
Abstract
Abstract
Aims:
To assess the feasibility, safety, 1-year postoperative quality of life, and 2-year postoperative local recurrence of b-shaped laparoscopic dual anastomosis (bSLDA) technique in laparoscopic anterior resection (LAR) for mid-low rectal cancer.
Methods:
In this case-matched study, we retrospectively reviewed the database of 120 patients with mid-low rectal cancer who underwent LAR in Tangdu hospital between June 2014 and January 2017. The database included baseline characteristics, operative data and short-term outcomes, specimen, and pathological results. Among all the participants, 60 patients underwent bSLDA and 60 patients underwent conventional laparoscopic dual anastomosis (CLDA). After lymph node dissection and rectal dissociation, patients in the bSLDA group received the operation as follows: (1) the rectum distal end was closed vertically instead of horizontally; (2) the anastomosis was conducted in an end-lower corner of rectal stump. We also performed at least 2 years of follow-up (the median follow-up was 36 months, ranging from 24 to 54 months), including 2-year recurrence scores, 1-year low anterior resection syndrome (LARS) scores, and QLQ-C30 scores.
Results:
In this case-matched study, there were no differences between bSLDA group and CLDA group in operative data and short-term outcomes, which suggested that bSLDA and CLDA were equally safe. Furthermore, compared with CLDA group, bSLDA group had no statistical difference in the rate of anastomotic leakage (AL), but there was a trend that the rate in bSLDA was lower. In postoperative specimen data, the maximum and minimum edge distances of the ring from the rectal stump are longer in the bSLDA group. What is more, in the EORTC QLQ-C30 (version 3.0), the diarrhea score in bSLDA group was statistically lower (better) than in CLDA group (P = .043). Although bSLDA group had no significant differences in the LARS scores with CLDA group, there was a trend that the LARS scores were lower in bSLDA. At last, the 2-year local recurrence rate in both groups was not significantly different.
Conclusions:
The bSLDA technique is safe and accessible, which may reduce the incidence of AL to some extent. Therefore, it could be an alternative to laparoscopic proctectomy for mid-low rectal cancer and may also improve postoperative quality of life for many patients.
Background
Based on recent technical improvements, it was demonstrated by several randomized trials that laparoscopic anterior resection (LAR) is safe and feasible.1–3 However, laparoscopic proctectomy was sometimes limited due to difficulties related to rectal excision and anastomosis within the narrow pelvic space. What is more, because of the technical difficulties in laparoscopic proctectomy, the incidence of early complications, especially anastomotic leakage (AL), is often disappointing. 4
AL is considered as the most anxious complication after LAR. It was reported that the incidence of AL ranged from 3.6% to 21%.5–9 AL brings patients not only longer hospitalization, but also lowers patients' survival rate and postoperative life quality.10–12
The reconstruction of the digestive tract especially for anastomosis after LAR was greatly facilitated by the double-stapling technique (DST). In the DST, there are at least two staple lines crossed by each other, which create stapled corners known as “dog ears,” potentially forming vulnerable areas.4,13
To overcome these difficulties, various methods have been suggested, including the single-stapled method, double-purse string method, and bioabsorbable staple-line reinforcement.14,15 However, all the aforementioned methods require advanced-technique and are highly difficult, requiring a longer operation time.
To solve the aforementioned problems, we adopted a modified dual anastomosis (end-lower corner anastomosis), which locally formed a structure similar to “b” at the anastomosis, so we named it “b-shaped” anastomosis. This study assessed the feasibility, safety, postoperative quality of life, and local recurrences of the b-shaped laparoscopic dual anastomosis (bSLDA) technique in patients undergoing the laparoscopic surgery for the mid-low rectal cancer.
Patients and Methods
Patients
This is a retrospective case-matched study, including a total of 120 (1:1 matched) consecutive patients who underwent bSLDA (60) or conventional laparoscopic dual anastomosis (CLDA) (60) in our institution from June 2014 to January 2017.
Patient inclusion criteria were as follows: (1) age 18–70 years old; (2) endoscopic examination and biopsy proven adenocarcinoma of the rectum; (3) the tumor is ≤10 cm from the anal margin; (4) expected curative resection through LAR; and (5) preoperative T stage is less than or equal to T3, and the tumor not located in the frontier wall of the rectum. Exclusion criteria were as follows: (1) distant metastasis or invasion to adjacent organs; (2) local irresectability of the primary rectal tumor; (3) major organ functions cannot stand major operation and chemotherapy; (4) with neoadjuvant radiochemotherapy; and (5) preventive ostomy during surgery. Then we matched the patients for gender, age (± 5 years), body mass index, American Society of Anesthesiologists physical status score, and tumor-node-metastasis (TNM) stage of tumor according to the American Joint Committee on Cancer (sixth edition) TNM classification scheme.
Surgical procedure
LAR was performed by clearance of No. 253 lymph nodes, with priority given to fascial space and ensuring the preservation of the left colic artery. 16 According to the principles of total mesorectal excision, pelvic dissection was performed.17–19 After distal rectal irrigation, the rectum was closed with linear stapler (ETS 45 or ETS 60; Ethicon Endo Surgery, yellow or green cartridge).
The proximal colon was extracted through a small incision of about 4 cm in the lower left abdomen. Under the principle of oncology and reliability of blood supply, an extra 10 cm of proximal colon was resected outside the abdominal cavity. An anvil from a 29 mm circular stapler was secured to the colon with a purse string suture. The proximal colon was put back into the abdominal cavity and pneumoperitoneum was re-established. Then, the anastomosis was conducted in an end-lower corner.
Our technical procedure included the two following main parts: (1) the rectum distal end was closed vertically instead of horizontally. If the rectum was incompletely transected with <10 mm width rectum continuation, the joint of the rectum was cut directly; (2) the circular stapler puncture head was passed through the lower corner and the anvil shaft was connected to the puncture head. Subsequently, the circular stapler was closed and fired. Then, the circular stapler was pulled out and the lower corner of the rectal stump was removed (Figs. 1–3).
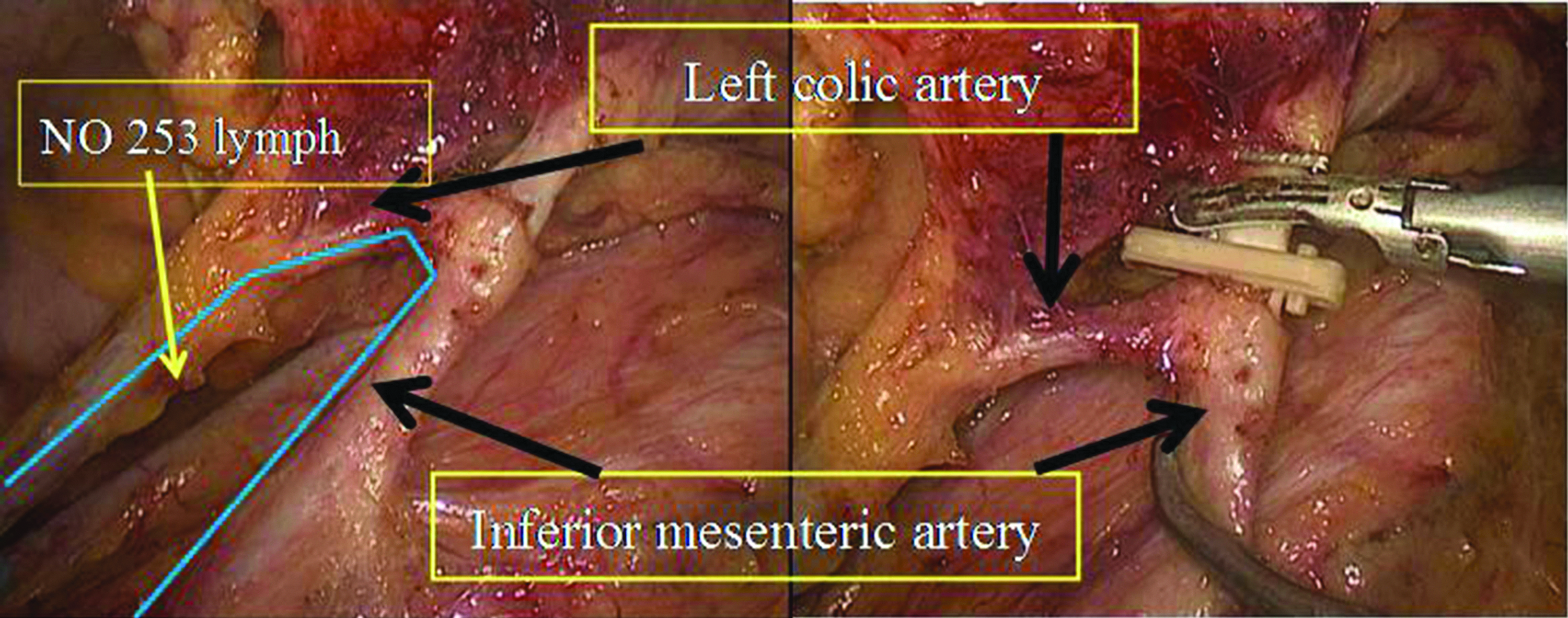
NO. 253 lymph nodes were cleared and left colic artery was preserved.
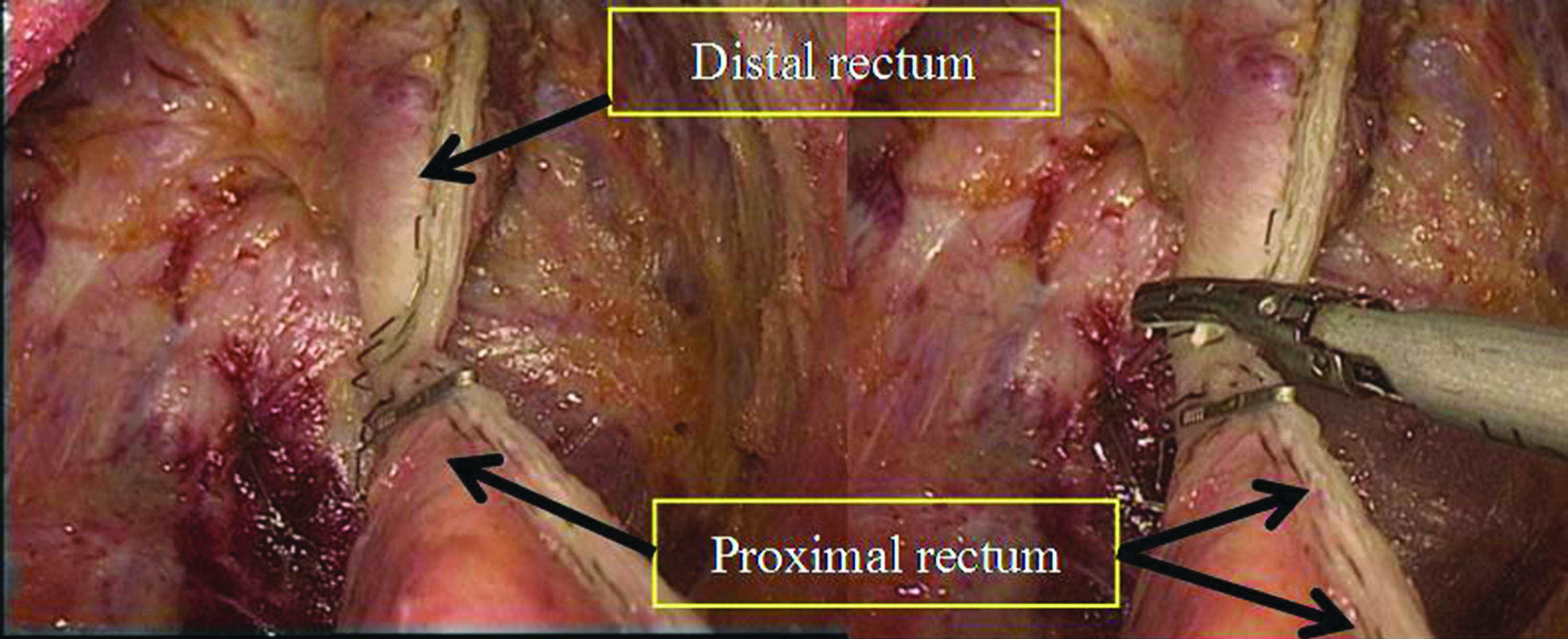
The rectum distal end was closed vertically.

The circular stapler puncture head was passed through the lower corner and the anvil shaft was connected to the puncture head.
Variables
The baseline characteristics, operative time, intraoperative blood loss, minimum edge distance of the ring from the rectal stump (RFRS), maximum edge distance of RFRS, inner diameter of RFRS (Fig. 4), postoperative recovery, AL, quality of life, and 2-year recurrence were compared between bSLDA group and CLDA group. To confirm whether recurrence occurred, we performed a follow-up through an outpatient service, telephone calls, or mailshots.
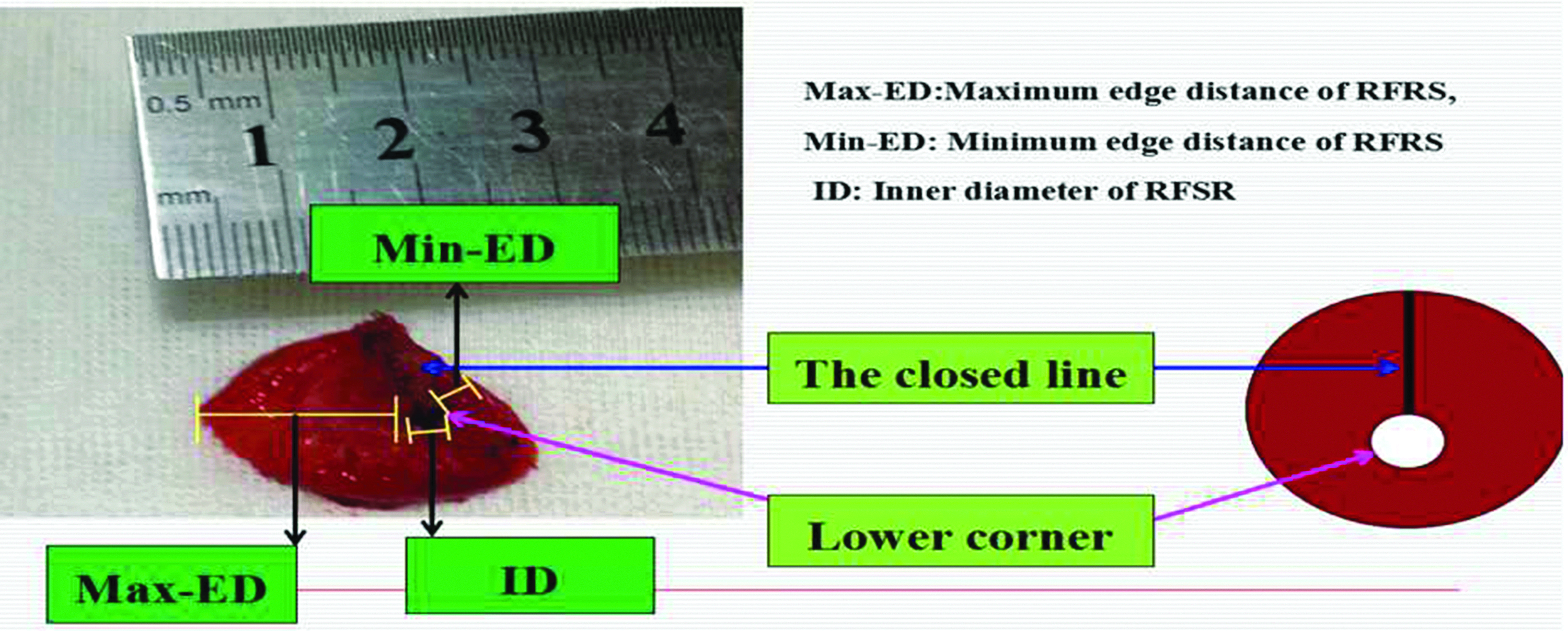
Minimum edge distance of the RFRS, maximum edge distance of RFRS, and inner diameter of RFRS. RFRS, ring from the rectal stump.
Statistical analysis
All statistical analyses were conducted using SPSS Version 16.0 (SPSS, Inc., Released 2007, SPSS for Windows, Version 16.0, Chicago, SPSS Inc.). Differences in distribution were performed using the t-test for continuous variables and Pearson chi-squared for categorical variables. P value <.05 was considered statistically significant.
Results
A total of 120 patients who underwent laparoscopic dual anastomosis for rectal cancer were considered for enrollment. There were 60 patients who performed bSLDA and 60 patients performed CLDA. There was no significant difference between the groups in baseline characteristics (Table 1).
Baseline Characteristics of the b-Shaped Laparoscopic Dual Anastomosis Group and Conventional Laparoscopic Dual Anastomosis Group
ASA, American Society of Anesthesiologists; BMI, body mass index; bSLDA, b-shaped laparoscopic dual anastomosis;
The operative data and short-term outcomes are given in Table 2, and the specimen and pathological results are given in Table 3. Comparison between two groups demonstrated no significant difference in operation time, blood loss, hospital stay, depth of tumor invasion, and level of anastomosis. The maximum and minimum edge distance was longer in the bSLDA group than CLDA group. In the CLDA group, AL occurred in 4 patients. Among them, 2 patients received reoperation and 2 patients received conservative treatment. One patient had AL and was cured after conservative treatment in bSLDA group. No perioperative mortality occurred in both groups. There was 1 case of 2-year recurrence in CLDA group and 0 case in bSLDA group.
Comparison of Operative Data and Short-Term Outcomes Between the Two Groups After Surgery
bSLDA, b-shaped laparoscopic dual anastomosis;
Specimen and Pathological Results of the Two Groups
The tumors were T3 in preoperative magnetic resonance imaging T stage and T4a in postoperative pathological T stage, which are located above peritoneal reflection.
bSLDA, b-shaped laparoscopic dual anastomosis;
The low anterior resection syndrome (LARS) and QLQ-C30 scores are given in Tables 4–5. Although bSLDA group had no significant differences in the LARS scores with CLDA group, there was a trend that the LARS scores in bSLDA were lower. In QLQ-C30 scores, the diarrhea score in bSLDA group was statistically lower (better) than in CLDA group (P = .043). The other QLQ-C30 subscale scores had no significant differences.
Low Anterior Resection Syndrome (1-Year Follow-up)
Interpretation: LARS 0–20, no; LARS 21–29, minor; LARS 30–42, major.
bSLDA, b-shaped laparoscopic dual anastomosis;
The EORTC QLQ-C30 (1-Year Follow-up)
bSLDA, b-shaped laparoscopic dual anastomosis;
Discussion
With the advancement of surgical instruments and techniques, and popularity of sphincter-preserving surgery, 20 AL is considered as the most serious problem after proctectomy. Apart from the immediate clinical outcomes, such as increased morbidity and mortality, AL also has long-term impacts, such as pelvic organ function impairment and an increase in local cancer recurrence. 21 Because there were several risk factors for AL in patients with laparoscopic rectal surgery identified in previous reports, ensuring the anastomosis is tension free and maintaining blood flow are still considered to be crucial to decreased AL incidence. 22 Laparoscopic double-stapling anastomosis has been considered as a prevalent and helpful technique. Nevertheless, this technique forms the points where the staple line intersects on both sides of the anastomosis and the crossing staple lines creates two weak points, which were often regarded as the predilection sites of AL. 23
Various modified methods have been applied to improve the double-stapled anastomotic technique, such as the single-stapled method, double-purse string method, and bioabsorbable staple-line reinforcement.14,15 However, all the aforementioned methods had advanced-technique requirements, and were highly difficult to perform, with a longer operation time.4,24,25 Chen et al. 26 suggested a modified dual anastomosis, in which the upper corner of rectum distal end was removed and anastomosed to the end of the colon. The result showed that the incidence of AL was reduced after modified dual anastomosis. Unlike their procedure, the intersection of staple lines and the remaining dog's ear are located on the anterior wall of the rectum in our study. However, our method was limited in the application of ultralow rectal cancer. In a patient with ultralow tumor, we failed to perform bSLDA and had to turn to the Parks operation, because the closed line in the rectal stump was located within 2 cm above the dentate line, and the circle staple could not be placed.
Several studies9,27–29 reported that male sex, low anastomosis, history of ischemic heart disease, preoperative chemoradiation, advanced tumor stage, and multiple firings of the linear stapler increased the risk of AL after LAR. In our study, there are 4 AL cases in the CLDA group and 1 AL case in the bSLDA group. In the case of bSLDA group, the enteroscopy showed that the circular anastomosis was intact and the leakage occurred on the stapler line of the rectum. The unsuitable cartridge might be the main reason of the leakage. Although no significant statistical difference was found in AL between the two groups, data seem to indicate that bSLDA is less likely to leak. There are several reasons for reducing AL in our study. The longer maximum and minimum edge distance in the bSLDA group means that more likely ischemic tissue is removed by anastomosis procedure, which may be the main reason contributing to the lower incidence of AL. Moreover, removing a “dog ear” may be another important reason. In addition, when the width of the rectal joint is <10 mm, the direct disconnection of the joint can reduce the number of linear staplers used, and may also be one of the reasons for the low rate of AL. In addition, reducing the use of linear staplers can also partially reduce hospitalization costs.
LARS is an important indicator of postoperative quality of life in patients with rectal cancer. However, the mechanism of LARS is not entirely clear. Many potential pathophysiological mechanisms for LAR syndrome have been proposed: internal anal sphincter dysfunction, decrease in anal canal sensation, disappearance of the recto-anal inhibitory reflex, disruption in local reflexes between the anus and the neorectum, and reduction in rectal reservoir capacity and compliance all have been described. 30 Moreover, different surgical procedures, especially the anastomosis, may also have different results. In the absence of a clear mechanism, it is difficult to have a clearer and better surgical approach, which may require further prospective studies. Chen et al. 26 considered that the corner of the rectum stump would form diverticulum effect, induce inflammatory changes, and cause postoperative anal rectal irritation. In our study, the diarrhea scores were obviously lower and the LARS scores had a lower trend in bSLDA group. Therefore, a larger sample size would likely make for more significant data, as the results of this study might be due to reasons such as less staple residue and mild relevant inflammatory response.
Our preliminary data indicate that this bSLDA technique is a safe procedure. This technique, however, may not be applicable to patients with an ultralow rectal cancer (1–2 cm above the dentate line). The small sample size and retrospective nature of the study design are the most glaring limitations within this study. In addition, in this study, all patients came from China. Thus, randomized and controlled trials should be performed in a larger and more diverse sample size in the future.
Conclusion
The bSLDA technique is safe and accessible, which may reduce the incidence of AL to some extent. Therefore, it could be an alternative to laparoscopic proctectomy for mid-low rectal cancer and may also improve postoperative quality of life for many patients.
Footnotes
Acknowledgments
The study was funded by International Cooperation Fund (2013DFA32110) and National Natural Science Foundation of China (NSFC81272275).
Disclosure Statement
No competing financial interests exist.