center study population which may limit its external validity, as well as the relatively small enrollment compared with larger database studies. Our center is unable to offer bariatric surgery to uninsured and Medicaid patients, which may decrease the proportion of low education and low literacy patients compared to the U.S. population. Another potential weakness of our study is the relatively short follow-up of 6 months, which was due to a significant number of our patients being lost to follow-up at the 1 year visit. Early weight loss has been shown to be predictive of long-term weight loss outcomes 19 so these trends are likely to continue if followed more long term. Finally, because there were relatively few patients that scored below perfect (<7) on the health literacy test or had less than a high school education, we had to dichotomize our exposures to meaningfully assess them.
As bariatric surgery has been proven to be the most effective treatment of obesity, expanding bariatric surgery availability to people of lower socioeconomic status should be a priority. We hypothesized that lower levels of education may predispose to worse outcomes after bariatric surgery, but found that those with lower level of education had no difference in EWL or improvement of hypertension or diabetes mellitus. Low literacy level was found in a small proportion of our patients and was correlated with a statistically significant decrease in EWL but no change in comorbidity improvement. Based on these findings, patients with lower levels of education seem to do reasonably well following bariatric surgery, while those few patients with low literacy score may deserve increased vigilance in preoperative education and postoperative monitoring to ensure excellent outcomes. More frequent follow-up with reinforcement of dietary expectations and weight loss goals could potentially improve outcomes in this group at high risk for weight loss failure.
The effects of education and health literacy on outcomes after bariatric surgery are not well represented in the literature, and future research on this topic is necessary. Future studies with greater enrollment could perform multivariate analysis to determine if other factors associated with low socioeconomic status are contributing to decreased weight loss success seen in low health literacy patients. Larger enrollment would also allow subgroup analysis by procedure type to determine if decreased weight loss is seen in malabsorptive (RYGB), as well as primarily restrictive (sleeve gastrectomy), procedures. If dietary noncompliance is higher in low-literacy patients, it may be that these patients would benefit more from a malabsorptive procedure. Furthermore, longer term follow-up is necessary to determine the durability of weight loss success in these patient groups.
Footnotes
Disclosure Statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.