
Abstract
Abstract
Background:
Optimal elective surgery for splenic flexure cancer is unclear. Three types of surgical treatment methods are commonly used, subtotal colectomy (STC), left hemicolectomy (LHC), and segmental colon resection (SCR), but consensus is lacking as to which is the optimal method.
Materials and Methods:
We retrospectively compared clinicopathological and operative results, morbidity, mortality, and long-term survival in patients with splenic flexure cancer who underwent surgery between 1998 and 2018.
Results:
The study included 124 patients in the study. Following retrospective evaluation of the database, patients were classified into one of three groups according to the surgical approach: (1) STC (n: 41), (2) LHC (n: 55), and (3) SCR (n: 28). No statistically significant differences were found between groups regarding operative results, hospital stay, pathological data, mortality, recurrence, or long-term survival outcomes.
Conclusion:
Our results suggest that surgical procedures such as STC and LHC have no statistically significant clinical benefits over less aggressive approaches such as SCR. We thus conclude that SCR seems both a safe and effective alternative for splenic flexure tumors.
Introduction
Colon cancer is the third most common cancer in the world. 1 The clinical characteristics of this disease include a higher prevalence in males and high risks of presentations with an obstruction.2,3 Although the optimal elective surgical technique for most parts of the colon is clear, consensus is lacking regarding the most effective surgery for splenic flexure tumors.
Lymphatic drainage is particularly complex in this site. Because the splenic flexure is located between the right and left colon, it receives a dual blood supply and irrigates both regions. Therefore, more aggressive surgical procedures such as subtotal colectomy (STC) and left hemicolectomy (LHC) have been proposed. Furthermore, the surgical and long-term outcomes in splenic flexure cancer are uncertain.3–6
The aim of this study was to determine the most suitable surgical procedure for patients with a splenic flexure tumor. The results of STC, LHC, and SCR patients were compared with respect to postoperative pathological results, morbidity and mortality rates, and long-term results.
Materials and Methods
We retrospectively reviewed the data of patients who underwent elective surgery at our hospital between 1998 and 2018. All patients included had a pathologically diagnosed adenocarcinoma that was curatively resected. All tumors were located between 10 cm proximally and 10 cm distally from the splenic flexure according to the preoperative and operative data. Patients were excluded if they had a synchronous tumor, polyposis coli, preoperative remote metastasis, multiorgan resection, or obstruction.
In our clinic, splenic flexure cancers may be surgically treated with any of the three resection techniques STC, LHC, and SCR. STC is defined as resection of most of the colon by ligating the ileocolic artery, the right colic artery, the middle colic artery (MCA), and the inferior mesenteric artery, with the ileum then being anastomosed to the rectum. In LHC, the distal part of the transverse colon, the descending colon, and the sigmoid colon are resected by ligating the left branch of the MCA and inferior mesenteric artery, followed by colocolic anastomosis. In the SCR technique, the distal part of the transverse colon and the descending colon are resected by ligating the left branch of the MCA and the left colic artery (LCA), followed by colocolic anastomosis. In all the study cases, the surgical approach (open or laparoscopic) was selected according to the surgeon's judgment and recorded.
A physical workup and standard laboratory tests were conducted preoperatively in all patients. The American Society of Anesthesiology (ASA) classification was used to assess the operative risk. All patients underwent preoperative staging using computed tomography (CT) with colonoscopy. Preoperative mechanical bowel preparation and antibiotic prophylaxis were carried out. Deep venous thrombosis prophylaxis with a low-molecular-weight heparin was administered until 30 days postoperatively.
The clinical, radiological, and pathological results of the eligible patients were examined. Anatomopathological analysis of the surgical specimens included tumor extension and the number of total and metastatic lymph nodes according to the 6th edition of the American Joint Committee on Cancer classification. Postoperative morbidity was assessed according to the Clavien–Dindo severity classification. 7 Postoperative mortality was defined as death within 30 days of surgery.
According to the disease stage, all patients underwent assessment of serum carcinoembryonic antigen and carbohydrate antigen sialyl Lewis a levels, chest and abdominopelvic CT at 4–6-month intervals, and colonoscopy at 1-year intervals. Adjuvant treatments were applied according to the disease stage. Except in cases of medical contraindications, adjuvant treatment was administered in all stage III patients and also in stage II patients with a high risk of recurrence. We analyzed local and distant recurrence and also global survival.
Statistical analysis was performed using SPSS v20 software. The chi-square and Fisher's tests were applied, as appropriate, to compare categorical variables. Quantitative data were compared using ANOVA. The survival rate was analyzed using the Kaplan–Meier method and comparedwith the log-rank test. A two-tailed value of P < .05 was considered significant statistically.
Results
Of the 124 patients, 41 (33%) underwent STC, 55 (44%) LHC, and 28 (22%) SCR (Table 1). Age, gender, ASA score, grades, and tumor stages were similar in all three groups (Tables 1–4). A laparoscopic approach was performed in 61% of patients. The rate of laparoscopic surgery was 61% in STC patients, 58% in LHC patients, and 93% in SCR patients; the difference between groups was significant (P = .001). The rates of conversion from laparoscopy to open surgery were 19% in the STC group, 28% in the LHC group, and 7% in the SCR group. There was no significant difference between the groups with respect to operating time (Table 1).
Demographic and Operatory Data
Mean ± SD.
STC, subtotal colectomy; LHC, left hemicolectomy; SCR, segmental colon resection; ASA, American Society of Anesthesiology.
Postoperative Data
Median (±SD).
STC, subtotal colectomy; LHC, left hemicolectomy; SCR, segmental colon resection.
Postoperative Data, Laparoscopy Resection
Mean ± SD.
STC, subtotal colectomy; LHC, left hemicolectomy; SCR, segmental colon resection.
Anatomopathological and Oncological Data
Mean (±SD).
STC, subtotal colectomy; LHC, left hemicolectomy; SCR, segmental colon resection; TNM, tumor node metastasis staging.
When the complications according to the Clavien–Dindo classification were examined, no significant difference was found. Postoperative morbidity was 25% in the laparascopic STC group, 17% in the laparoscopic LHC group, 23% in the laparoscopic SCR group. Postoperative morbidity was 31% in the STC group, 25% in the LHC group, and 28% in the SCR group. No statistically significant differences were observed between the STC, LHC, and SCR groups with respect to postoperative morbidity. No statistically significant differences were observed between the laparoscopic STC, laparoscopic LHC, and laparoscopic SCR groups with respect to postoperative morbidity. One patient who underwent laparoscopic STC died on day 3 due to pulmonary sepsis. There were no statistically significant differences between the STC, LHC, and SCR groups with respect to the length of hospital stay (Tables 2 and 3).
According to the harvested lymph node counts, the STC group had the highest number of extracted lymph nodes, but no statistically significant differences were found between the groups. There were no differences between the groups regarding the number of metastatically positive lymph nodes removed (Table 4).
The long-term follow-up period was determined as mean 84 (±64) months in the STC group, followed by LHC 54 (±39) months and SCR 35 (±24) months; differences between groups were not significant (Fig. 1). Local recurrence was detected in two (2%) patients who underwent LHC. When distant organ metastases were considered, the most frequently affected organ was the liver, followed by the lung and brain in two cases (5%) in the STC group, in three cases (5%) in the LHC group, and in three cases (10%) in the SCR group; there were no statistically significant differences between the three groups (Table 5).
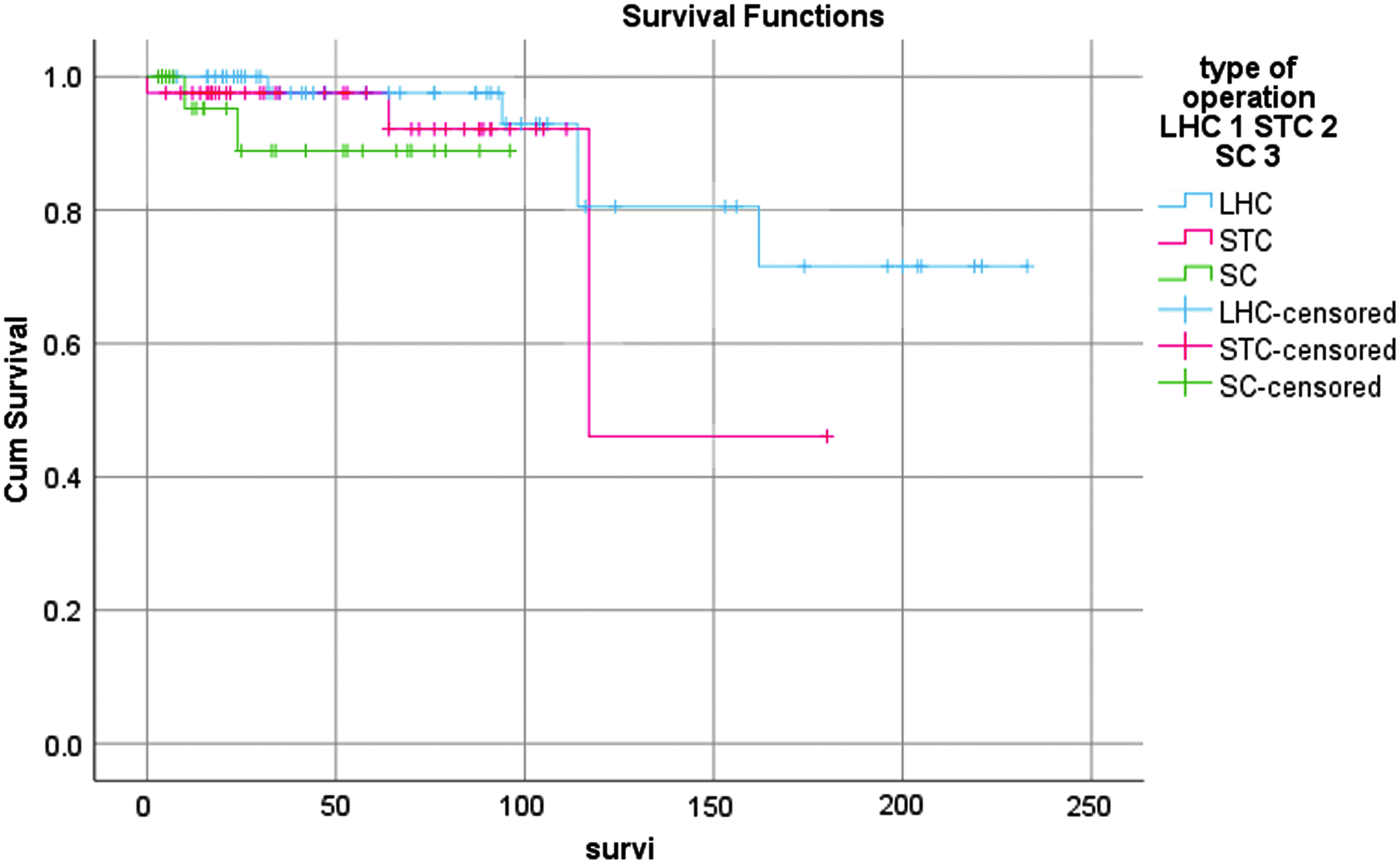
Survival according to surgical technique. Red line: subtotal colectomy; blue line: left hemicolectomy; green line: segmental colon resection. Note that there are no significant differences between the curves (log rank: 0.306).
Long Term
Mean ± SD.
STC, subtotal colectomy; LHC, left hemicolectomy; SCR, segmental colon resection.
Discussion
Although there is no consensus on the optimal treatment of splenic flexure cancer, there are insufficient publications in the literature to permit meaningful conclusions.8–13 The objective of this study was to contribute to the better surgical procedure for patients with a splenic flexure tumor. In the current study, the groups with extensive resection showed more morbidity in terms of number, but this was not statistically significant. The number of harvested lymph nodes was similar in all groups. The data showed no differences between groups with respect to clinicopathological data and long-term oncological outcomes.
The lymphatic drainage of splenic flexure is complex due to the blood supply of this region.8,13,14 Some surgeons consider splenic flexure tumors to have a worse prognosis than other parts of the colon. 5 Therefore, some surgeons prefer extended resection and lymph node dissection. 5 However, in the two publications in which splenic flexure cancer was examined scintigraphically, Watanabe et al. 15 found that in 61% of patients, lymph flow was directed to the area at the root of the inferior mesenteric vein (IMV). They considered this finding explained the importance of the area of the root of the IMV and stated that the left branch of the MCA may not be necessary. In contrast, Vasey et al. 16 reported that in 96% of patients, lymph drainage was through the left colic pedicle, and toward the left branch of the MCA in only a few patients. Griffiths also reported that the splenic flexure is supplied by terminal branches of the LCA in ≈90% of cases, with the left branch of the MCA supplying the remainder. 14 In another study, Nakagoe et al. 13 reported invaded lypmh nodes only in the paracolic, left branch of the MCA and LCA. When these studies are examined, IMV root and LCA appear to be important in splenic flexure cancer surgery Based on this point of view, the researchers claimed that SCR and ligation of LCA and IMV from the mesenteric root were adequate and that these procedures could avoid unnecessary resections of the MCA or the inferior mesenteric artery. In SCR, the lymph nodes in the IMV root are dissected and the LCA binds to the root of the IMA. According to the American Pathology Association, the harvesting of 12 lymph nodes is sufficient in colon cancer.17,18 In our series, the number of lymph nodes removed in SCR was similar to that in other studies,8–10 and therefore, lymph node dissection of splenic flexure cancer appears to be sufficient oncologically in SCR. Although more lymph nodes were harvested in the STC group, which is consistent with the larger extension of colon resected, there was no significant difference between groups.
In a study of 30 cases of STC and 137 SCR operations for colon cancer, Kim et al. 6 reported no differences between groups with respect to survival and disease-free survival. Many studies have shown that SCR is as safe as other extended resections and probably produces very similar oncological results.8–10 In the current study, no significant difference was determined between patients who underwent surgery of SCR, LHC, or STC for splenic flexure cancer with respect to survivals and distant or local reccurence.
Moreover, extended resections have a negative impact on the postoperative quality of life of patients, as has been shown in many studies, and postoperative morbidity and mortality rates are higher. 19 You et al. 20 reported that 521 patients with SCR had a better quality of life and bowel function than those with extensive resection, although perioperative complications did not differ.
Some surgeons have recommended extended colonic resection and splenectomy because of direct lymphatic drainage of the splenic flexure toward the splenic hilum. 5 Splenectomy increases morbidity and mortality rates and decreases life quality. However, previous studies have reported that metastasis to splenic flexure cancer is very rare and splenectomy is unnecessary. 13 Therefore, splenic hilum dissection should be limited to cases of locally advanced cancer with suspicious secondary lymph nodes, perhaps highlighted with a preoperative imaging method.
In many studies, laparoscopy has been shown to have advantages over open surgery such as less postoperative pain, better pulmonary function, and less postoperative ileus. 11 Recent studies have demonstrated the feasibility and oncological safety of laparoscopic treatment for splenic flexure cancer.8–12 In the current study, the rate of laparoscopic SCR was higher and the conversion rate was lower in SCR.
Limitations of this study include the retrospective design, a difference in the follow-up time between the surgical techniques, the use of either laparoscopy or open surgery, and a lack of study on quality of life. Further prospective randomized clinical trials are warranted.
Conclusions
The results of this study showed that SCR especially lapararoscopic approach clinicopathological, operative results, postoperative results, long-term oncologic outcomes were equal to other surgical procedures. Since more aggressive surgical approaches such as STC and LHC do not seem to provide more statistically significant clinical benefits, SCR can be concluded as a safe and effective alternative surgical approach for splenic flexure tumors.
Statement of Ethics
The authors have no ethical conflicts to disclose, and have complied with all ethical standards.
Footnotes
Acknowledgment
There are no acknowledgments for this article.
Authors' Contributions
R.B.: principal author, J.B.R.: primary operator, data collection and work, M.C.M.: primary operator, data collection and work, M.P.H.: primary operator, data collection and work, E.M.T.S.: primary operator.
Disclosure Statement
No competing financial interests exist.