
Abstract
Abstract
Background:
Advances in choledochoscopy technology lead to an improvement in the treatment of hepatolithiasis. The aim of this study is to analyze the complications and efficacy of percutaneous postoperative choledochoscopy (PPOC) for residual stones.
Materials and Methods:
Retrospective analysis of patients who underwent PPOC for residual stones. Main outcome measures included the rate of stone removal and postoperative complications.
Results:
Eight hundred twenty-six patients received PPOC. The average duration of choledochoscopy was 30 min (range, 14–42 min). Complications included basket incarceration, T-tube dislodgement, bleeding, bile leaks, and infection. Residual stone clearance rate was achieved in 97% of the cases.
Conclusions:
PPOC is a safe and effective approach for residual stones.
Introduction
Amultidisciplinary approach has been applied effectively to treat gallstone disease, including endoscopic retrograde cholangiopancreatography, laparoscopy choledochotomy, and open choledochotomy. Choledochoscopy was a valuable method in the treatment of intrahepatic duct stones.1,2 Biliary surgeons make an effort to clear the bile ducts of stones in the operation; retained stones still occur. Thus, choledochoscopy played a very important role in residual stones. In our country, percutaneous postoperative choledochoscopy (PPOC) through the T-tube tract is widely used.
Choledochoscopy was started to be used in our department in 1990s. Methods of choledochoscopy in removing biliary stone include duct irrigation, lithotripsy, and stone retrieval using baskets. The aim of this article is to evaluate the results of 826 PPOC procedures performed in a 20-year period between July 1998 and July 2018, which highlights our experience with PPOC and analyzes the complications.
Materials and Methods
From January 1998 to June 2018, a consecutive series of 1000 patients (with intrahepatic and extrahepatic bile duct stones) underwent laparoscopy or conventional exploration of the common bile duct (CBD). All patients were evaluated by a combination of diagnostic imaging examinations, including ultrasonography, computed tomography (CT), magnetic resonance cholangiopancreatography, and cholangiograms. Among them, 826 patients had residual stones after operation, with diameters ranging from 0.4 to 3 cm. There were 456 women (mean age 49 years, range: 31–78) and 370 men (mean age 46 years, range: 32–84). One hundred eighty patients had undergone laparoscopy common bile duct exploration (LCBDE), and the rest had laparotomy. The interval time between the initial operation and the last PPOC is 4–42 weeks. The average time is 5 weeks. In this study, 826 cases were treated at 2264 times.
Olympus overlay transport virtualization-state estimation fiber optic choledochoscope and a supporting video monitoring system were used. The diameter of the choledochoscope was 4 mm. For large stones, electrohydraulic lithotripsy and holmium laser lithotripsy were performed.
Statistical analysis was performed using SPSS 20.0 software. Chi-square test was used for comparing categorical variables. Quantitative data were expressed as mean ± standard deviation, and comparisons of data were performed with the Student's t-test. Variables were considered significant with P < .05.
Operative procedure
Standard laparoscopy and conventional exploration of CBD were performed initially. All cases were evaluated with routine blood screening, blood grouping, liver function, coagulation functions, and other laboratory investigations before operation. In operation period, an incision was made in the anterior of the CBD for exploration. Subsequently, a choledochoscope was put into the CBD to examine and remove stones. Lithotripsy was performed for large stone. Partial hepatectomy was performed depending on the extent of intrahepatic biliary stricture and liver atrophy. All the patients were placed on T-tube larger than 20 gauges.
T-tube cholangiography and CT scan were performed on day 14 after surgery, to determine the presence of residual stones and their locations. PPOC was performed in the patients with residual stones at least 6 weeks after surgery.
PPOC was performed with continuous saline irrigation with a pressure of 80 mmHg. After withdrawing the T-tube, choledochoscope was inserted through the sinus tract to the CBD and was performed up to the branches of the intrahepatic bile ducts. They visualized the papilla of Vater by deflecting the scope distally. Whenever small stone was observed (diameter <5 mm), by applying saline irrigation with high pressure, 3 the small stones were flushed out of the CBD and through T-tube sinus tract. Bigger stones (5–10 mm) required extraction with the stone basket. Electrohydraulic lithotripsy was performed for larger stone (15 mm). Finally, the function of the sphincter of Oddi was checked by observation of symptoms and signs to determine whether there was any complication. The T-tube was reinstated after operation and was removed from patients with complete stone clearance. Reinstated T-tube could maintain the fistula in case further treatment was necessary. If residual stone was found, choledochoscopy and extraction were repeated one week later.
Results
In this series, mortality was not seen due to the PPOC procedures. One thousand patients underwent surgery with T-tube. Of the patients, 826 patients have residual calculi and received PPOC after operation. The anatomical distribution of residual stones is listed in Table 1 and Fig. 1. It also can be acquired from CT scan (Figs. 2–7). One to 12 times (average 2.9) was required to extract the residual calculus. The success rate of residual stone clearance was 97%.
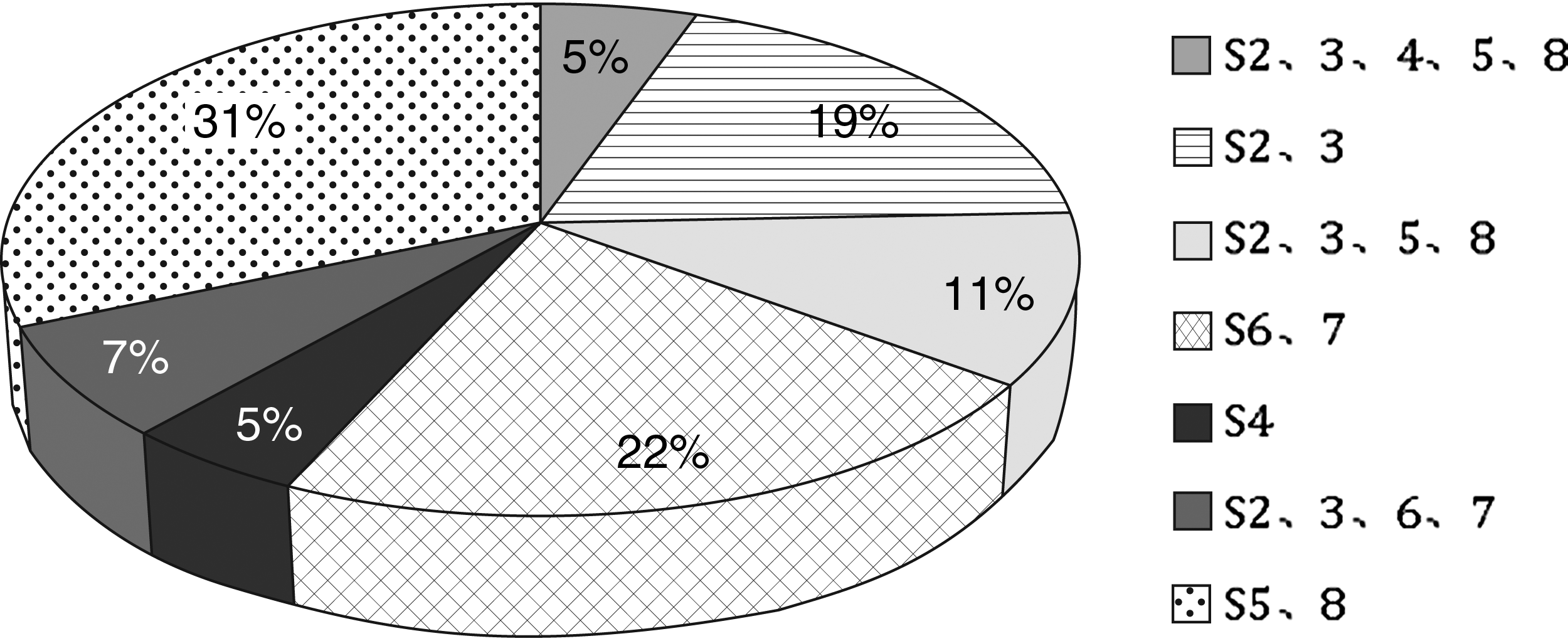
Distribution of residual stone.
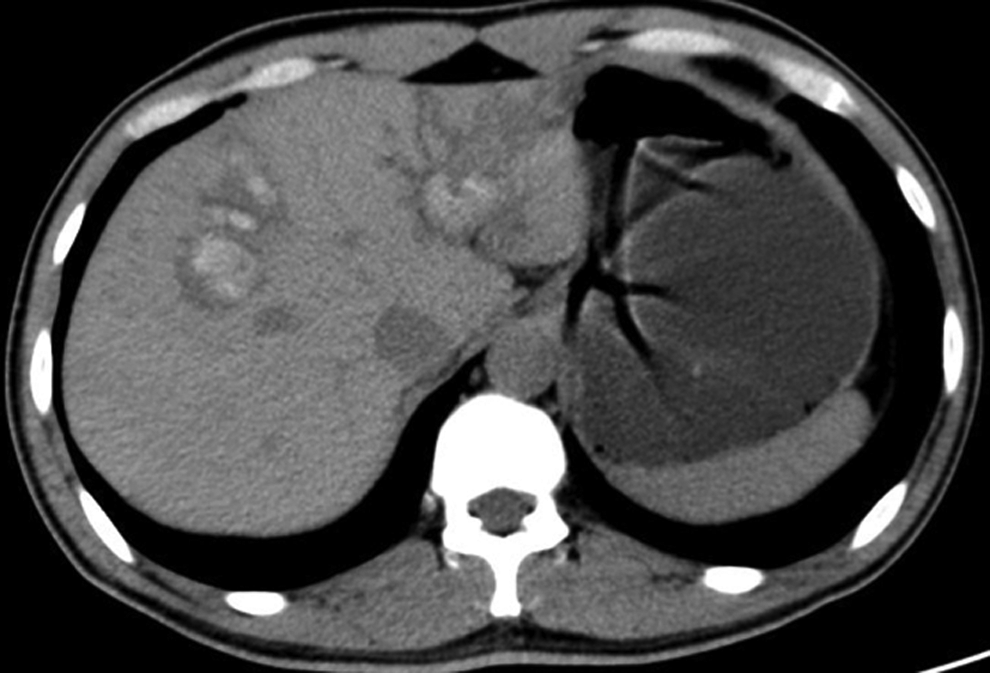
Residual multiple stones in S2.3.5.8.
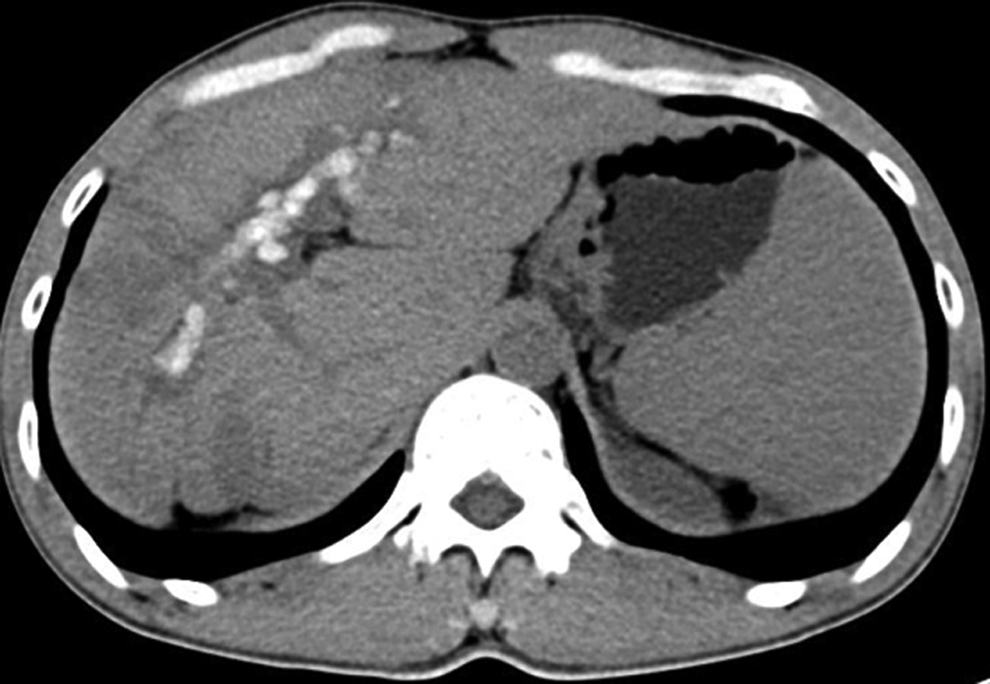
Residual multiple stones in S2.3.4.5.8.
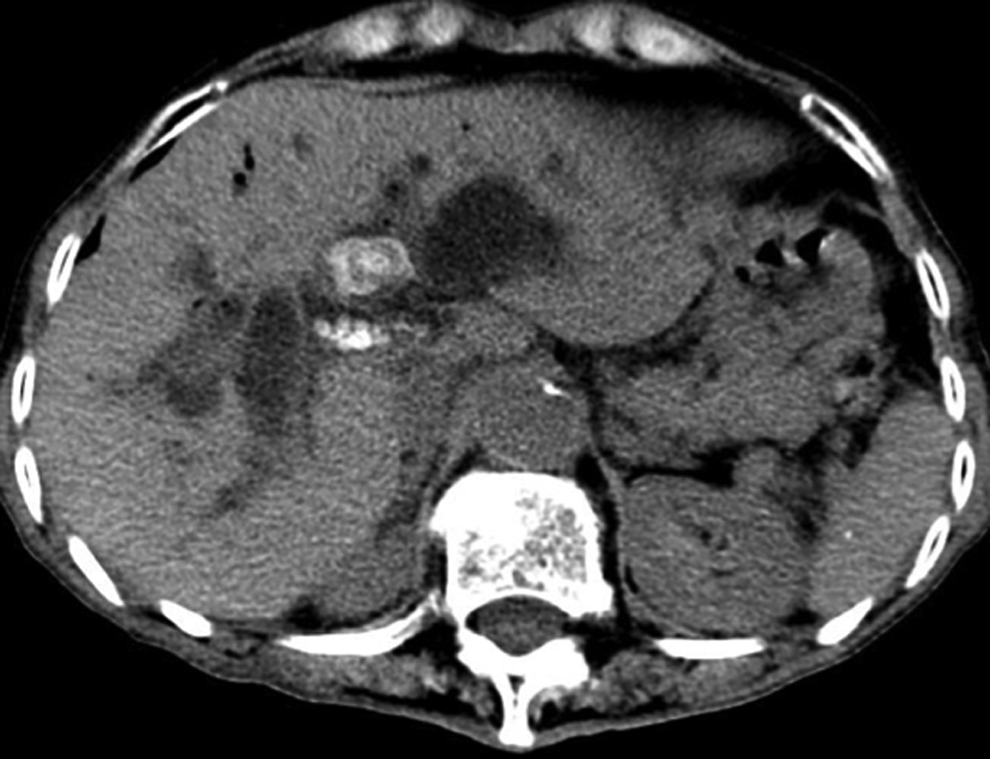
Residual multiple stones in S4.

Residual multiple stones in S8.

Residual multiple stones in S2.3.6.

Residual multiple stones in S6.
Distribution of Residual Stone and Stone Clearance Rate
Severe acute pancreatitis and acute cholangitis were not observed (Table 2). Twelve cases were unsuccessful because of the basket incarceration or the T-tube accidentally dislodged. Sixteen patients had biliary hemorrhage in choledochoscopy as a result of stone friction of the inner wall of bile duct, 10 patients had delayed biliary hemorrhage, one of the intraoperative biliary hemorrhage required surgical intervention at last, and the rest of the patients were cured after conservative treatment. Three cases of bile leakage happened when putting out the T-tube because of fistula hypoplasia. These cases were treated successfully; one patient received surgical drainage and the other conservatively with a drainage tube. There were 30 cases which had biliary tract infection and sepsis after PPOC, 5 patients were severe; fortunately, all the patients recovered by anti-infective treatment. They were managed conservatively and did not develop acute cholangitis.
Complication of Postoperative Choledochoscopy
A total of 133 patients underwent lithotripsy in PPOC (Table 3). They were divided into group A (Fluid-electric lithotripsy) and group B (holmium laser lithotripsy) according to the different methods of lithotripsy. There were no significant differences between clinical characteristics and regarding demographics between the two groups. The mean operation time was 32 ± 8 min for group A and 30 ± 6.6 min for group B (P = .12). Stone clearance rates were not significantly different between the two groups (97.11% for group A versus 95.32% for group B, P = .42). Postoperative bleeding occurred in 9 patients (13%) of group A and 4 patients (6.25%) of group B.
Comparison of Effect and Complication of Patients Treated by Different Lithotripsy
P values are for comparison of group A and group B.
P value < .05 was considered statistically significant.
Group A, electrohydraulic lithotripsy; Group B, holmium laser lithotripsy; SD, standard deviation.
Discussion
Hepatolithiasis is a common disease in East Asia and is prevalent in China. Endoscopic treatment is assumed to be the first alternative treatment for the stone in the CBD, 4 but was not applicable for the intrahepatic duct stone. Meanwhile, it can cause the damage of duodenal papilla and lead to postoperative biliary reflux, cholangitis. In contrast, the application of hepatectomy has been limited because of a highly invasive procedure, which may induce postoperative complications. In China, there are a large number of patients with intrahepatic bile duct stones, too many intrahepatic bile duct stones to be completely removed in one operation. Comparatively speaking, CBD exploration or LCBDE with T-tube approach has been still widely applied to establish channels for percutaneous postoperative choledochoscopic treatment.
Residual stone was a problem in the treatment of intrahepatic duct stones. Despite remarkable improvements in the treatment of intraoperative lithotomy, which can improve the stone-free rate for patients undergoing surgery combined with choledochoscopy during the operation, 5 the incidence of post-operative residual stones is still high.6,7 It may be impossible to attain clearance of stones in one session. So, PPOC is very important for these patients, especially for the complicated stone.
Successful removal of stones depends on skilled techniques and careful monitoring. The reported success rate for residual stone removal from the intrahepatic duct ranges from 60% to 90%.8,9 In our study, there were altogether 826 cases that had residual stones after biliary tract exploration; the residual stone rate was 61.19%. And then, PPOC through T-tube sinus was performed; in 802 out of 826 cases the stone was taken out cleanly; and the success rate was 97%. Normal saline is used to insufflate the biliary system, and choledochoscope was first inserted to observe the integrity of sinus tract and the angle of sinus and CBD. Then, the basket through the duodenal papilla is opened and pulled back to detect the function of sphincter. For intrahepatic duct stone, the basket is maneuvered over the stone, opened behind it, trapped, and the stone is pulled out. For incarcerated stone, lithotripsy is used to release it and then it is maneuvered out using the basket technique. The lithotripsy also is applicable in cases where the stone is too large. It is important that each session (choledochoscopy) is limited to less than 3 L physiological saline, because prolonged perfusion of the bile duct results in the increase of biliary pressure associated with infection.
Sepsis or biliary tract infection after PPOC is a common phenomenon. During PPOC, normal saline is used to insufflate the biliary system, helps to dilate the bile ducts, and improves visualization by clearing mucus, pus, and stone debris. 10 Continuous saline irrigation can potentially increase intrabiliary pressure 11 and may therefore increase the risk of cholangitis. Sepsis after PPOC can be prevented in two ways. First, the pressure of physiological saline flushing should not be too high, which may increase the chance of biliary tract infection, finally leading to sepsis. Second, older patients cannot tolerate PPOC for as long as younger patients; too long operation time is not suitable for these patients.
Hemobilia is a complication caused by the repeated stimulate (friction of basket or detritus) of the inside wall of inflammatory bile duct. The gentle movement during stone removal can avoid friction to the biliary tract as much as possible.
Lithotripsy is safe and effective in the treatment of residual stone. Lithotripsy, such as electrohydraulic and holmium laser lithotripsy, is often needed for complex biliary calculi. Although electrohydraulic lithotripsy and holmium laser lithotripsy work differently, they have the same advantage for the biliary stones because the depth of penetration of human tissue is very shallow. They are used for the calculus that is unable to be managed with standard techniques, including mechanical lithotripsy. 12 Previous studies suggest that stone size and stone impaction are the key predictors for failure of lithotripsy. 13 In this study, we reviewed 133 patients who had lithotripsy using choledochoscopy. Stone clearance was attained in 92% patients, with 70% obtaining complete clearance directly after electrohydraulic lithotripsy therapy. Complication from lithotripsy was acceptable. This suggested that electrohydraulic lithotripsy and holmium laser lithotripsy are safe and effective methods for treatment of the residual stones after operation.
Many centers have their own reports on the effects of different lithotripsy methods. Some people believe that electrohydraulic lithotripsy is often performed under direct choledochoscopic guidance to avoid errant application of shock waves that can cause trauma and perforation. 14 There is still a relative paucity of data on the comparison of the effects of electrohydraulic and holmium laser lithotripsy. In this study, electrohydraulic lithotripsy has been compared to holmium laser lithotripsy in 133 patients. They were divided into two groups. We found that there is no significant difference in the incidence of bleeding and final residual stones. The results demonstrate that electrohydraulic lithotripsy and holmium laser lithotripsy have equal safety and effectiveness.
Conclusions
The results of this study show that PPOC is necessary for residual stone removal, with low morbidity and, to date, no mortality. Therefore, PPOC is an effective and safe alternative to nephrolithiasis.
Footnotes
Acknowledgment
This work was undertaken in partial fulfillment for Guangdong Provincial People's Hospital.
Disclosure Statement
No competing financial interests exist.