
Abstract
Abstract
Background:
Laparoscopic repair has become the preferred option for the treatment of pediatric hernias. Recently, laparoscopic operations have also been conducted in pediatric recurrent hernia cases. Laparoscopic percutaneous extraperitoneal closure (LPEC) is a simple and reliable minimally invasive procedure for pediatric inguinal hernia repair. However, it is still unclear whether LPEC is an ideal procedure for recurrent inguinal hernias in children. The aim of this study is to evaluate the efficacy of LPEC in the treatment of pediatric recurrent inguinal hernias.
Patients and Methods:
We retrospectively reviewed all children with primary inguinal hernia repairs in our hospital from 2016 to 2017 and analyzed the outcomes of recurrent inguinal hernia repairs with LPEC.
Results:
There were 1703 children with 1985 indirect inguinal hernias: 1549 were laparoscopic (91.0%) and 154 open (9.0%). Thirty-five (2.1%) of these children had recurrent inguinal hernia with no difference in prevalence between laparoscopic and open (P = .24). One case was bilateral. LPEC was performed successfully in all children with recurrent inguinal hernias. There were no severe intra- or postoperative complications in any of the recurrent cases. No children had inguinal hernia recurrence at follow-up (8 months–2 years).
Conclusions:
LPEC of the internal ring is a reliable and effective minimally invasive technique for the treatment of recurrent inguinal hernia in children.
Introduction
Pediatric inguinal hernia is one of the most common conditions that require surgical intervention. Inguinal hernia recurrence is not a frequent postoperative complication but a major indication for reoperation in children. 1 Conventional open repair of recurrent childhood inguinal hernias can still be challenging for pediatric surgeons since it is performed in the same procedure field as the previous open repair. 1 Furthermore, the open approach has a definite risk of damaging the vas deferens and testicular vessels in male children.2–4 Recently the laparoscopic approach is becoming a preferred option for pediatric recurrent inguinal hernia repair due to the benefits of avoiding the difficulties of redo open surgery and reducing the risks associated with the open approach.5–10
Laparoscopic percutaneous extraperitoneal closure (LPEC) was first reported by Takehara et al. in 2006. 11 It is a simple extraperitoneal approach to treat inguinal hernias in children, where internal inguinal ring closure is performed percutaneously using nonabsorbable suture material. 11 Currently, LPEC has become one of the most simple and reliable minimally invasive procedures for primary inguinal hernia repairs in children, including extremely low birth weight infants.12–17 However, the efficacy of LPEC in pediatric recurrent cases remains unclear.
The aim of this study was to evaluate the efficacy of LPEC in children with recurrent inguinal hernias at a national children's medical center in China.
Patients and Methods
Patient population
The Children's Hospital of Fudan University Institutional Review Board approval was obtained before initiation of this study. A single institution retrospective review was performed on all children who underwent open or laparoscopic primary hernia repair, in the department of pediatric surgery, Children's Hospital of Fudan University, between January 2016 and January 2017. The following details were reviewed, including demographics, the type of the primary hernia repair (open or laparoscopic), and date of recurrence. Among all recurrent cases, details of reoperation, postoperative course, and long-term outcome were collected.
Operative procedure
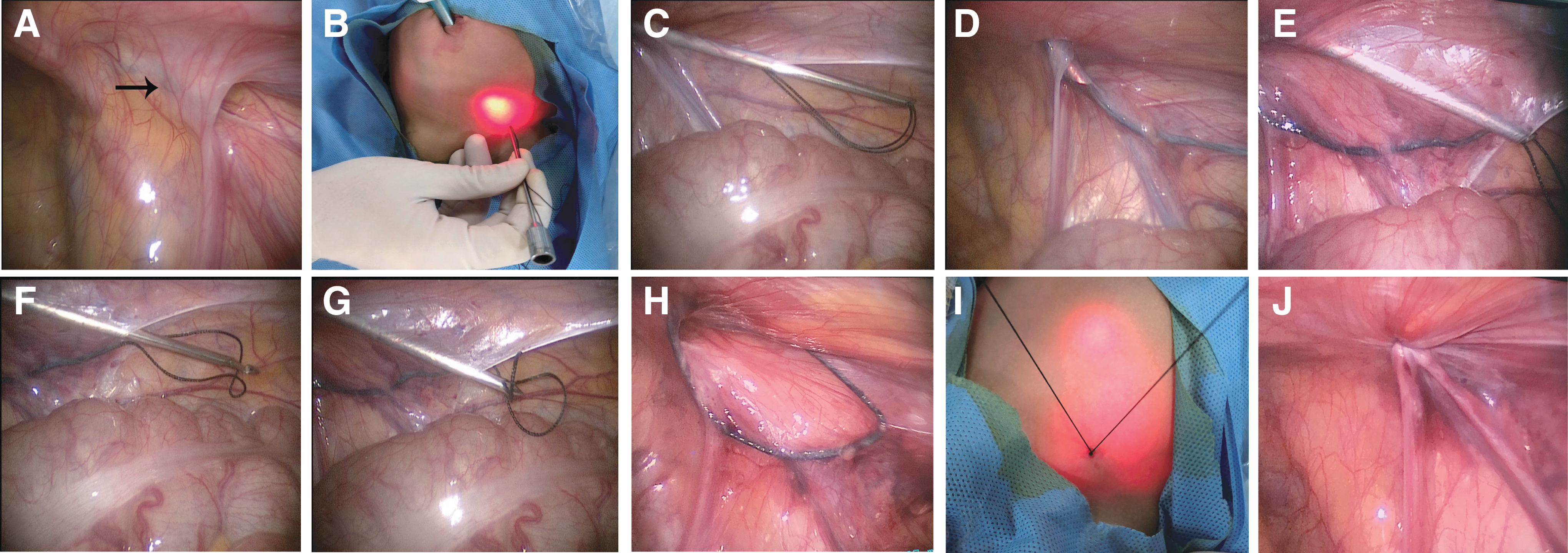
A modified single-port LPEC with a single-hooked hernia device (Fig. 1A), based on the technique previously described by Li et al., 18 was performed in all recurrent inguinal hernia cases. In brief, the patient was administered general endotracheal tube anesthesia in the supine position. One 5 mm trocar was inserted through the umbilicus. Through this trocar, a 30° laparoscope was placed and a pneumoperitoneum was maintained at 8–10 mmHg with a CO2 flow rate of 1–2 L/min. Bilateral internal inguinal rings were checked carefully (Fig. 2A). A stainless steel sheath with a 2–0 silk suture loop placed retrogradely (Fig. 1B) was inserted through the corresponding skin of the internal ring into the extraperitoneal space (Fig. 2B).
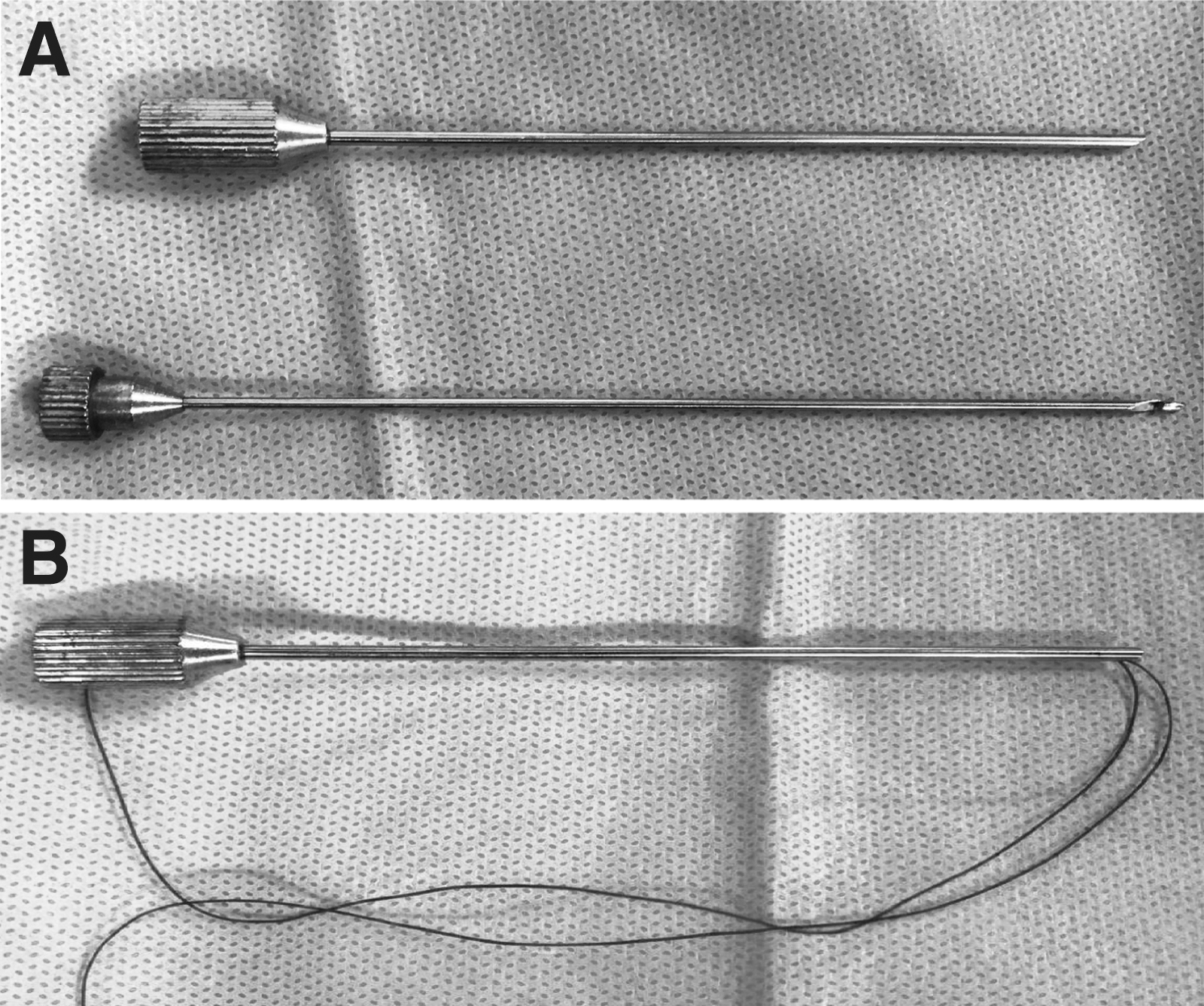
The single-hook hernia repair device:
Modified single-port laparoscopic percutaneous extraperitoneal closure procedures:
The device was further advanced along the medial side of the ring and passed into the peritoneal cavity lateral to the spermatic vessels (Fig. 2C). The sheath was then detached from the suture loop and withdrawn to the initial extraperitoneal site with the assistance of the laparoscope (Fig. 2D). The sheath was then advanced along the internal ring laterally and reintroduced into the abdominal cavity through the previous peritoneal puncture point (Fig. 2E). The core with the single hook passed into the suture loop through the sheath and locked the suture end inside the sheath (Fig. 2F, G). Finally, the single-hooked hernia device with the suture was pulled out through the abdominal wall and the internal inguinal ring closed by knotting the suture extracorporeally (Fig. 2H–J).
Statistical analysis
Continuous data were expressed as mean ± standard deviation. Qualitative data were presented as percentages and compared with the Fisher's exact test. Statistical analysis was performed using SPSS® version 20.0 statistical software (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.). A P-value of <.05 was considered statistically significant.
Results
Patient demographics
A total of 1703 children with 1985 indirect inguinal hernias in the department of pediatric surgery, Children's Hospital of Fudan University, during January 2016–January 2017 were included. Patient demographics and clinical characteristics are given in Table 1. The mean age at primary surgery was 17.2 ± 11.9 months (range, 5 months–9 years). The primary inguinal hernia repair procedure was LPEC (n = 1549, 91.0%) or open (n = 154, 9.0%). 35 (2.1%) of these children developed recurrence, where 1 patient had bilateral recurrent hernia: 30 (1.9%) after initial laparoscopy and 5 (3.2%) after initial open repair (P = .24). All of the recurrent cases are male children with a mean age of 19.1 ± 8.3 months (range, 8–40 months). The mean recurrence period was 9.0 ± 4.2 months (range, 3–19 months).
Demographics and Clinical Characteristics of Children with Primary Hernia Repair and Recurrent Patients
IH, inguinal hernia.
Reasons for recurrence after primary inguinal hernia repair
Thirty-five recurrent cases were identified and a review of their medical records, operative notes, and operative videos for both the original operation and the reoperation was conducted to pinpoint the potential cause of recurrence. Causes of hernia recurrence are given in Table 2. The most frequent cause was failure to completely ligate the hernia sac (n = 11, 31.4%), and unexpected release of the suture closing the sac or internal ring (n = 8, 22.9%) during open or laparoscopic hernia repair. Additional 14 recurrences occurred after laparoscopic procedure due to the use of absorbable sutures (n = 8, 22.9%) and repair under tension (n = 6, 17.1%), respectively. Lower ligation of hernia sac (n = 1, 2.9%) and missed hernia sac (n = 1, 2.9%) also contributed to recurrences after open hernia repair.
Causes of Recurrence After Primary Inguinal Hernia Repair
Outcomes of laparoscopic reoperation and long-term follow-up
Single-port LPEC was successfully conducted in all recurrent cases without conversion (Table 3). The mean operative time for unilateral repairs was 16.5 ± 1.2 minutes (range, 15–20 minutes). The operative time for the bilateral surgery was 27 minutes. Postoperative hydrocele occurred in 2 patients (5.7%) and they were resolved spontaneously during follow-up. No other complications were identified in any of the postoperative cases during the hospital stay or early follow-up period.
Outcomes of Laparoscopic Reoperation and Long-Term Follow-Up
LPEC, laparoscopic percutaneous extraperitoneal closure; SD, standard deviation.
All of the reoperative cases were followed up until August 2018. The mean duration of follow-up was 17.5 ± 4.3 months (range, 8 months–2 years). A knots response at the inguinal surgical site was identified in 1 (2.9%) case that was treated by removal of the stitch in the outpatient department. No hernial re-recurrence or testicular atrophy occurred in any of the reoperative cases as per their latest follow-ups in the outpatient department of our hospital.
Discussion
Pediatric inguinal hernia recurrence is still a significant issue that requires general anesthesia and redo surgery. Hernia recurrence results from multiple factors, including various special conditions (prematurity, incarceration, overweight, cough, constipation, and connective tissue disorders), anatomic factors (large hernia sac and wide inner orifice), and technical issues (advertent release of a ligature closing the sac or internal ring, failure to completely ligate a large hernia sac, and multiple ruptures of the sac during surgical dissection).1,19–21
In our series, several technical issues contributed to hernia recurrences. Failure to completely ligate the hernia sac and unexpected release of the suture closing the sac or internal ring, which contributed to >50% of recurrences in children with both open and laparoscopic hernia, are frequent causes in our teaching hospital. Other issues such as use of absorbable sutures, repair under tension, lower ligation of hernia sac, and missed hernia sac caused recurrence in the rest of cases.
Furthermore, multiple studies have indicated that the surgical repair approach (open or laparoscopic) is not a real risk factor for hernia recurrence.1,22–24 In this study, there was no significant difference in recurrence rate between children with open and laparoscopic repair, which was similar to what is reported in the literature.1,22–24 This highlights the efficacy and safety of laparoscopic operation for primary pediatric hernia repairs. It further implies the potential benefit of laparoscopic recurrent hernia repairs.
Laparoscopic primary inguinal hernia repair can be performed through intraperitoneal or extraperitoneal approach. 25 Furthermore, extraperitoneal closure has been increasingly used due to its technical simplicity and effective results. 25 Recently, multiple studies have reported successful applications of intraperitoneally laparoscopic repair in pediatric recurrent hernias.5–10 However, the extraperitoneal approach to treat recurrent inguinal hernia in children remains poorly understood.
LPEC procedure is currently the most reliable and commonly used extraperitoneal approach for primary inguinal hernia repair. Besides general benefits of the laparoscopic extraperitoneal hernia repair, LPEC has additional advantages, including the following: (1) Dissection is limited to the internal ring area around, which significantly reduces the risk of vas deferens and testicular vessel damage, and (2) it can be performed even when adhesion around the sac or internal ring exists, which usually exists in recurrent cases. 16
In this study, single-port LPEC procedure was also successfully conducted in all recurrent cases without conversion. In addition, no severe postoperative complications, including re-recurrence or testicular atrophy, took place. Therefore, LPEC is likely a safe and reliable laparoscopic treatment for pediatric recurrent inguinal hernias.
To our knowledge, this is the first report of LPEC procedure being applied in pediatric patients with recurrent inguinal hernia repairs. However, this study is still limited by the small population size and short follow-up period. Results of this study would need to be correlated with further analysis based on more pediatric recurrent hernia cases. Our findings provide preliminary data and adequate justification to further evaluate our laparoscopic technique for children with recurrent inguinal hernias.
In conclusion, the laparoscopic procedure does not increase the risk of hernia recurrences in pediatric patients. LPEC of the internal ring is a simple and effective minimally invasive technique for the treatment of recurrent inguinal hernias in children.
Footnotes
Acknowledgments
This study was supported by Shanghai Hospital Development Center (SHDC, 12014106) and Shanghai Key Disciplines (No. 2017ZZ02022). We appreciate the comments from Dr. Agostino Pierro (The Hospital for Sick Children, Toronto, ON, Canada).
Disclosure Statement
No competing financial interests exist.