
Abstract
Abstract
Background:
Endoscopic technique is a valid and safe approach for the treatment of abdominal wall defects. To combine the advantages of complete endoscopic extraperitoneal surgery with those of sublay mesh repair we propose Totally Endoscopic Sublay Anterior Repair (TESAR) a safe and feasible approach for the treatment of ventral and incisional midline hernias.
Methods:
From May to November 2018, 12 patients were referred to our unit for clinical and radiological diagnosis of midline ventral or incisional hernia and selected for TESAR. Exclusion criteria were: complicated ventral or incisional hernia (i.e., incarcerated hernia), maximum defect width >7 cm, and contraindications to general anesthesia.
Results:
All procedures were completed with endoscopic approach, with no conversion to laparoscopy or open surgery. No intraoperative complications were registered. Total mean operative time was 148 ± 18.5 minutes. No postoperative major complications were registered. Only one subcutaneous seroma was registered (8.3%) and treated conservatively. The mean postoperative stay was 2.6 ± 0.6 days.
Conclusions:
TESAR is a safe and feasible technique for the extraperitoneal sublay repair of ventral hernias with a totally endoscopic approach. It provides accurate hernia repair with good outcomes in terms of resolution of symptoms and postoperative complications.
Introduction
Minimally invasive surgery for incisional and ventral hernia repair has gained popularity in the last 25 years, due to the lower incidence of surgical site complications and similar recurrence rates compared with open repair.1,2 There are several recognized advantages of minimally invasive approach, like shorter hospitalization, lower pain, decreased recovery time, faster return to work or activity, improved cosmesis, and minimal wounds. 3 LeBlanc and Booth first described in 1993 the laparoscopic ventral hernia repair (LVHR) technique, characterized by the placement of an intraperitoneal mesh bridging the defect and fixed to the abdominal wall with appropriate overlap. 4 Despite different improvements in this approach during the years, some issues have been raised about its safety and potential long-term complications due to intraperitoneal mesh placement. For these reasons modifications of the original technique have been subsequently described, to minimize its pitfalls. 3 In particular approaches, including defect closure and extraperitoneal mesh placement have been proposed.5,6 More recently other approaches have been described to overcome the limitations of LVHR, in particular robotic-assisted hernia repair and several endoscopic techniques.7–14 These techniques seem to provide good results in terms of short-term outcomes, preserving the benefits of minimally invasive surgery, but without the risks associated to intraperitoneal mesh placement. In particular, the endoscopic techniques, currently with low diffusion, appear like a valid perspective for the treatment of abdominal wall defects. To combine the advantages of complete endoscopic extraperitoneal surgery with those of sublay mesh repair, we propose Totally Endoscopic Sublay Anterior Repair (TESAR) a safe and feasible approach for the treatment of ventral and incisional midline hernias. At the beginning of our experience we tested this approach for the treatment of diastasis recti and small midline hernias and their good outcomes suggested us a more extensive indication. 15
Materials and Methods
From May to November 2018, 12 patients were referred to our Unit for clinical and radiological diagnosis of midline ventral or incisional hernia and selected for TESAR. All patients underwent a preoperative study of the abdominal wall with physical and radiological examinations by ultrasound imaging and/or computed tomography (CT) scan. Exclusion criteria were: complicated ventral or incisional hernia (i.e., incarcerated hernia), maximum defect width >7 cm, and contraindications to general anesthesia. Candidate patients for TESAR presented ventral or incisional hernias for previous laparotomic or laparoscopic operations, and they were 7 males and 5 females with a mean age of 37.8 ± 5.4 years. After routine preoperative and anesthesiological examinations 4 patients were classified as ASA 1 and 8 patients as ASA 2.
The procedures performed in this study were in accordance with the ethical standards of the Institutional and National Research Committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Formal informed consent was obtained from all patients.
Procedure
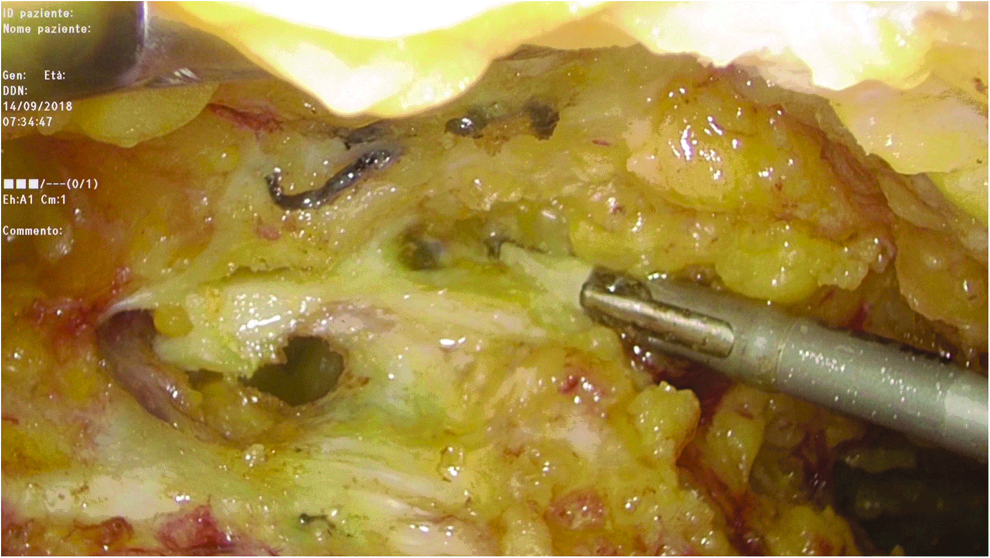
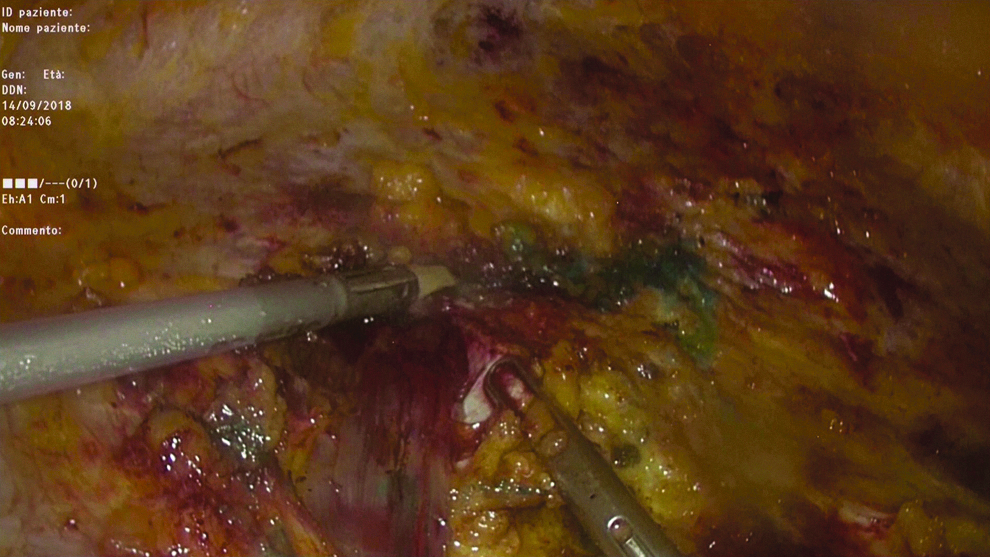
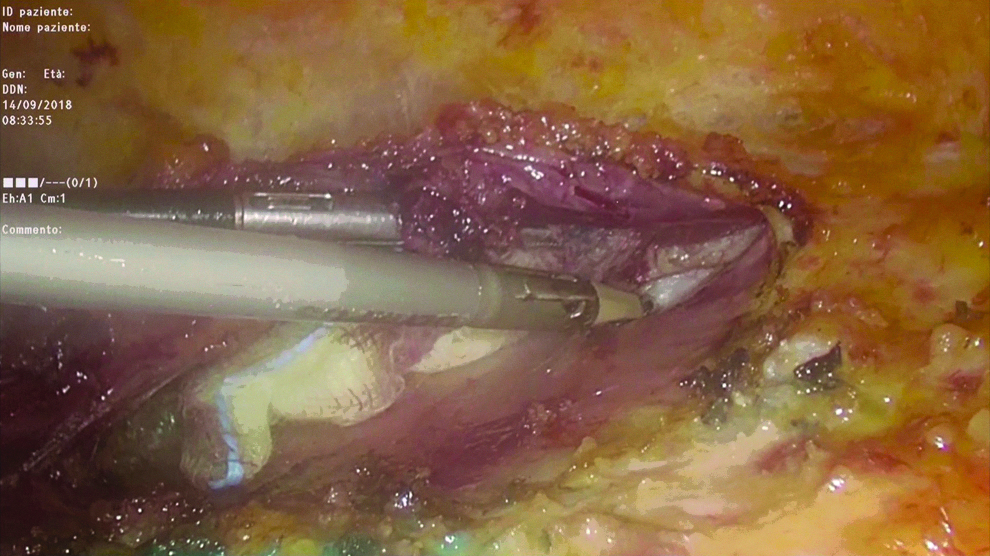
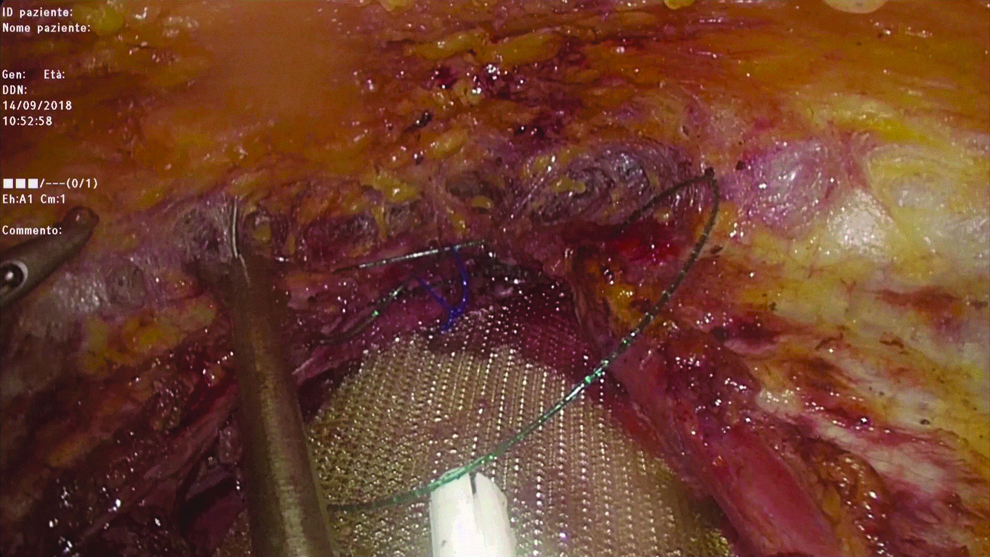
We perform the operation under general anesthesia with patient placed in supine position, split legs, and open arms. The monitor is placed over the right shoulder, the surgeon is placed between the legs and the assistant is placed on the left of the patient. Three mini incisions are carried out: 10 mm transverse suprapubic incision on the midline (4 cm above the pubic symphysis), used for the camera; another 10 mm transverse incision is performed 6–8 cm on the left (for the surgeon's right hand); and a 5 mm transverse incision is performed 6–8 cm on the right (for the surgeon's left hand). Through these incisions we proceed with blunt dissection of the subcutaneous plane, until the incisions are in communication, so the beginning of working camera is created (Fig. 1). This is a very delicate phase of the intervention because even if performed in part blindly (not under vision), it is necessary to obtain the correct work space. To help us in this phase and to allow better postoperative recovery we use subcutaneous infiltration with physiological solution, local anesthetic, and adrenaline. Only after creating this space we introduce the trocars and start with CO2 insufflation. CO2 is inflated at 8–10 mmHg and with Thunderbeat® we progress to create the working camera dissecting under endoscopic vision the subcutaneous preaponeurotic space (Fig. 2). This plane is created up to the subxiphoid region in the upper part, following the rib arches, until the midclavicular line bilaterally (lateral rims of both recti muscles), to promote skin retraction postoperatively. During this phase the ventral/incisional hernia is isolated (Fig. 3), the umbilicus is completely dissected, and the hernial sac is reduced into the abdominal cavity (Fig. 4). If the hernial sac is opened, CO2 pressure is reduced to 6–8 mmHg to introduce less CO2 into the abdominal cavity and the sac is repaired with reabsorbable suture under endoscopic vision. The anterior recti aponeurosis is marked and can be incised on its medial rims bilaterally from the subxiphoid region to the suprapubic space to expose the retromuscular space (Figs. 5–7). In case of small ventral or umbilical hernia we proceed to a less extensive dissection. In this phase, CO2 helps a safe dissection of the retromuscular plane in synergy with the action of Thunderbeat. If necessary we also repair the posterior fascia with a continuous barbed suture (we usually use Stratafix 1™). At this point, a polypropylene 30 × 15 cm mesh, tailored cut is inserted through the right trocar and positioned in the retromuscular space above the posterior aponeurosis (Fig. 8). The mesh is fixed with nonabsorbable polypropylene sutures to the four cardinal points. A suction drain, inserted through the left trocar incision, is positioned above the mesh in the retromuscular space through the left rectus muscle. Then we reduce the CO2 pressure to 6–8 mmHg to facilitate the closure of the anterior aponeurosis with direct reconstruction of linea alba by another continuous barbed suture (Stratafix 1) always under endoscopic vision (Fig. 9). With progressive deflation of CO2 the umbilicus is then fixed to the anterior aponeurosis with absorbable suture. A second drain is positioned through the right trocar in the subcutaneous space. At the end, a compressed binder is placed to prevent the risk of postoperative collection.

Blunt dissection in the subcutaneous space.
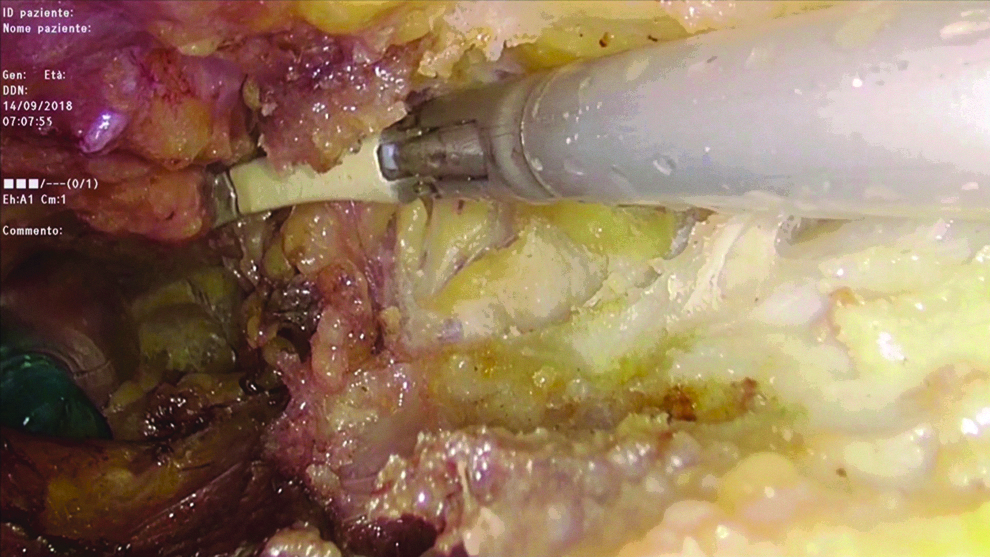
Dissection of the preaponeurotic plane.
Isolation of the sac.

Sac reduction.
Incision of the medial rims of recti aponeurosis.
Dissection of retromuscular space.

Complete bilateral retromuscular dissection.

Sublay mesh positioning.
Anterior aponeurosis reconstruction.
Results
Clinicopathological characteristics of the patients and main outcomes are summarized in Table 1. All procedures were completed with endoscopic approach, with no conversion to laparoscopy or open surgery. No intraoperative complications were registered. Total mean operative time was 148 ± 18.5 minutes. The retromuscular drain was removed on postoperative day (POD) 2 or 3 and the subcutaneous on POD 6–8. No postoperative major complications were registered. Only one subcutaneous seroma was registered (8.3%) and treated conservatively. The mean postoperative stay was 2.6 ± 0.6 days. At postdischarge clinical checkups drains were checked and removed when indicated. No wound complications nor recurrence were registered to date. Cosmetic and functional results were successful in all patients. We recommend abdominal compression binder for 2 months postoperatively.
Clinicopathological Characteristics of the Patients and Main Outcomes
PO, postoperative.
Discussion
LVHR with intraperitoneal onlay mesh placement (IPOM) is a consolidated procedure for the minimally invasive approach to primary and incisional abdominal wall hernias. 16 There are several technical issues about IPOM regarding the choice of mesh, the fixation method, the decision to close or not the hernia defect, and the position of the mesh. The general criteria of IPOM are universal, 17 they are mainly characterized by the peripheral trocar placement away from the defect, accurate adhesiolysis and hernia reduction, exact defect measurement preferably intracorporeal, mesh selection, mesh overlap, and mesh fixation to the peritoneum. 3 All these steps require a completely intraperitoneal access, the fundamental principle of IPOM. The most debated themes about this technique are with regard to intraperitoneal manipulation and mesh placement and fixation. In effect, the intraperitoneal site of mesh placement with possible complications, such as visceral adhesions, bowel obstruction, fistulas, mesh dislocation, together with intra-abdominal manipulation, and postoperative sequelae, such as chronic pain, were problems raised by some surgeons against the procedure. 16 In fact, there is also a described incidence of reoperation up to 25% for IPOM patients.18–20 Moreover, the classic IPOM approach does not include defect closure with consequence of postoperative problems, such as bulging of abdominal wall and seromas. Fascial closure has been recommended by some authors, but even if technically feasible, yet evidence of any superiority over standard procedure is lacking.21–23 For these reasons, modifications to the standard procedure have been proposed. One of the alternatives is transabdominal preperitoneal approach that has long been used for inguinal hernia repair, now applied also to ventral hernias. 24 The peritoneum is dissected and separated from the abdominal wall around the defect to create a large camera, where the mesh is inserted. After defect closure, the mesh is positioned in contact with the abdominal wall and the peritoneum is closed over the mesh, so it is excluded from the abdominal cavity. This technique seems to have comparable outcomes to standard IPOM, with lower complications.25,26 However, the primary issues of intraperitoneal access and manipulation are not excluded with this technique and the risk of visceral injury may vary from 4% to 21%.18,19,27,28 As a matter of fact in the last years more alternative approaches have been proposed to minimize the risks of minimally invasive ventral hernia repair. One of the most recent technological advance in this field is robotic-assisted hernia repair. First described in 2003 by Ballantyne et al. 29 with a standard IPOM approach, it has been subsequently improved for preperitoneal dissection and myofascial release to facilitate extraperitoneal mesh placement. Even if encouraging, there are still limited data about this technique, due to its recent implementation. Moreover, the high costs and the limited diffusion of robotic platforms among community hospitals make this technique difficult to spread. In more recent years there has been a huge proliferation of endoscopic techniques for abdominal wall repair, which aim to overcome the limitations of laparoscopy and robotics. First, introduced for the treatment of diastasis recti and midline hernias by Bellido Luque et al. in 2015, 8 their indications were then expanded to other conditions, such as primary and incisional hernias (Table 2). They have the advantage to be carried out with laparoscopic instruments available in common hospital theaters and the general principle among all of them is the extraperitoneal mesh placement. There are two main approaches, preaponeurotic or retromuscular dissection, some techniques are hybrid, with a first open or mini-open phase and a second endoscopic phase.
Main Studies About Endoscopic Techniques for Abdominal Wall Repair
ELAR, endoscopic-assisted linea alba reconstruction; EMILOS, endoscopic mini/less open sublay; eTEP, enhanced-view totally extraperitoneal; MILOS, mini/less open sublay; REPA, endoscopic preaponeurotic repair; TES, totally endoscopic sublay.
The technique described by the group of Guadalajara consists of totally endoscopic approach by suprapubic access with preaponeurotic dissection, preperitoneal mesh placement through the defect, and recti plication. They presented a prospective cohort study with 21 patients affected by midline hernias ≥2 cm (mean size 3.4 cm ±0.78) and associated diastasis recti. No major complications were described, but 23% incidence of seroma was registered, and all, except one case, were conservatively treated. 8
The mini/less open sublay (MILOS) concept was developed by W. Reinpold in 2015 and applied to ventral hernia surgery. 30 A large mesh is placed into the retromuscular plane through a small skin incision with the help of endoscopic instruments, which facilitates exposure, visualization, and retraction. There is a recent report of MILOS application where this technique shows lower complication rates, recurrence, and chronic pain compared with IPOM and open surgery. However, there was also a reported mean skin incision of 6.8 cm (range, 2–12 cm), and these data raise doubts about the mini-invasivity of the procedure. 12 The same group described also the endoscopic mini/less open sublay (EMILOS), to implement the MILOS concept. This is essentially a reversed total extraperitoneal procedure in which the first steps are identical to the MILOS, then immediately after opening of the rectus sheath, the operation continues with endoscopic dissection of the retromuscular space. The authors proposed this variation in case of primary or incisional ventral hernia associated to diastasis recti. No particular complications were described in the first series of 25 patients published. 9
The endoscopic assisted linea alba reconstruction (ELAR), primarily indicated for symptomatic umbilical, trocar, and/or epigastric hernias and concomitant rectus abdominis diastasis, consists of an hybrid approach with periumbilical incision and hernia repair and then endoscopic reconstruction of the linea alba by the anterior rectus sheaths and bridge mesh placement above recti muscles. In the first 140 patients, the authors described no recurrence, 2 cases of redo surgery due to bleeding, and 9 cases of impaired wound healing. 10
The enhanced-view totally extraperitoneal (eTEP), previously described for inguinal hernia repair, 31 has then been applied to upper and lower midline ventral and incisional hernias. This is a totally endoscopic technique in which the working camera is created directly in the retromuscular space, where the mesh is then placed. Trocar placement varies according to the defect position and in case of large defects (>10 cm) transversus abdominis release (TAR) is also associated. Defects in the posterior and anterior rectus sheaths are always closed. The authors described a low rate of intraoperative and postoperative complications (2.5% and 3.8%, respectively) and 1 case of recurrence after 332 days of mean follow-up.
The endoscopic preaponeurotic repair (Reparación Endoscópica Pre-Aponeurótica in Italian [REPA]) described in 2017 13 and recently updated with complete follow-up data 32 is characterized by suprapubic access and totally endoscopic preaponeurotic dissection up to 3 cm beyond the bilateral costal margin and laterally to the anterior axillary lines. Then recti sheaths are plicated with barbed suture from the xiphoid appendix to 5 cm subumbilical and onlay mesh is positioned and fixed to the anterior recti aponeurosis with trackers, straps, or absorbable suture. This technique is only indicated for diastasis recti associated to midline hernias. In the first 50 cases no intraoperative complications were described, seroma was registered in 12% cases, all conservatively treated, except one needing drainage.
The most recently described technique is totally endoscopic sublay (TES) repair indicated for primary or secondary midline ventral hernias ≤10 cm. After a first phase of minimal subcutaneous access and dissection the working camera is created in the retromuscular space, the hernia is reduced, posterior and anterior rectus sheaths are closed, and sublay mesh is positioned and fixed with chemical glue. The first 26 patients treated with this technique registered no particular intraoperative or postoperative complications nor recurrence with mean follow-up of 9.2 months. 14
Our approach, already tested for the treatment of diastasis recti and small midline hernias with encouraging results, 15 combines the advantages of totally endoscopic anterior access with those of sublay repair, which is, in our opinion, but also for many other surgeons, the optimal treatment for ventral hernias, especially in terms of recurrence and surgical site infections. 33 All minimally invasive techniques described above are valid and we think that the endoscopic approach is an effective and safe technique for the treatment of abdominal wall defects. However, MILOS and EMILOS do not offer a totally endoscopic approach, eTEP and TES, although totally endoscopic, require direct access and dissection into the retromuscular space and this can be very challenging in some patients, particularly in case of narrow retrorectus planes, with small working camera. On the other hand, REPA and ELAR are characterized by onlay mesh placement and not indicated for incisional hernias. In fact they are described for diastasis recti and small midline hernias only.
TESAR offers the same anterior suprapubic extraperitoneal approach for every type of hernia, and with no need of changing port placement, it creates a large working camera where the dissection allows to easily and safely identify every anatomic structure and to perform a perfect hernia isolation and reduction. All the planes can be correctly dissected, from the subcutaneous space to the posterior rectus sheath, the hernia sac can be reduced and dissected from the subcutaneous plane and, if opened, it can be sutured as in open surgery. Then complete reconstruction of posterior and anterior recti sheaths, after sublay mesh placement, is performed as in the open approach. The surgeon works in a safe and comfortable space, larger than eTEP or TES, all the phases are performed in extraperitoneal way and sutures are easy to carry out. In addition, the large subcutaneous dissection allows postoperative cutaneous retraction with also good cosmetic results without any problem of wound infection or ischemia. The incidence of subcutaneous seroma is still low and comparable to other techniques. Finally, TESAR is indicated for both ventral/incisional hernias and for diastasis recti as well.
Although the lack of long follow-up, in our experience we did not register any intraoperative complication, operative time, hospital stay, and postoperative complications were comparable to the other techniques. In particular, operative times are reducing as experience advances. We do not expect a higher incidence of seroma or bleeding compared with those described in the literature, considering also that we use advanced energy devices that are supposed to decrease serous secretion and bleeding.
We have limited our initial experience to simple cases with no incarcerated hernias and defects ≤7 cm, but we are planning to expand our indications, maybe with the implementation of additional features such as TAR or including also lateral hernias.
In conclusion, TESAR is a safe and feasible technique for the extraperitoneal sublay repair of ventral hernias with totally endoscopic approach. It provides accurate hernia repair with good outcomes in terms of resolution of symptoms and postoperative complications. Further investigation will provide longer follow-up data and expanded indications.
Footnotes
Disclosure Statement
No conflicts of interest or financial ties to disclose.