
Abstract
Abstract
Background:
Laparoscopic intracorporeal sutures and knots require advanced techniques in children. The JAiMY® needle holder (Endocontrol Company, Grenoble, France), a flexible jaw with both clockwise and anticlockwise revolving functions, enables the placement of sutures in very small working spaces. Using this tool, a novel new ligation method, which we named “twitching technique,” can be performed.
Methods:
To perform the “twitching technique,” first grasp the long tail of the thread with the JAiMY and the forceps on the needle side. Then, rotate the tip of the needle holder halfway in either direction and bring the forceps closer to the needle holder to make a ring using the thread. Grasp the thread at the crossing point with the forceps, and then catch the short tail through the ring with the needle holder.
Results (Case Presentation):
A 1-year-old boy presented with vomiting because of esophageal hiatal hernia. He was being treated for single ventricle and asplenia at our hospital. Laparoscopic esophageal hiatus plication was performed. Although the working space was extremely limited, the JAiMY and the “twitching technique” enabled steady suture placement and ligation.
Conclusions:
The “twitching technique” is an easy, steady, and safe method for performing ligation in difficult situations and may facilitate the performance of many laparoscopic surgeries in pediatric fields.
Introduction
Laparoscopic approaches are now widely accepted in many pediatric surgery fields. 1 However, laparoscopic surgery is associated with higher degrees of technical and ergonomic difficulty in comparison with open surgery due to the limited degrees of freedom (DOF) of the forceps.2,3 Up to 80% of laparoscopic surgeons suffer musculoskeletal pain of the shoulder-arm and neck due to the difficult positions in which they must operate. 4 In particular, advanced techniques are required for the placement of intracorporeal sutures and knots in pediatric patients because the working spaces in children are small. The JAiMY® needle holder (Endocontrol, Grenoble, France), a flexible jaw with both clockwise and anticlockwise revolving functions, enables the placement of sutures in very small working spaces (Fig. 1). 5 The instrument is the only robotized needle holder that can be used through a 5-mm laparoscopic port. This tool allows for the placement of a novel ligation method, which we named the “twitching technique.” We herein report the in vitro and in vivo (case presentation) suture techniques.
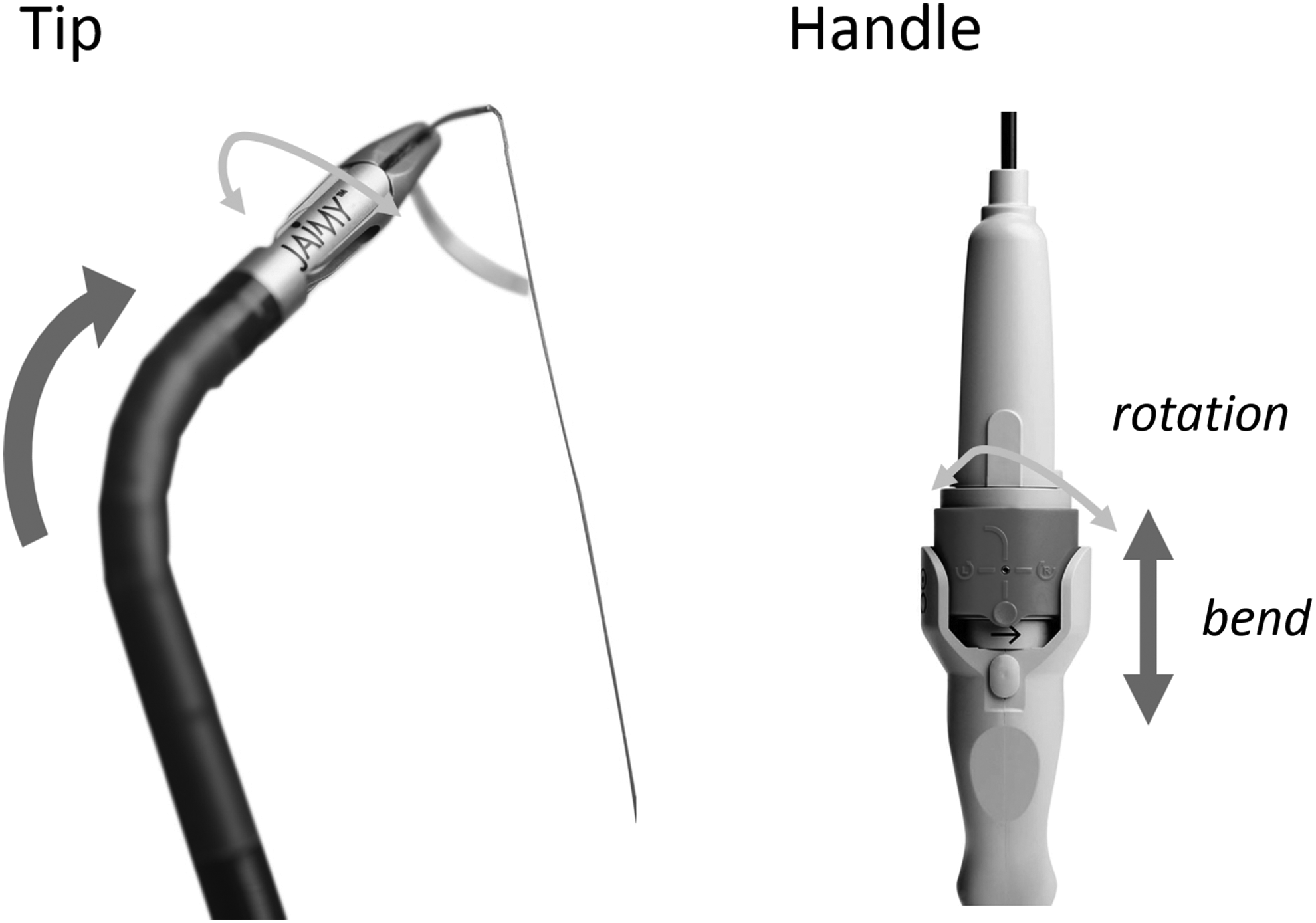
The JAiMY® needle holder The JAiMY can provide two intracorporeal DOFs using a joystick placed on an ergonomic handle: the bending of the tip of the instrument and the rotation of the jaws around their own axis. DOF, degrees of freedom.
The “Twitching Technique” Using JAiMY
First, place the suture through both sides to secure the two structures you wish to bring together (Fig. 2a–f). To perform the “twitching technique,” first grasp the long tail of the thread with the JAiMY at an appropriate position and the forceps on the needle side. Then, rotate the tip of the instrument halfway in an anticlockwise direction and slightly pull the instrument. At the same time, bring the forceps closer to the JAiMY to make a ring using the thread (Fig. 2a). Grasp the thread at the crossing point with the forceps (Fig. 2b), and then catch the short tail through the ring with the needle holder (Fig. 2c). To make a surgical square knot, rotate the tip of the needle holder halfway in a clockwise direction and slightly push the needle holder. At the same time, bring the forceps closer to the needle holder to make a ring using the thread (Fig. 2d). Grasp the thread at the crossing point with the forceps (Fig. 2e) and then, catch the short tail through the ring with the needle holder (Fig. 2f). Use a slip knot that can be tightened for the second throw.
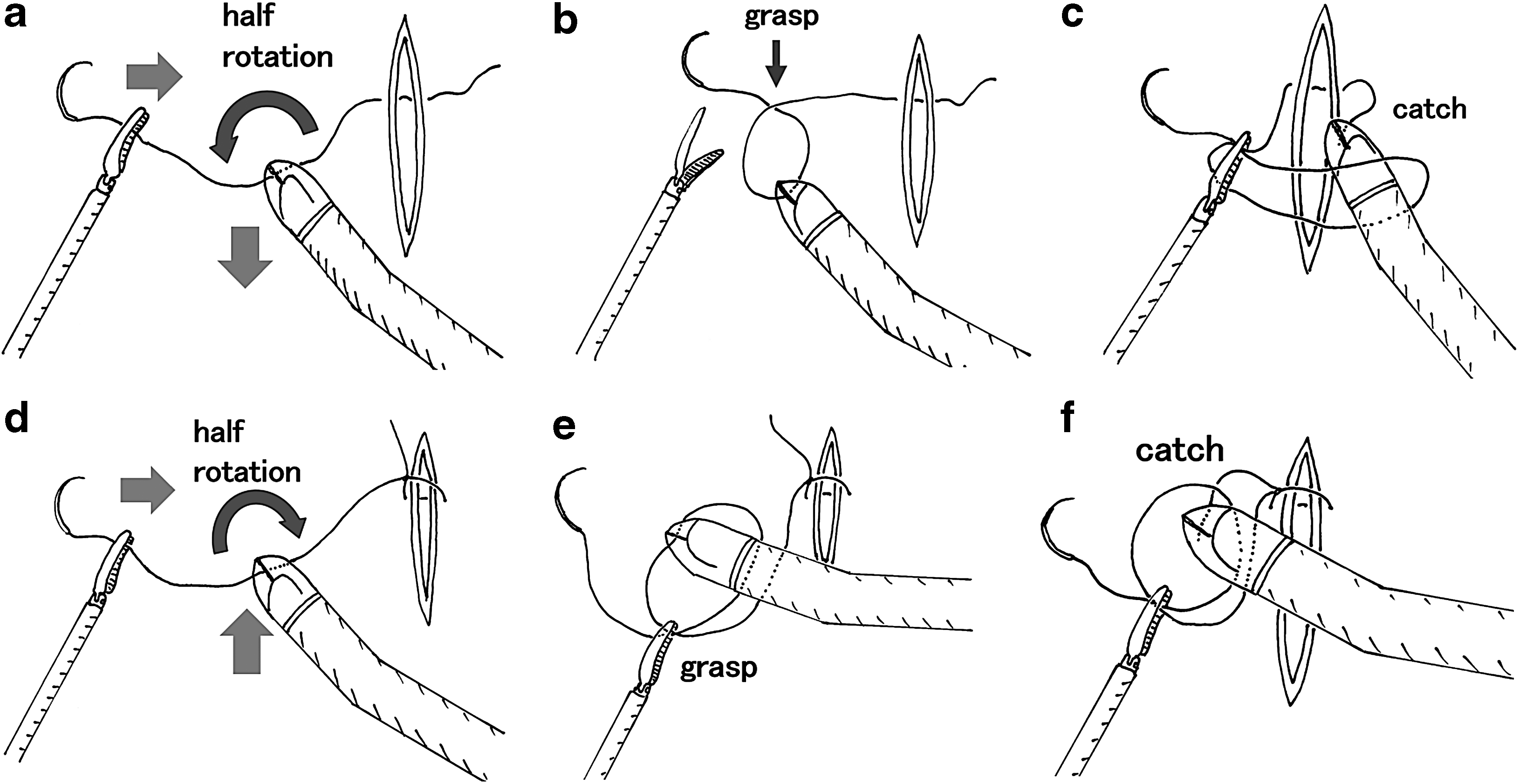
The “twitching technique.”
Case Presentation
A 1-year-old boy presented with vomiting and malnutrition because of esophageal hiatal hernia. He was being treated for single ventricle, total anomalous pulmonary venous return, and asplenia by the pediatric cardiovascular department at our hospital. His height was 62.4 cm and his body weight was 4.5 kg. An upper gastrointestinal contrast study showed herniation of the stomach to the mediastinum. He developed symptoms of severe heart failure and his NT pro-BNP level was 11,000 pg/mL (normal value <125 pg/mL). We decided to perform laparoscopic reefing of the hiatus as a minimally invasive surgical procedure to resolve the intolerance of enteral feeding due to vomiting and severe nausea.
Laparoscopic esophageal hiatus plication and gastrostomy were performed. Although a Nathanson retractor was inserted, the working space was extremely limited because of symmetrical liver, hepatomegaly due to pulmonary hypertension and adhesion between the gall bladder and the lesser curvature of the stomach (Fig. 3a). Because the right lower abdominal 5-mm port was not effective for use as a working port due to adhesion, an additional 5-mm port was inserted through the left lower abdomen (Fig. 3b). Although the angle of working ports was narrow, which would have made it difficult to perform conventional intracorporeal suture and knot placement techniques, the JAiMY and the “twitching technique” enabled steady suture placement and ligation. In particular, the “twitching technique” facilitated the stress-free placement of intracorporeal knots despite the small working apace.

The intraoperative findings.
The postoperative course was uneventful and the patient's symptoms (vomiting and nausea) showed a remarkable improvement.
Discussion
Intracorporeal sutures and knots are among the most difficult advanced techniques in laparoscopic surgery.3–6 A laparoscopic instrument only has four DOF in comparison with the arm, which has nine DOF; many surgeons feel stress as a result of this limitation. Approximately 8% of students training in laparoscopic techniques cannot surpass the proficiency threshold of advanced techniques, even after practicing such techniques >40 times. 3
The JAiMY is the only robotized needle holder that can be used through a 5-mm port. 5 The instrument possesses two more intracorporeal DOF, yaw-roll, and yaw-pitch-roll, which facilitate safe and easy intracorporeal suture placement. Furthermore, the revolving jaw around its own axis, the speed of which is controlled by a joystick, allows for the performance of a novel ligation method that we have named the “twitching technique.”
The most commonly used intracorporeal knot techniques are the C-loop and winding methods.6,7 Many experts can place intracorporeal knots easily and quickly using the C-loop method. However, the degree of difficulty increases in the presence of adverse conditions, such as forceps interference, poor visibility, and a small working space. A side-winding intracorporeal suturing method is reported to be easier to apply than the C-loop method when the angle of working ports is narrow; however, it is still difficult to apply this method in a small working space. 7 Although, there are many other reports of “new” intracorporeal knot tying methods, they require complex forceps movements.8–10 The “twitching technique” is the only knot tying method that does not involve winding the thread to the forceps. The technique is surprisingly simple and easy to perform. The forceps is only moved a very short distance; thus, the method can be safely applied in extremely small spaces.
This report is a technical report and, therefore, it is associated with some limitations. We have no data to compare the “twitching technique” with other knot tying methods regarding the facility or speed of knot tying. Further study to evaluate this technique should, therefore, be conducted.
Although the “twitching technique” itself can be performed using another revolvable forceps, the combination of the “twitching technique” and the JAiMY, which is reported to be useful for intracorporeal difficult sutures, makes it possible to perform pediatric laparoscopic surgery both easily and safely under difficult conditions.
Footnotes
Acknowledgment
The authors thank Brian Quinn for reviewing our article.
Ethical Approval
Written informed consent was obtained from the patient's parents for the publication of this report and any accompanying images. A copy of the written consent form is available for review by the editor-in-chief of this journal.
Disclosure Statement
No competing financial interests exist.