
Abstract
Abstract
Background:
Laparoscopy and more recently robotics are increasingly used for colorectal cancer surgery in the United States. We examined the current trends of minimally invasive surgical resections for colorectal cancer in Florida.
Methods:
The Florida Inpatient Discharge Dataset was used to examine the clinical data of patients who underwent elective surgery for colorectal cancer during 2013–2015. Multivariate analyses were performed to compare patient characteristics associated with the use of open and minimally invasive surgeries.
Results:
A total of 10,513 patients were analyzed; 5451 (52%) had open surgery, 4403 (42%) laparoscopy, and 659 (6%) robotic surgery. The rates of minimally invasive surgery (MIS) increased from 46.95% in 2013 to 48.72% in 2015. Among minimally invasive surgical procedures, the use of robotics increased from 9.82% in 2013 to 15.48% in 2015. Metastatic cancer (odds ratio [OR] 0.61, confidence interval [CI] 0.55–0.67), Elixhauser score of 3–5 (OR 0.85, CI 0.76–0.95) or more than 5 (OR 0.78, CI 0.63–0.97), Medicaid insurance (OR 0.73, CI 0.6–0.89), Black race (OR 0.88, CI 0.77–0.99), and rural residence (OR 0.83, CI 0.69–0.99) were associated with lower odds of MIS than open surgery.
Conclusions:
This study demonstrates that the overall rates of MIS for colorectal cancer in Florida increased from 2013 to 2015. Socially deprived and very sick patient populations with colorectal cancer are less likely to undergo MIS.
Introduction
Laparoscopy and more recently robotics have been increasingly used in colorectal cancer surgery.1,2 The benefits of the laparoscopy to colorectal cancer treatment have been previously demonstrated by landmark randomized clinical trials, including the COST trial,3,4 COLOR trial,5,6 COLOR II trial, 7 COREAN trial,8,9 and CLASICC study.10–12 These trials found an improvement in short-term surgical outcomes, and equivalent long-term oncologic and survival outcomes compared to open surgery. Other studies also indicate that minimally invasive platforms result in less blood loss, lower postoperative pain, early recovery of bowel function, decreased length of stay, lower readmission rates, and reduced postoperative mortality.13–18 The more recent use of robotics has also seen a reduction in conversion rates to open surgery compared with laparoscopic surgery.15,17,19
However, the use of laparoscopy and robotics in colorectal surgery is not without drawbacks. Two recent clinical trials (The ACOSOG and ALaCaRT trials) have challenged the noninferiority of the laparoscopic approach for rectal cancer, suggesting that the oncologic outcomes with laparoscopy may not be equivalent to open surgery.20,21 In addition, laparoscopic colectomies require a steep learning curve and advanced technical expertise compared to open surgery.1,22 Robotics can result in significantly higher total procedure-related charges,19,23 although there is evidence that the laparoscopic approach results in lower total hospital costs than open surgery.14,23
In 2012, the American Society of Colon and Rectal Surgeons (ASCRS) reported that laparoscopic colectomy for curable cancer results in equivalent cancer-related survival to open colectomy, and that minimally invasive surgery (MIS) for rectal cancer is appropriate in the hands of well-trained surgeons following accepted cancer surgery principles. 24 Although subsequent investigators have reported national variations in the use of laparoscopic and robotic surgeries for colorectal cancer patients,25–27 an evaluation of state-level data is likely to reveal pertinent differences not captured by national studies. A previous study which assessed state-level data in Nebraska found important differences in the receipt of laparoscopic colectomy between rural and urban colon cancer patients. 28
Florida is the 4th most populous state in the United States and the 19th ranked state for colorectal cancer screening in the nation, with an age-adjusted incidence rate of 119 cases per 100,000 population among adults aged 50 years or older.29,30 The primary objective of this study was to examine the current trends of MIS use among patients undergoing elective surgery for colorectal cancer in Florida. This study also sought to identify pertinent patient and geographic characteristics associated with the receipt of laparoscopy and robotics for colorectal cancer.
Materials and Methods
Data source
The 2013–2015 Florida Inpatient Discharge Dataset was utilized for this analysis. This dataset provides anonymized patient level data from all acute care hospitals within the state of Florida and includes information regarding diagnosis, treatment, patient demographics, hospital as well as physician characteristics. 31 Due to the publically available nature of the dataset, as well as the anonymous nature of the patient data, the Institutional Review Board categorized the research as exempt.
Population and variables
The population for this analysis included all patients in Florida who were diagnosed with colorectal cancer (ICD-9 codes 153.0, 153.1, 153.2, 153.3, 153.4, 153.5, 153.6, 153.7, 153.8, 153.9, 154.0, and 154.1), and who received the following colorectal procedures: cecectomy, right or left hemicolectomy, transverse colectomy, sigmoidectomy, total colectomy, anterior resection, and abdominoperineal resection. Patients excluded from the analysis include those who underwent multiple segmental colectomy (n = 42) and pull-through resection (n = 73) based upon small samples and lack of variance. In addition, those that were identified as emergent cases were excluded due to considerations of significant differences in clinical disease burden and surgical approach. The study period extended from January 2013 to September 2015 (33 months) due to the restraints imposed by the change in procedure codes from ICD-9 to ICD-10 within the dataset in the fourth quarter of 2015.
Dependent variable
The dependent variable for this analysis was the surgical approach classified as open or MIS (laparoscopic or robotic). ICD-9 Codes were utilized to define the colorectal surgical approach. If a robotic surgery indicator was present (ICD-9 Codes: 17.41 and 17.42), the surgery was classified as robotic. If no robotic code was present, but a laparoscopic code (ICD-9 Codes: 17.32, 17.33, 17.34, 17.35, 17.36, 45.81, 48.42, and 48.51) was present, then it was laparoscopic. If neither code was present, it was classified as an open surgery (ICD-9 Codes: 45.71, 45.72, 45.73, 45.74, 45.75, 45.76, 45.82, 48.43, 48.52, and 48.63). An exception to this was anterior resection of the rectum (ICD 9 code 48.63), which does not differentiate between open and laparoscopic approaches. To identify laparoscopic anterior resection of the rectum, we utilized two secondary laparoscopic codes (ICD 9 codes: 54.21 and 54.51) combined with primary code (ICD 9 code 48.63).
Independent variables
Patient characteristics, namely sex, age, race, ethnicity, and location, including region and rurality, as well as payer type, were included as covariates. Race was divided into three categories (white, African American or black, and other). The “other category” was utilized due to low frequencies in the non-white or black categories and include Asian, American Indian or Alaska Native, Native Hawaiian or other Pacific Islander, and unknown categories. Ethnicity includes Hispanic or Latino and non-Hispanic or Latino, while Payer includes the patient's identified insurer, including Medicare, Medicare Managed Care, Medicaid (Medicaid Patient and Medicaid Managed Care Patient), commercial, or other, which includes self-pay or nonpayment. Patient region was divided into seven regions as defined by the Florida Department of Transportation and indications of rurality as defined by the Florida Department of Health. 32 In addition, patient comorbidities were defined via the Elixhauser Score, which is divided into four categories indicating the presence of 0, 1–2, 3–5, or greater than 5 comorbidities. 33 Due to their importance, both metastatic cancer and obesity were included as separate variables and not included within the Elixhauser score. Finally, the year of diagnosis was included to provide better context concerning the changes in open versus minimally invasive surgeries occurring over time.
Analysis
Data were described as percentages or means and Pearson χ 2 and t-tests were used to compare categorical and continuous variables, respectively. In addition, three multivariable logistic regression models were utilized to compare differences in patient characteristics, location, comorbidities, or year of diagnosis and MIS versus open surgery, and robotic versus laparoscopic surgery. All tests of significance were 2-sided, and both the 95% confidence interval and the P-value were reported. The level of statistical significance was set at P-value <0.05. Analyses were performed using SAS version 9.4 (SAS Institute Inc).
Results
A total of 10,513 patients undergoing elective colorectal resections were analyzed. Of these, ∼52% had open surgery, 42% laparoscopic surgery, and 6% robotic surgery. The mean age of patients was 68.4 years (SD, 12.7) overall, 68.0 years (SD, 12.8) for open surgery, 68.8 years (SD, 12.5) for laparoscopic surgery, and 68.4 years (SD, 12.3) for robotic surgery. The largest patient categories were male (51.9%), white (83.8%), non-Hispanic (85.0%), Elixhauser Score of 1–2 (47.8%), Medicare insured (35.5%), and lived in urban areas (95.0%). In addition, 20.1% of the patients had metastatic cancer and 13.0% were obese (Table 1).
Patient Demographics and Clinical Characteristics By Surgical Approach
χ 2 test.
t-test.
Trends in MIS
The rates of MIS increased from 46.95% in 2013 to 48.72% in 2015 (Fig. 1). Among minimally invasive surgical procedures, the use of robotics increased from 9.82% in 2013 to 15.48% in 2015 (Fig. 2).
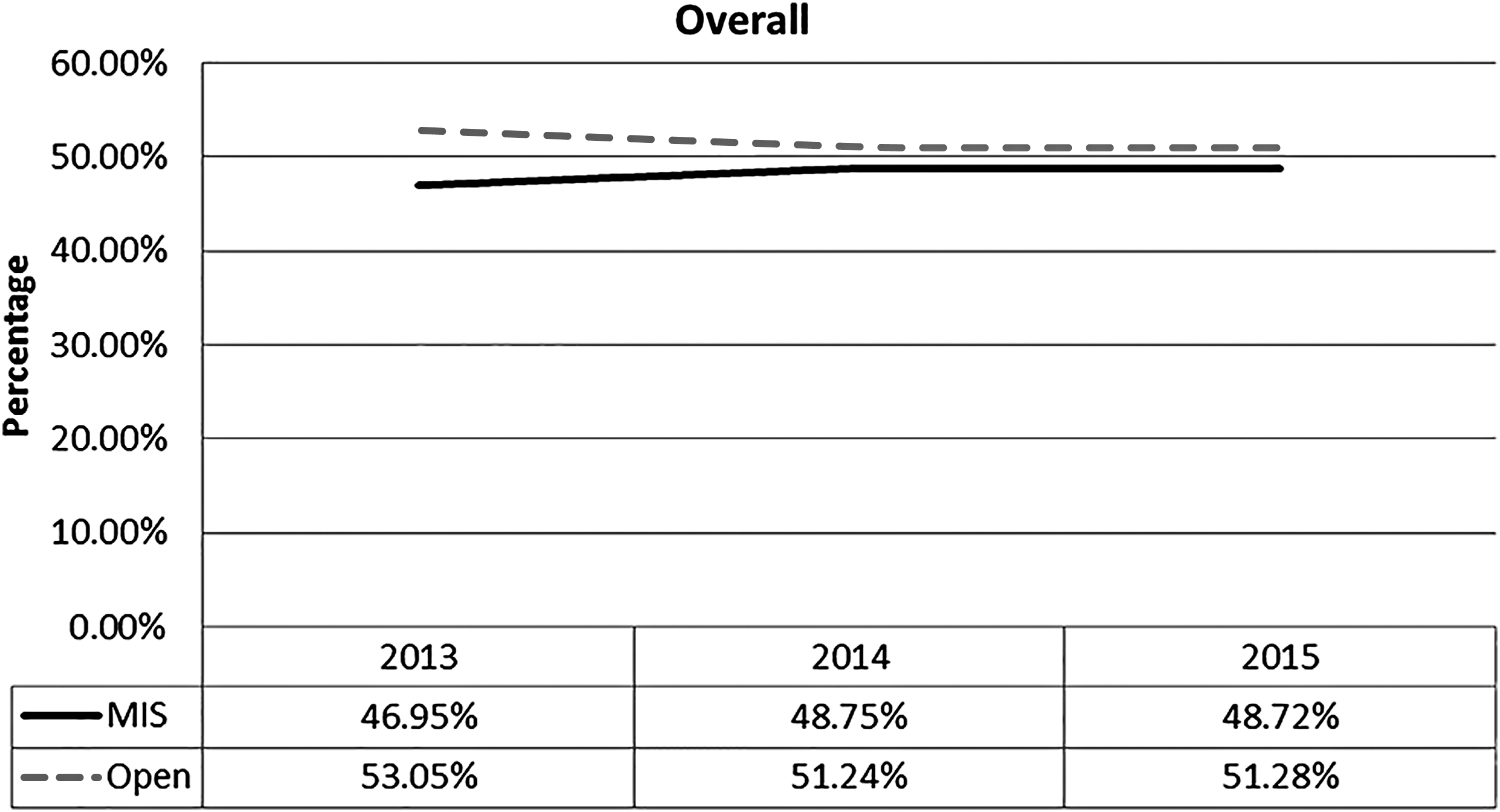
Overall Trends in Open and Minimally Invasive Surgical Procedures for Colorectal Cancer from 2013 to 2015.

Trends in Laparoscopy and Robotics for Colorectal Cancer Surgery from 2013 to 2015.
Table 2 shows univariate associations between patients characteristics and surgical approach. Metastatic cancer (odds ratio [OR] 0.61, confidence interval [CI] 0.55–0.67), Elixhauser score of 3–5 (OR 0.85, CI 0.76–0.95) or more than 5 (OR 0.78, CI 0.63–0.97), Medicaid insurance (OR 0.73, CI 0.6–0.89), Black race (OR 0.88, CI 0.77–0.99), and rural residence (OR 0.83, CI 0.69–0.99) were associated with lower odds of minimally invasive than open surgery. Females (OR 1.10, CI 1.02–1.19), older patients (OR 1.05, CI 1.02–1.08), Hispanic individuals (OR 1.46, CI 1.31–1.63), and residents of South Florida (OR 1.28, CI 1.09–1.49) were more likely to undergo minimally invasive than open surgery.
Univariate Associations Between Surgical Approach for Colorectal Cancer and Patient Characteristics
ORs, 95% CIs, and P-values result from logistic regression models.
CI, confidence interval; MIS, minimally invasive surgery (laparoscopy + robotics); N/A, not applicable; OR, odds ratio.
Among minimally invasive procedures, a more recent year of diagnosis (OR 1.66, CI 1.34–2.05 for 2015) and Hispanic ethnicity (OR 1.25, CI 1.01–1.53) were associated with greater odds of robotics than laparoscopy, while obesity (OR 0.76, CI 0.58–0.99) and rural locations (OR 0.5, CI 0.30–0.84) were associated with lower odds of robotics compared with laparoscopy.
Multivariate analysis
Minimally invasive versus open surgery
After adjustment for covariates, metastatic cancer (OR 0.61, CI 0.55–0.67), Elixhauser score of 3–5 (OR 0.81, CI 0.71–0.92) or more than 5 (OR 0.76, CI 0.60–0.95), and Medicaid insurance (OR 0.74, CI 0.60–0.91) were associated with lower odds of minimally invasive than open surgery (Table 3). Female (OR 1.11, CI 1.02–1.20) and Hispanic patients (OR 1.19, CI 1.03–1.38) had higher odds of MIS.
Multivariate Associations Between Surgical Approach for Colorectal Cancer and Patient Characteristics
ORs, 95% CIs, and P-values result from logistic regression models.
CI, confidence interval; MIS, minimally invasive surgery (laparoscopy + robotics); N/A, not applicable; OR, odds ratio.
Robotic versus laparoscopic surgery
Among patients who underwent MIS, female patients had lower odds of robotics than laparoscopic surgery (OR 0.83, CI 0.70–0.98). Medicare managed care was also associated with lower odds of robotics than laparoscopic surgery (OR 0.75, CI 0.59–0.95). A more recent year of diagnosis was associated with higher odds of robotics than laparoscopic surgery (OR 1.66, CI 1.34–2.07).
No associations were observed between race and surgical approach in the multivariate analysis.
Discussion
This large retrospective cohort study examined the trends of minimally invasive surgical procedures for colorectal cancer in Florida between 2013 and 2015. The primary finding in our study is that the use of MIS increased during the 3-year period. We also observed a growth of robotics among procedures performed via MIS in the study period. Pertinent patient characteristics that correlate poorly with the receipt of MIS for colorectal cancer include metastatic cancer, presence of comorbidities, Medicaid insurance, Black race, and rural residence.
The prevalence of laparoscopy (42%) in the present study is similar to previous large retrospective studies (40%–55%),2,25,34–36 but the rate of robotic surgery (6%) is higher than more recent large retrospective studies (1.5%–4.7%).19,25,34,37 Our study gives additional credence to recent studies that show an upward trend in the adoption of MIS for colorectal cancer. A review of the Nationwide Inpatient Sample for patients who underwent elective colectomy for colon cancer or diverticular disease showed an increase in laparoscopic colectomy from 51.3% in 2009 to 59.3% in 2012. 2 A more recent retrospective study using the Premier Hospital Database reported that the use of laparoscopy for colon cancer increased from 48.94% in 2009 to 52.03% in 2014. 36 Similarly, a national study of rectal cancer patients by Moghadamyeghaneh et al. reported a fourfold increase in the rate of robotic procedures from 2.1% to 8.1% during a 2009–2012 study. 19 Compared to older studies, the slight reduction in laparoscopy frequency in 2015 in the present study is likely due to an uptake in robotic surgery during the study period (Fig. 2). It may also be due to the impact of recent clinical trials such as the ACOSOG and ALaCaRT trials that demonstrated that laparoscopic resection of rectal cancers did not meet the criterion for noninferiority for pathological outcomes compared with open resection.20,21
Despite the upward trend of MIS, important differences persist by patient location, demographic, and clinical characteristics. Patients residing in rural areas were less likely to receive MIS. Furthermore, after adjustment for covariates, there was a trend toward a lower likelihood for robotic surgery in rural locations (OR 0.61, P = 0.07). Given the relatively recent emergence of robotics and associated costs, it is possible that these technologies are still in the early stages of adoption in rural locations. Another consideration is the extent of dissemination of robotic expertise in rural facilities, as a similar effect has been demonstrated for laparoscopic colectomies in rural hospitals in Nebraska. 28 In comparison, there was an increased likelihood of robotic surgery in South Florida, a region characterized by large urban cities, academic medical centers, high-volume centers, and availability of fellowship training programs; characteristics associated with increasing use of MIS.34,38–40
For gynecology, robotic surgery seems to be advantageous for obese patients, leading to fewer complications and shorter length of stay.41,42 This advantage is likely due to the potential of robotics to facilitate technically complex manipulations within the narrow pelvic space. In comparison, our study data show that obesity is associated with lower use of robotic surgery for colorectal cancer. A possible explanation for this could be the tendency of obesity to increase the risk for conversion of robot-assisted colectomies to open surgery due to difficult dissection, 43 although the reasons remain unclear. In comparison, when Schootman et al. evaluated the use of robot-assisted surgery (RAS) for colon cancer and nonmalignant polyps, they found that obese patients were equally likely to receive RAS as nonobese patients. 44
In a study of patients undergoing partial colectomies, Bardakcioglu et al. reported that Medicaid and self-pay were significant negative socioeconomic determinants of MIS. 39 Similarly, we found that patients with Medicaid insurance were less likely to receive MIS. This is likely due to the proportionally higher procedure charges and costs associated with minimally invasive technologies. Unexpectedly, Medicare insurance was associated with increased likelihood of receiving MIS. Although this finding is encouraging due to the high proportion of elderly Medicare-insured patients in Florida, our understanding of the association is incomplete. Thus, additional studies are underway to clarify this association.
Our study has important limitations. The use of state level data may in some cases limit the generalizability of the findings to other populations with significantly different demographics. However, Florida has an ethnically and socially diverse population. In addition, the administrative nature of the data and the retrospective perspective limit the ability to assess all aspects of patient care which constrains the ability to accurately account for all possible factors associated with the use of MIS. For example, there are a number of other covariates that can potentially impact surgical approach which have not been captured in this analysis. These include previous abdominal operations, tumor size and invasion, surgeon training and experience, access to the robot, and economic market forces. The relatively short duration of the study period (2013–2015) may also restrain the ability to observe significant changes in practice patterns. The switch in coding system from ICD 9 to ICD 10 within the Florida Inpatient Discharge Dataset restrained the potential to extend the study period beyond the third quarter of 2015 due to differences in granularity between the two coding systems. We envisage that as more data become available, changes in practice patterns can be better characterized.
Conclusions
This study demonstrates that the overall rates of MIS for colorectal cancer in Florida increased from 2013 to 2015. Equally important, a significant growth of robotics was seen in procedures performed via MIS in the study period. Although these results are encouraging, socially deprived and very sick patient populations with colorectal cancer are less likely to undergo MIS. Future research is recommended to investigate the role of hospital characteristics as well as the possible influence of surgeon training and experience on the adoption trends of MIS.
Footnotes
Acknowledgments
This work was supported by the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.
Authors' Contribution
All authors were responsible for the drafting of the article, analysis, and interpretation of data, and critical revision of the article for important intellectual content. The study has been approved by all authors in the present format.
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.