
Abstract
Abstract
Background:
The aim of this report was dual: (a) to describe the step-by-step standardized intraoperative percutaneous injection of carbon nanoparticles (CNPs) procedure for CNP-stained central compartment lymph nodes (CLNs) and passive display of parathyroid gland by CNP-stained thyroid in endoscopic thyroidectomy via bilateral areola approach (ETBAA) and (b) evaluation and outcomes of percutaneous injection of CNPs in total thyroidectomy plus CLN dissection through ETBAA.
Materials and Methods:
Video describes the technique of intraoperative percutaneous injection of CNPs for central compartment LNs identification, dissection, and parathyroid glands preservation in ETBAA for papillary thyroid cancer.
Results:
Supplementary video shows that after intrathyroid injection of CNPs, black carbon can be seen rapidly along the lymphatic vessels to the surrounding LNs. Parathyroid gland can be passive display when the thyroid is black and the parathyroid gland is normal in color. Intraoperative neuromonitoring (Medtronic® NIM-Response 3.0) was applied to identify recurrent laryngeal nerve and external branch of superior laryngeal nerve. No patient had any side effects of CNPs from 152 patients followed up for an average of 19.6 months (6–34 months). LNs were easily found under ETBAA. The accuracy of black-dyed LN in thyroid cancers was 95.9% (1016/1059). The number of parathyroid glands passive display was 69.9% (267/382).
Conclusions:
It is feasible to use CNPs to show CLNs in thyroid cancer during ETBAA. CNP suspension is safe for thyroidal injection.
Introduction
Endoscopic thyroidectomy via bilateral areola approach (ETBAA) is widely adopted in China because national practice tradition, intrinsic advantages in dissecting the external branch of superior laryngeal nerve and the superior thyroid vessels, realizes clearance of lateral and central compartment lymph nodes (CLNs), and fine cosmetic results.1,2
Carbon nanoparticles (CNPs) have been used in open thyroidectomy for lymph node (LN) tracer in papillary thyroid cancer (PTC).3,4
Up to now, there has been no technical report on the application and effect of CNPs in endoscopic thyroid surgery.1–10 The purpose of this video is to describe the step-by-step standardized intraoperative percutaneous injection of CNP procedure for CNP-stained CLNs and facilitate identification of parathyroid glands.
Materials and Methods
Patient
Table 1 summarizes selection and exclusion criteria for ETBAA and CLN dissection. PTC is preoperatively confirmed by fine needle aspiration cytology. Neck ultrasound examination is routinely performed.
Patient Selection Criteria for ETBAA
Low-risk factors included lesion size <4 cm, age <55 years, no prior radiation, no distant metastases, no LN metastases, no extrathyroidal extension, no aggressive variant, and no first-degree family history of thyroid carcinoma.
CLN, central compartment lymph node; ETBAA, endoscopic thyroidectomy via bilateral areola approach'; LN, lymph node.
Percutaneous CNP injection
CNP (Chongqing LUMMY Pharmaceutical Co., Chongqing, China) is approved by Chinese Food and Drug Administration (CFDA) (Permit No 2007204, registration number: National prescription H20041829). 1 CNP is applied in the form of standard CNPs suspension injection (0.5 mL:25 mg). 3 This product, which is a stable suspension of carbon pellets of 150 nm in diameter, does not enter the blood circulation and has no toxic side effects on the human body. 5 A small amount of tiny carbon particles may be captured by macrophages, and they are excreted through the lungs and intestine. 7
Approach for percutaneous injection
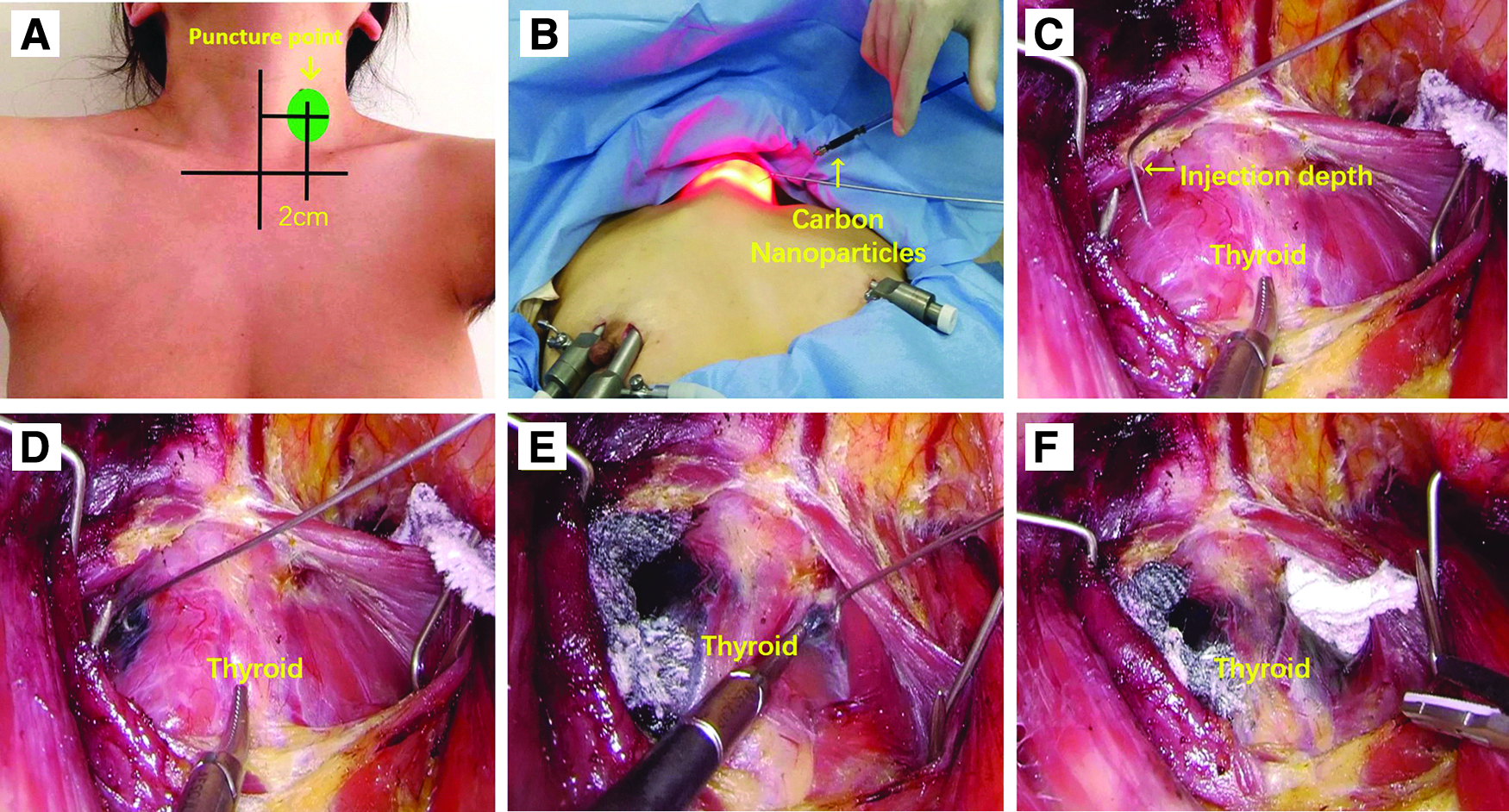
CNP suspension injection is extracted with 1 mL syringe, 70 mm long needle (outer diameter 0.71 mm, inner diameter 0.41 mm; Beijing Changchuan Medical Technology Co., Ltd., China) connected with syringe is inserted into the neck space through cervical skin puncture. On the left neck side, a 0.5 cm circle is drawn with the center of the circle at the intersection of a line 2-cm lateral to the anterior median line and a line 2-cm above the line connecting the bilateral clavicular heads (Fig. 1A). This area of the puncture is dictated by the fact that it does not interfere with the other endoscopic instruments; moreover, it remains in the center of the camera vision from right to left side. Moving 2 cm outward from the midline avoids the anterior cervical vessels.
Intraoperative CNP percutaneous injection.
Surgery
Endoscopy
ETBAA technique consists of a 10-mm curved incision made along the margin of right areola, 2–4 clock, for 10 mm trocar and 30° endoscope use. Bilateral 5-mm incisions are made on the areola, 11–12 clock, and were used for operating 5 mm trocars. The CO2 is maintained at 6 mmHg. The thyroid gland is exposed by hooking an external retractor to the strap muscle.
CNP injection
The timing for CNP injection is after anesthesia induction, placement of the trocars, working space definition and exposure of the thyroid gland. The needle enters the working space through the puncture point, and the tip of the needle is bent to mark the injection depth (half of the thyroid glandular thickness) (Fig. 1B, C). CNPs suspension is injected into the thyroid gland at the lobe of the excised side. The injection point is in the normal thyroid tissue in the middle of the lobe. The injection dose is 0.1–0.15 mL depending on the volume of thyroid gland. The injection time is usually <3 minutes. In the case of bilateral thyroidectomy, both sides are injected (Fig. 1D, E).
Needle extraction
The tip of the needle should be wiped on the surface of the anterior surface of strap muscle to avoid the subcutaneous tissue and skin being stained black. After injection, the sites of gland injection should be pressed by gauze lightly for 1 minute (Fig. 1F), to prevent the overflow of CNP suspension and pollution to surgical field. After 1 minute, ETBAA and CLN dissection can be continued.
Thyroid gland
The thyroid gland surface is evidently stained black.
LNs detection
The video shows that after intrathyroid injection of CNPs, black carbon can be seen rapidly along the lymphatic vessels to the surrounding LNs. There is no specific staining direction in CLN. If the injection method is improper, the surrounding tissues, such as the recurrent laryngeal nerve (RLN) and external branch of the superior laryngeal nerve (EBSLN), can be blackened because of CNP spillage. There is no difference between the left and the right CLN staining (Fig. 2A, B). LN staining is not related to LN size, but only to lymphatic vessels.
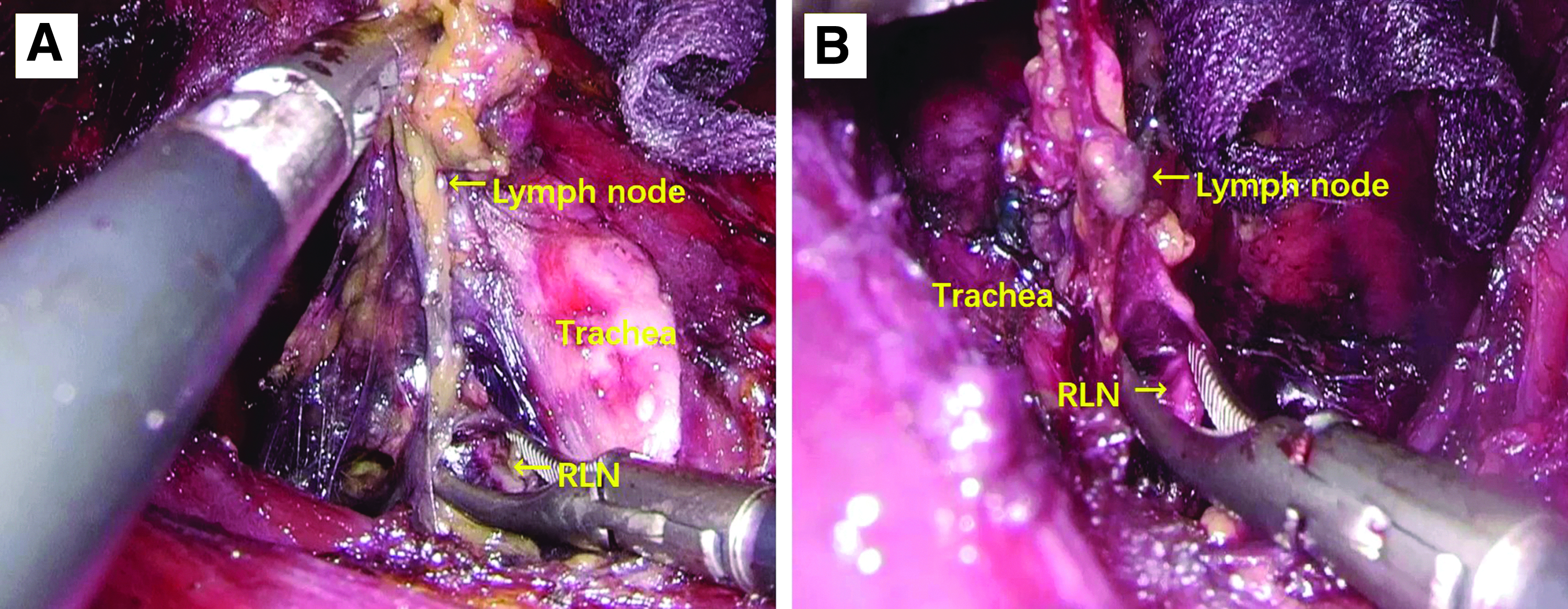
Intraoperative pictures of LNs stained with CNPs in the endoscopic surgical field.
Metastatic LNs detection
In our experience of >150 PTC, 92% of positive LNs were stained and 8% unstained. Some metastatic LNs are not stained because the lymphatic vessels may be clogged with tumor embolus. LN staining is not related to time of operation.
Parathyroid glands
If the thyroid is stained well, the upper and lower parathyroid glands can be well displayed (Fig. 3A, B).
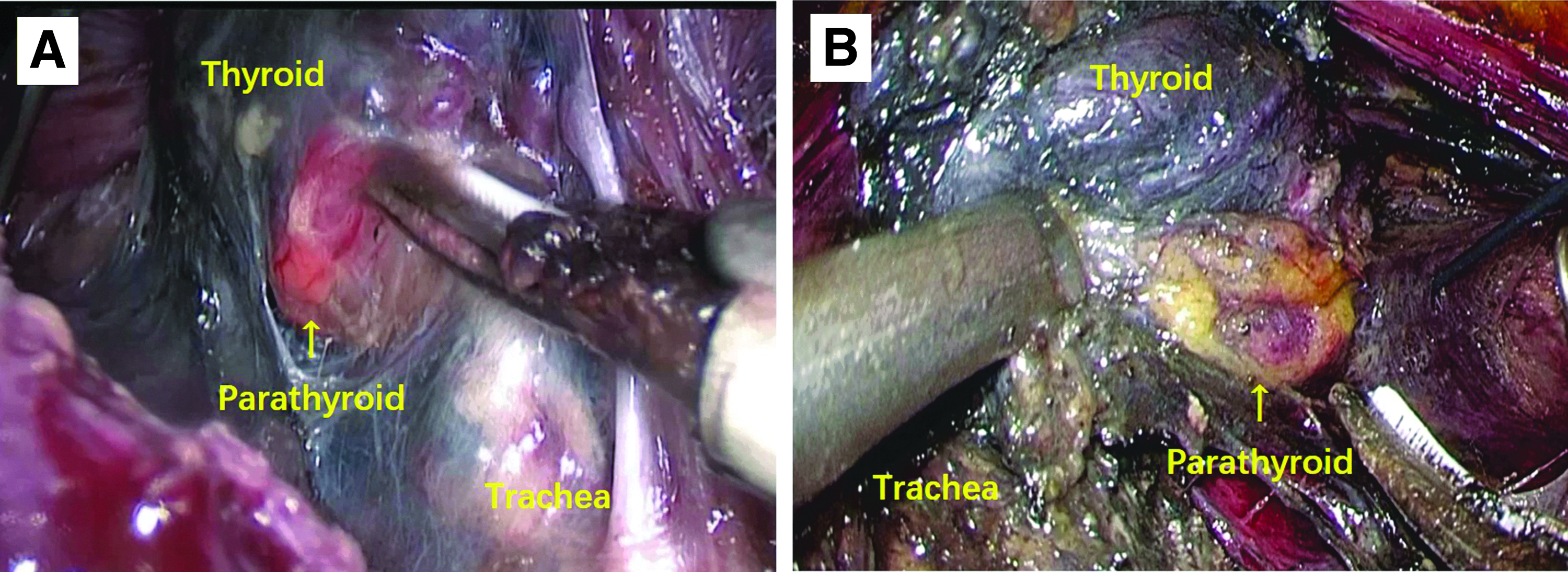
Intraoperative pictures of CNPs suspension in the endoscopic surgical field.
Recognition and protection of laryngeal nerves
RLN and EBSLN will not be stained by CNPs, unless the injection method is improper (i.e., CNP spillage). Intraoperative neuromonitoring (Medtronic® NIM-Response 3.0) is applied in accordance with international standards to identify RLN and EBSLN (Fig. 4).
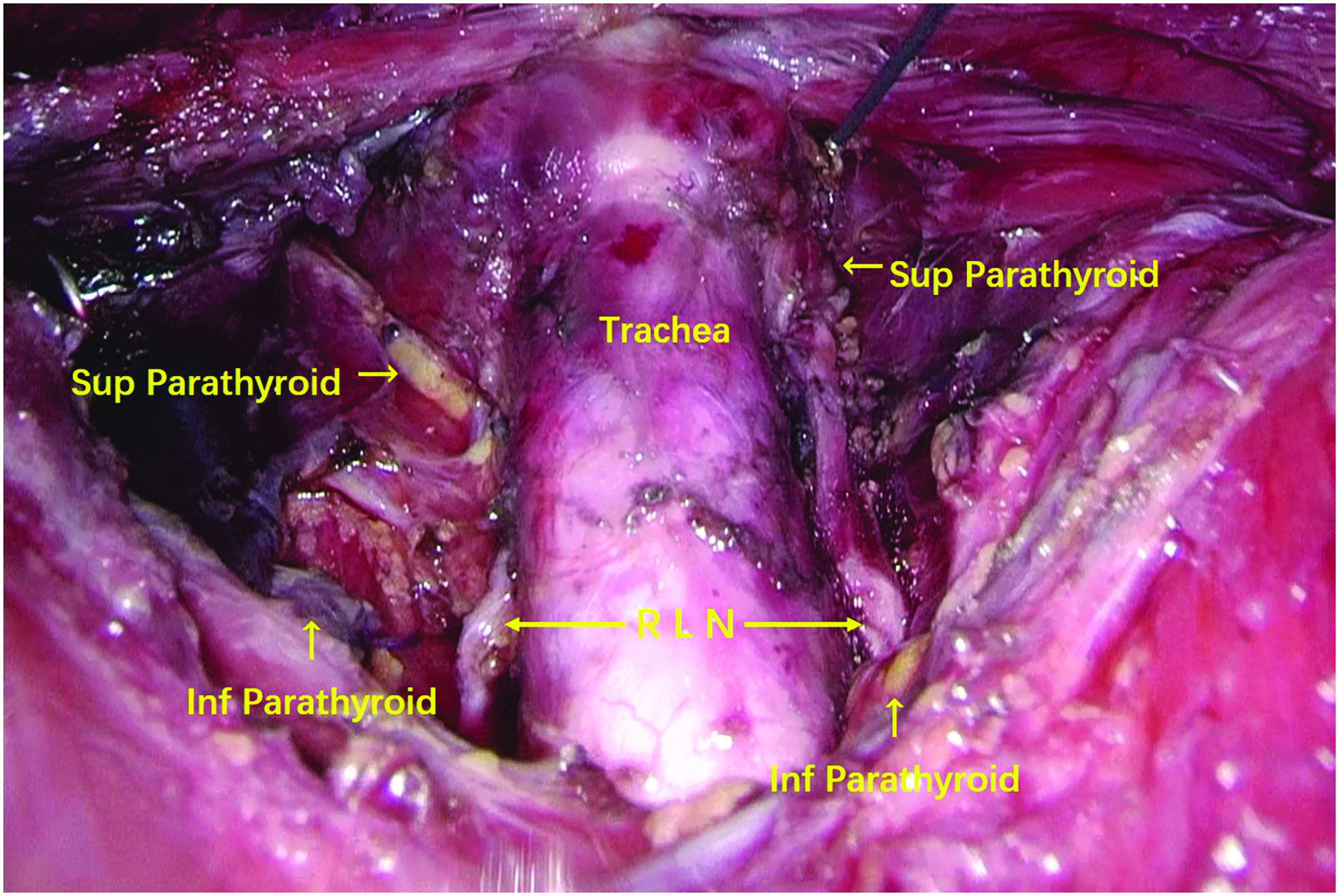
Postoperative pictures of total thyroidectomy plus central LN dissection after injection of CNPs. CNP, carbon nanoparticles; LN, lymph node.
Discussion and Conclusion
This is the first video report of application of CNPs in LN dissection and parathyroid protection during endoscopic thyroid cancer surgery. In this video, ETBAA and central compartment lymphadenectomy is offered. CLNs are defined as nodes that were black dyed by CNPs in the central compartment. We selected to perform intraoperative (not preoperative) dye injection, which is an easier, painless, less time-consuming, not logistically difficult, and similar effective method of open surgery. Patient with PTC underwent CNP injection and surgery in the same session. Our CLN staining rate was 96%, somewhat similar to the rate reported in open thyroidectomy studies about PTC. Furthermore, this video describes the identification of parathyroid glands indicating that CNPs could help improve the discovery rate and preservation of parathyroid glands. In conclusion, it is feasible to use CNPs to show CLNs in endoscopic thyroidectomy. CNP suspension was safe and we do not find any side effects in our series of >150 PTC.
Details of the operation are shown in Supplementary Video S1.
Footnotes
Acknowledgments
This research was funded by China Postdoctoral Science Foundation (no. 2017M611313) and Department of Science and Technology of Jilin Province (no. 20170520018JH and 20190201225JC).
Statement of Ethics
This study was approved by the research institute's committee on human research of China–Japan Union Hospital of Jilin University (Protocol no. 2015ks034), and the patients' written informed consent was obtained before study participation. Data were collected and stored in concordance with the Declaration of Helsinki. All data had no personal identifiers and were kept confidential.
Authors' Contributions
H.S. and G.D. were in charge of conception and design of the article, and H.S. gave the administrative support. H.S., G.D., and D.Z. were responsible for the collection and assembly of data, data analysis, and interpretation. All authors wrote and gave final approval of the article.
Disclosure Statement
No competing financial conflicts of interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.