
Abstract
Abstract
Background:
Esophageal hiatal hernia can be classified into four types. It has been reported that most complications occurred in type II–IV hernia patients compared with type I hernia. This study aimed to investigate and compare the efficacy, complications, and long-time outcomes after laparoscopic fundoplication between type I and type II–IV hernia patients.
Materials and Methods:
Medical records of 110 children who underwent laparoscopic fundoplication during 2008–2017 in our institution were retrospectively analyzed. Information of postoperative symptoms, complications, and quality of life (QOL) were compared between different types.
Results:
All 110 children underwent laparoscopic fundoplication, and none converted to open surgery. Type I and type II–IV each accounted for 50.9% and 42.8%. There was no significant difference in the perioperative data between type I and type II–IV esophageal hiatal hernia. The follow-up information of 81 children was obtained. The scores of postoperative symptoms were comparable between type I and type II–IV group, except the severity score of reflux symptom was higher in type I hernia patients (P = .032). The difference in the incidence of postoperative complications and recurrence after laparoscopic fundoplication between type I and type II–IV hernia was not significant. The QOL in three aspects improved significantly after laparoscopic fundoplication in all types of esophageal hiatal hernia.
Conclusions:
Laparoscopic fundoplication was an effective approach for all types of esophageal hiatal hernia. Type II–IV hernia could obtain a comparable therapeutic effect and long-time outcome compared with type I hernia despite its increased complexity of the anatomy and the required laparoscopic repair procedure.
Introduction
Congenital esophageal hiatal hernia is a pediatric disease caused by congenital diaphragm malformation. The main pathological change is the enlargement of esophageal hiatus, weakness of the tendon of diaphragm around the esophagus, causing the esophageal ventral section, the cardia and the fundus to enter the mediastinum through the enlarged esophageal hiatus as the abdominal pressure increased. 1 Hiatal hernia can be divided into four types, including sliding hernia (type I) and three types of paraesophageal hernia (type II–IV).2,3 The upper gastrointestinal contrast figure of each type is shown in Figure 1. The most popular procedure for congenital hiatal hernia in children is to repair the esophageal hiatus and perform fundoplication laparoscopically. The number of studies focused on comparing outcomes of laparoscopically repaired type I and type II–IV hernia is small, and one of them suggested that postoperative complications were more likely to happen in type II–IV hernia patients.4,5 Therefore, the aim of this study is to investigate and compare the efficacy, complications, and long-time outcomes after laparoscopic fundoplication between type I and type II–IV esophageal hiatal hernia in children by retrospectively analyzing clinical and follow-up information of patients who underwent laparoscopic fundoplication in our hospital for the past 10 years.
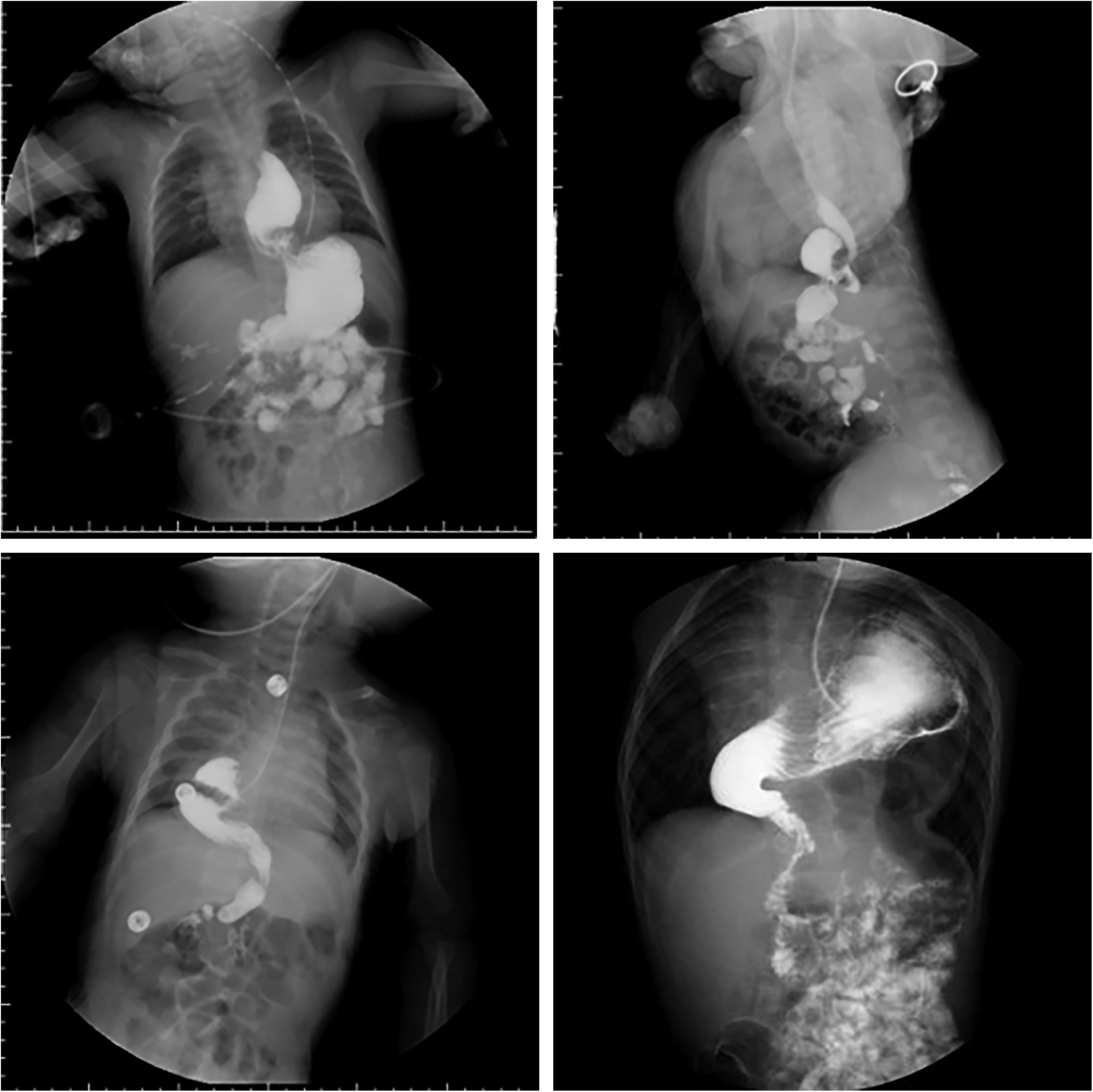
These four figures were upper gastrointestinal contrast figures obtained from patients' medical records in our institution. The figure on the top left, top right, bottom left, and bottom right represented for type I, type II, type III, and type IV esophageal hiatal hernia, respectively.
Materials and Methods
Study population
The clinical data of 110 children undergoing laparoscopic fundoplication for congenital esophageal hiatal hernia in our hospital from 2008 to 2017 were retrospectively reviewed. The patient population was 67.3% male, with a mean age of 10.42 ± 11.14 months and a mean weight of 7.34 ± 3.33 kg at operation. The diagnosis and classification of all patients were validated by upper gastrointestinal contrast and/or chest and abdominal computed tomography. According to Shinner classification, type I, II, III, and IV each accounted for 50.9%, 17.3%, 6.4%, and 19.1%. And 7 patients classified as recurrent hernia were excluded. The most common first symptom was vomiting (74.5%), followed by recurrent pneumonia (16.4%). Perioperative issues (time of operation, length of hospital stay, and time to full feeding), postoperative symptoms (dysphagia, vomit, and food reflux), complications (esophageal stenosis and gastroesophageal reflux), quality of life (QOL), and recurrence were evaluated by online questionnaire and telephone follow-up. Postoperative symptoms were evaluated by severity scores of 1–7, indicating a range from mild to worse. QOL questionnaire was composed of three aspects, including daily care and the overall condition of the child, child and parents' overall QOL, and child's special medical needs. Scores of each question in QOL questionnaire ranged from 1 (best) to 5 (worst). 6
Operative technique
All patients underwent laparoscopic esophageal hiatal hernia repair and fundoplication according to patients' condition and intraoperative situation, which were mainly conducted by two sophisticated pediatric surgeons. Enlarged esophageal hiatus was closed by performing 2–3 sutures of bilateral diaphragmatic crura, and in the meantime, making sure that the ventral esophagus length was 2–3 cm. Besides the repair of esophageal hiatal hernia, laparoscopic fundoplication was performed in all patients to prevent postoperative gastroesophageal reflux. In this study, two kinds of fundoplication were performed, Nissen-Rossetti and Thal fundoplication. Nissen-Rossetti fundoplication created a 2–3 cm-long posterior wrap around the lower esophagus by placing a total of 2–3 sutures, including 1 suture from the fundus to esophagus and 1–2 sutures from fundus to fundus. Thal fundoplication created a partial (180–270°) anterior wrap by suturing the fundus anteriorly to the esophagus using ∼4 sutures. A supporting tube was placing in the esophagus to prevent postoperative esophagus stenosis caused by a too-tight wrap. Most patients underwent Nissen-Rossetti fundoplication, which eliminated the need to release splenogastric ligament, shortened operation time, reduced surgical damage, and could achieve comparable antireflux effect when compared with conventional Nissen fundoplication.
Statistical analysis
Baseline information, perioperative data, and postoperative outcomes were collected and analyzed retrospectively. Variables were demonstrated by mean with standard deviation or frequency with percentage. Student's t-test and chi-square or Fisher's exact test was used for univariate analysis to compare postoperative symptom severity scores, QOL values, incidence of postoperative complications, and recurrence between patients with different type hernia. P value of <.05 was considered statistically significant.
Results
Baseline data and perioperative outcomes
Of 103 patients, 90 (87.4%) patients underwent laparoscopic Nissen-Rossetti fundoplication and 13 underwent Thal fundoplication. None of these patients was converted to open surgery or experienced severe intraoperative complications. Meshes were only used in two cases.
Perioperative outcomes are given in Table 1. There was no difference of average time of operation, length of hospital stay, and time to full feeding between type I and type II–IV hernia.
Comparison of Perioperative Outcomes Between Type I and Type II–IV Hernia (N = 103)
The values of length of hospital stay, time of operation, and time to full feeding are given as mean with standard deviation.
Postoperative follow-up and outcomes
The postoperative data and QOL of 81 (78.6%) patients were obtained by online questionnaire and telephone follow-up, including 2 recurrent patients who were excluded from analysis. The length of follow-up ranged from 12 to 124 months.
There was no difference between type I and type II–IV hernia in the severity score of several postoperative symptoms, including abdominal pain, dysphagia, and vomit. However, type I group had higher severity score of reflux symptom (P = .032) than type II–IV group. In type I group, 6 patients had esophageal stenosis shortly after surgery, whereas 4 in type II–IV group. Among these 10 patients, 7 patients needed esophagus dilation to relieve esophagus stenosis symptoms, 5 patients in type I group and 2 in type II–IV group. Postoperative esophageal stenosis improved during recovering or by dilation. At the time of follow-up, only 1 patient still had dysphagia and esophagus stenosis. Nine patients had symptoms of gastroesophageal reflux after fundoplication and 3 of them still needed antacids. Recurrence detected in computed tomography or upper gastrointestinal contrast test occurred in 5 patients in type I group and 5 in type II–IV group, and the difference of recurrent rate between two groups was not significant. Of these 10 patients, 5 recurrence occurred within the first year after surgery and all 10 happened within the first 3 years. Secondary surgery of 7 recurrent hernia were all performed laparoscopically, during which we found that the most common cause of recurrence was the impropriate closure of enlarged esophageal hiatal or the loosening of sutures between diaphragmatic crura (6/7), followed by loosening of fundus wrap (1/7).
The QOL of all three aspects improved significantly after laparoscopic fundoplication in all types of esophageal hiatal hernia children, and there was no difference of postoperative QOL between two groups. Postoperative information is given in Table 2.
Comparison of Postoperative Outcomes and Follow-Up Data Between Type I and Type II–IV Hernia (N = 79)
Postoperative symptoms values are given as mean with standard deviation. Postoperative symptoms values were given by patients' parents ranging from 1 (mild) to 7 (severe).
Complications and recurrence values are given as number with percentage.
Postoperative QOL values are given as mean with standard deviation. The answer to each question in the three aspects of postoperative QOL was given from 1 (best) to 5 (worst).
QOL, quality of life.
Discussion
Several studies have shown that laparoscopic esophageal hiatal hernia repair and fundoplication can get similar effectiveness, lower rate of postoperative complications, and shorter length of hospital stay compared with conventional open surgery.7,8 Therefore, since the first laparoscopic Nissen-Rossetti fundoplication performed in our institution guided by doctor Donald Liu from University of Chicago Comer Children's Hospital in 2000, patients diagnosed with congenital esophageal hiatal hernia and in line with the surgical indications received laparoscopic hernia repair and fundoplication. Surgical contraindications of laparoscopic fundoplication included premature infants, neonates who weighed <2 kg or presented with severe congenital malformation, cardiopulmonary dysfunction, severe pulmonary infection, coagulopathy, and history of abdominal surgery.
Fundoplication can be mainly divided into two types: total wrap and partial wrap. Laparoscopic Nissen fundoplication, one kind of total wrap fundoplication, is the most commonly used procedure in all age groups, which was described as the gold standard for antireflux procedure by a report of 20-year experience with ∼2000 pediatric patients. 9 Compared with conventional Nissen fundoplication, Nissen-Rossetti wrap can achieve same antireflux effect with a lower risk of injuring the spleen and bleeding from short gastric vessel due to the preservation of short gastric vessel during the procedure. A study of 1000 cases underwent Nissen-Rossetti fundoplication, 428 performed laparoscopically, has validated its antireflux effectiveness. 10 During 19-year experience of laparoscopic fundoplication practice for esophageal hiatal hernia patients in our institution, Nissen-Rossetti fundoplication was the first choice to do an antireflux procedure, and Thal fundoplication was performed only when patients' fundus was too small to create a total wrap. The usage of meshes in hiatal hernia repair was not a routine procedure in our institution and meshes were only used in 2 cases among 110 esophageal hiatal hernia patients during the past 9 years. One patient was 3 months old and has received laparoscopic repair of congenital diaphragmatic hernia 3 days after birth, whose left crura of diaphragm development was poor and posterior part of the diaphragm was loose, so a mesh was placed to reinforce the weak part of diaphragm. In the other case, the patient was diagnosed with recurrent esophageal hiatal hernia 8 months after the first laparoscopic hiatal hernia repair. During the secondary operation, two sides of crura of diaphragm were separated because the right crura of diaphragm was found to be cut by former sutures, so two sides of crura of diaphragm were stitched up and a mesh was placed under the suture line.
Based on current researches, type II–IV hiatal hernia was considered to have more complicated pathological anatomy and difficult laparoscopic operation than type I hernia. A study on the comparison of outcomes after laparoscopic repair and fundoplication between type I and type II–IV hiatal hernia, which composed of 2047 patients in adult population, suggested that the higher incidence of postoperative complications and recurrence occurs in type II–IV hernia. 5 Mikael et al. conducted a survey on the results of laparoscopic repair in type II–IV esophageal hiatal hernia and they proposed the feasibility and effectiveness of laparoscopic approach for paraesophageal hernia. 11 Our study, including all four types of esophageal hiatal hernia, concluded that type II–IV hernia can achieve comparable outcomes without increasing the incidence of postoperative complications and recurrence, which supported the conclusion of Mikael's study.
Postoperative symptoms have been analyzed in this study; it was noteworthy that type I group had higher severity score of postoperative reflux symptom, which was likely related with its pathological anatomy that the gastroesophageal junction moved into thorax and caused gastroesophageal reflux even before the surgery. Most of postoperative symptoms can gradually resolve over time; patient still needed antacids and had dysphagia at the time of follow-up was 1 and 1 in all types of esophageal hiatal hernia, respectively.
The most commonly seen intra- and postoperative complications include vagus nerve injury, partial spleen infarction, esophageal stenosis, and gastroesophageal reflux. 12 Based on our experience, vagus nerve injury could be prevented by avoiding excessive dissection of hernial sac near the posterior right wall of esophagus, and partial spleen infarction has been discussed three paragraphs earlier. Some operative skills have been applied in our procedure, such as using an esophagus supporting tube according to patients' age and size when repairing the hiatal hernia.
A research aimed to identify the risk factors in esophageal hiatal hernia patients who underwent laparoscopic repair and fundoplication for recurrence in adult has shown that preoperative type II anatomy and hernias contained a large part of stomach related with higher recurrence rate (not significantly). 13 In our study, recurrent rate in two types of hernia did not differ. Refundoplication was performed in 7 recurrent cases, and mesh was only applied in 1 case to close the enlarged hiatal hernia because the right diaphragmatic crus has been cut by former suture. Therefore, closing the hiatal hernia with a proper tightness is a critical step to avoid recurrence.
In conclusion, laparoscopic hernia repair and Nissen-Rossetti fundoplication is effective and safe for esophageal hiatal hernia patients. Type I hernia patients might be more likely to have postoperative gastroesophageal reflux symptoms due to its preoperative anatomy. Type II–IV hernia, although, having more complicated pathological anatomy and requiring difficult surgical procedure, can also achieve comparable antireflux effect and long-time outcome.
Footnotes
Acknowledgment
The authors thank Nurse Shourong Huang for her assistance with telephone follow-up.
Disclosure Statement
All authors have seen and approved the final version of this article. No competing financial interests exist.