
Abstract
Abstract
Objective
: This study aimed to evaluate the feasibility of the gasless transoral endoscopic thyroidectomy vestibular approach (TOETVA) using the Thyroidoscope, developed to maintain the surgical working space without CO2 insufflation.
Materials and Methods
: To prevent a potentially fatal CO2-related complication, we developed a retractable device, named the Thyroidoscope, which could maintain the surgical working space without CO2 insufflation. We conducted a preclinical cadaver study to evaluate its use in gasless TOETVA.
Results
: The Thyroidoscope provided a secure surgical field and stable image on the screen. We could successfully identify the recurrent laryngeal nerve, parathyroid gland, and other critical structures without inadvertent injury due to insertion of the Thyroidoscope.
Conclusions
: The Thyroidoscope provides sufficient working space to perform transoral thyroid surgery without the need for CO2 insufflation. Gasless TOETVA with the Thyroidoscope seems to be feasible and safe.
Introduction
The transoral endoscopic thyroidectomy vestibular approach (TOETVA) has recently grown in popularity due to its many advantages. These include the fact that it can be completed with only a mucosal incision, as a skin incision is unnecessary; the area of dissection is comparatively narrow; and the approach through a midline oral incision facilitates total thyroidectomy. However, during transoral thyroid surgery, an unnatural space is created in the anterior neck, and CO2 injected to maintain the working space may lead to gas-related complications, such as subcutaneous emphysema, pneumothorax, pneumomediastinum, and CO2 embolism. CO2 is inert, colorless, inexpensive, and readily available and dissolves in the blood; it is thus widely used during endoscopic surgeries. However, the complications of its use can include hypercapnia, metabolic acidosis, and cardiorespiratory compromise. In transoral thyroid surgery, subcutaneous emphysema usually improves spontaneously, while CO2 embolism during laparoscopic and endoscopic procedures is a rare but potentially fatal complication. 1 In the largest study of the transoral approach, Anuwong found that among the >600 evaluated patients, only 10 developed subcutaneous emphysema; none had severe gas-related complications (CO2 embolism, pneumothorax, or mediastinal emphysema). 2 However, Fu et al. reported that 2 of 81 patients developed intraoperative CO2 embolism, necessitating conversion to open thyroidectomy. 3 Kim et al. reported the development of CO2 embolism during flap elevation before transoral robotic thyroidectomy; the patient was instead operated on using a retroauricular approach. 4 Chen et al. reported that subcutaneous emphysema occurred in 31 (28.8%) of 80 patients, with 8.8% remaining in the post-anesthesia care unit for 2 hours, which was a longer duration than after other forms of surgery (2.2%). 5 Wilhelm and Metzig reported one case of mediastinal emphysema among eight patients (21%) who showed improvement after conservative treatment. 6
To address these limitations, we developed a retractable device, named the Thyroidoscope, which could maintain the surgical working space without CO2 insufflation. We conducted a preclinical cadaver study to evaluate its use in gasless TOETVA.
Materials and Methods
Human cadaver
A freshly frozen human cadaver was obtained from the Pusan Institute for Applied Anatomy, Pusan National University School of Medicine, Busan, Korea. This human cadaver had no previous neck surgery or thyroid disease. The institutional review board at the Pusan National University Hospital approved this study.
A prototype Thyroidoscope for gasless transoral endoscopic thyroid surgery
The thyroidoscope was designed by SG W., JO P., and SC S. and produced by SG W. It consists of a blade, handle, body, and two spreaders (Fig. 1A). The blade was designed to support the roof of the working space during surgery. A width of 12 mm was chosen for the blade to prevent inadvertent injury of the mental nerve. Two spreaders attached to the blade provided additional working space in the lower neck by unfolding them (Fig. 1B). The body of the Thyroidoscope was designed in conical shape to secure sufficient space between the mandible and the skin of the chin during surgery, which allows easy access and a sufficient range of endoscope motions. The handle is designed to be securely gripped by the operator during insertion and removal of the Thyroidoscope. The end of the handle can be connected to a common laryngoscope holder (Karl Storz GmbH, Tuttlingen, Germany) (Fig. 1C, D).
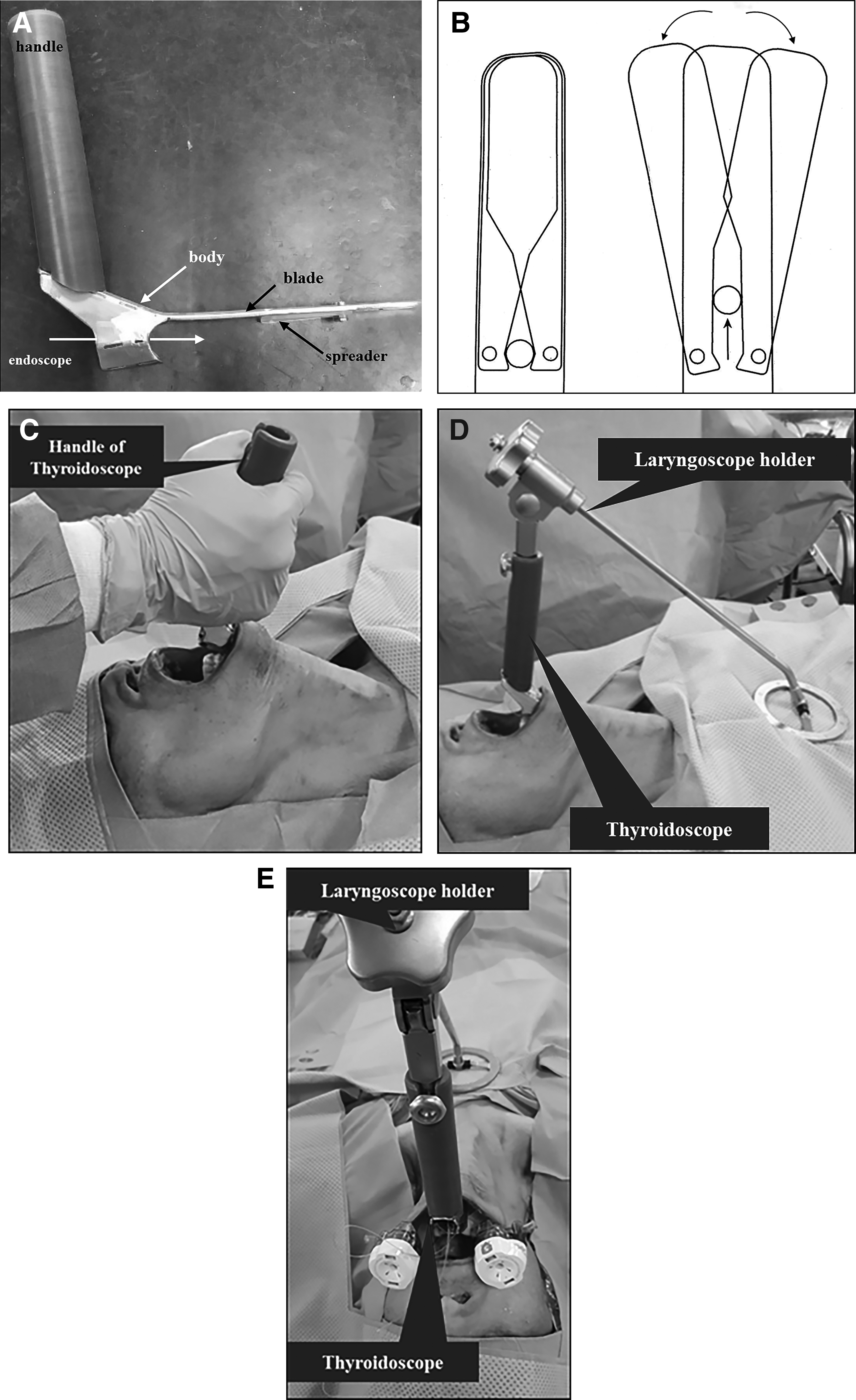
A prototype of our Thyroidoscope for gasless transoral endoscopic thyroid surgery.
Surgical procedure to secure the working space for transoral endoscopic thyroid surgery using the Thyroidoscope
The cadaver was placed in the supine position with the neck extended by a pillow placed under the back. The head of the cadaver was fixed using cotton plaster to prevent movement during the operation. Draping was done so as to expose the upper lip and suprasternal notch. The operator was positioned above the patient's head and the monitor was near the patient's leg. After a 2-cm curvilinear incision was made in the midline vestibule using monopolar electrocautery, 40–50 mL of normal saline was injected into the subplatysmal layer of the anterior neck to create a working space, which was then widened using blunt instruments (Kelly clamp and vascular tunneler). After the working space was dissected, the Thyroidoscope was inserted into the subplatysmal layer of the anterior cervical area. Then a 10-mm 30° endoscope was inserted through the Thyroidoscope, to determine whether the working space was appropriate and of sufficient size (Fig. 2A). Two small vertical incisions were made in the vestibule near the premolars bilaterally, and a 5-mm cannula was inserted through each lateral incision site. The endoscopic instruments were then positioned through each lateral cannula. The working space was widened sufficiently by unfolding two spreaders, extending from the sternal notch inferiorly to both sternocleidomastoid muscles laterally, using an L-hooked electrocautery and ultrasonic device (Fig. 2B). Transoral endoscopic thyroidectomy was then performed stepwise as described in our previous report. 7 At the completion of the surgery, the cadaver was explored and dissected through a traditional Kocher incision to confirm the preservation of important anatomical structures (mental nerve, submandibular gland, facial artery and vein, carotid artery and jugular vein, recurrent laryngeal nerve, parathyroid gland, tracheal and laryngeal structures, and the esophagus) and to identify any remnant thyroid tissue.

Securing the working space for transoral endoscopic thyroid surgery using the Thyroidoscope without CO2.
Results
Security of surgical field
The working space was secured sufficiently using the Thyroidoscope, extending from the sternal notch inferiorly to both sternocleidomastoid muscles laterally. During the entire surgical procedure, there was no collision between surgical instruments and the endoscope. Furthermore, there was no blind zone that could not be visualized through the endoscope, or dead zone where the surgical instruments could not reach. The laryngoscope holder to fix the Thyroidoscope provided a solid and convenient fixation. The additional two spreaders on the blade of the Thyroidoscope provided a wider view of surgical field in the lower neck.
Identification and preservation of critical structures
We could identify the recurrent laryngeal nerve and parathyroid gland successfully (Fig. 2D), and there was no injury of the trachea, esophagus, or major vessels during the entire surgical procedure (Fig. 2). The preservation of these structures was evaluated via a Kocher incision at the end of the surgery.
Inadvertent injury due to insertion of Thyroidoscope
There was no inadvertent injury to the teeth, corner of the mouth, mucosal incision site, or anterior neck skin due to insertion of the instrument.
Stability of the screen
The Thyroidoscope provided a stable image on the screen without fluctuation of the surrounding tissues and the roof of the working space due to pressure change related to CO2 insufflation and suction. The Thyroidoscope created an open cavity in the surgical space; thus, smoke generated by electrocautery or the energy device was easily emitted through the Thyroidoscope.
Discussion
Our newly developed retractable device, Thyroidoscope, allows transoral thyroid surgery without CO2 insufflation. CO2 is widely used in laparoscopic abdominal surgery, but gas-related complications, such as subcutaneous emphysema, pneumothorax, pneumomediastinum, and potentially fatal CO2 embolism, while rare, may develop.1,3,4 During TOETVA, the initial CO2 pressure is typically set to 5–6 mmHg at the beginning of surgery and lowered to 3–4 mmHg during the procedure. Close cooperation from an anesthesiologist and continuous monitoring of end-tidal CO2, which should not exceed 40–45 mmHg, are essential during transoral thyroid surgery using CO2. Nonetheless, the surgeon must pay great attention to prevent complications associated with CO2 use. Our Thyroidoscope is similar to a laryngoscope and can be fixed to the laryngoscope holder without any further adaptors. The initial design of the Thyroidoscope was simply a handle and right-angled blade, but vertical motion was limited due to the narrow inner diameter of the scope. To secure a sufficient range of motions, the body of the Thyroidoscope was redesigned in conical shape, which allows easy access and a sufficient range of endoscope motions. Also, two spreaders were attached to provide an additional working space in the lower neck. Of note, there was neither a blind zone—an area that cannot be visualized, nor a dead zone—an area where the instrument cannot reach to.
When CO2 is continuously injected into a narrow working space, as the pressure changes, the surrounding tissues and the roof of the working space are repeatedly moved as if they are pulsating. This may be dangerous during surgeries involving major structures, such as the recurrent laryngeal nerve or vessels. However, there was no such pulsating movement during gasless TOETVA, resulting in an improved surgical technique. In addition, since the working space in TOETVA is a closed cavity, frequent suction and removal of smoke generated from the energy device will typically result in a collapse of the working space, due to the high negative pressure and the adherence of blood to the endoscope, thus blurring the surgical field. However, in gasless TOETVA, the working space is an open cavity that remains open even if smoke is drawn by a continuous application of negative pressure.
Nonetheless, gasless TOETVA also has a few minor drawbacks. Because the blade of the retractor is located on the roof of the working space, the height of that space is slightly lower, and the blade may interfere with the endoscopic view of the retrothyroidal area. We evaluated the continuity of the mental nerve after surgery. However, as this was a preclinical cadaver study, we could not confirm if any functional deficit due to compression or traction injury occurred.
In conclusion, our newly developed Thyroidoscope provides sufficient working space to perform transoral thyroid surgery without the need for CO2 insufflation. Gasless TOETVA with the thyroidoscope seems to be feasible and safe. However, its drawbacks must be overcome before it can be used in patients.
Footnotes
Acknowledgments
This work was supported by a National Research Foundation of Korea grant funded by the Korean government (NRF-2014R1A2A2A03004802) and a clinical research grant from the Pusan National University Hospital in 2017.
Disclosure Statement
No competing financial interests exist.