
Abstract
Abstract
Introduction:
Laparoscopic rectopexy for recurrent rectal prolapse (RP) is more widely used nowadays. Strict indications are needed to get proper outcomes. The advantages rely on the careful dissection of peritoneal sac and fixation of rectum. One of the theories of recurrent RP is hernia-like physiology in front of the rectum.
Purpose:
The aim of this study is to present our experience of posterolateral laparoscopic suture rectopexy (LSR) in indicated children of recurrent RP.
Patients and Methods:
Sixteen patients were included with recurrent RP wherein all were subjected to LSR procedure after exclusion of other probable causes. Dissection of peritoneal sac anterior to the rectum was carried out followed by closure of the deep pouch by nonabsorbable sutures then fixation of the right side of rectum and sigmoid to the lateral wall of areolar tissue. Fixation to sacral promontory is done by Ethibond or Prolene sutures when redundancy is obvious.
Results:
The study included 11 girls and 5 boys with age ranging between 3 and 12 years in the past 5 years. Ten cases were treated earlier with injection therapy and 6 following Thiersh procedure after failure of conservative treatment for 6 months. Operative time ranged between 40 and 100 minutes. Follow-up period ranged between 6 and 36 months with mean of 19.5 months. Postoperative mucosal prolapse reported in 1 case 6 months postsurgery with no full thickness recurrence.
Conclusions:
LSR is an efficient technique in well-selected children of recurrent RP and could reverse this underlying pathology. Longer follow-up and evidence are needed to standardize the technique.
Introduction
Rectal prolapse (RP) in children is a self-limiting common condition in infancy and children. 1 Conservative management is the standard line in many cases; however, intractable or recurrent cases may need surgical intervention when it became full-thickness protrusion.1,2 Pediatric RP occurs below the age of 4 years. 1 Nonresponding cases may require surgical intervention. 3 The incidence of complete RP is unknown in children, and there is considerable debate regarding its definite pathogenic mechanism. 4
RP may be graded as minimal wherein the rectal mucosa is visible only with Valsalva maneuver, moderate wherein the prolapse is <5 mm without Valsalva maneuver, and evident wherein the prolapse exceeds 5 mm without Valsalva maneuver. 5
Classic treatment of RP includes applying stool softeners and/or laxatives, bowel management, and avoidance of prolonged straining.1,3 The exact mechanism of prolapse as hernia in the retrovesical peritoneum or redundancy of colon or wide levator hiatus remains unclear as it may compromise fecal continence. This may have an impact on the patient's quality of life. 6
Yet, there is no standard surgical management for RP refractory to conservative medical management in the pediatric population. Injection sclerotherapy remains the popular and well-known minimally invasive procedure for initial management of RP in the pediatric population in many areas,7,8 whereas other minimally invasive procedures described in the literature such as the Thiersch anal encirclement, linear cauterization, and packing of the presacral space with various materials have been described. Transsacral rectopexy, transcoccygeal rectopexy, posterior sagittal anorectoplasty, and perineal proctosigmoidectomy (Altemeier procedure) represent some of the more invasive techniques used. 8
The determinant for the need of surgical correction after failed conservative management is based on the disturbance in the anatomy of the RP. Contrarily, the aim in mucosal prolapse is to create adhesions between the mucosa and the muscular layer of the rectum, for example, with sclerotherapy, a full-thickness RP requires a fixation of the rectum to the presacral fascia, thus fixing and elevating it. 9
The data about the optimal operative management for refractory RP are yet debatable, mainly supported by failure of the primary operative procedure. 8 This is reported mainly as recurrent cases after failure of injection sclerotherapy and linear cauterization was reported. 9
Since there are no criteria and principles to assign a specific surgical approach as the one of choice, they are broadly classified as perineal or abdominal depending on whether narrowing/strengthening the anal sphincter, suspending the rectum, excising the redundant rectum, or restoring the weakened pelvic floor.10,11 These include many operations proposed for treating RP, with varying recurrence rates and functional outcome.10–12 Currently, more laparoscopic techniques have been described including laparoscopic suture rectopexy (LSR) with optimal outcomes.2,10,13–15
Purpose
Our study aimed to present our experience of posterolateral LSR in indicated children of recurrent RP in children.
Patients and Methods
After getting approval of the Internal Review Board, a retrospective analysis was done for all patients <12 years old who had recurrent RP after failed primary surgical procedures during 5 years between January 2014 and December 2018 in Tanta University Hospital and other affiliated hospitals in Egypt.
This study included 16 patients and all were subjected to LSR procedure after exclusion of other probable causes. Preoperative preparation included colonic preparations. Prophylactic antibiotic was given at time of induction. Under general anesthesia with endotracheal tube in supine position for all patients, three ports were used: one 10-mm port for the camera at the umbilicus and two working 5-mm ports on both sides in midclavicular line below the level of the umbilicus. Traction suspension sutures were used to suspend the uterus to the anterior abdominal wall in girls as shown in Figure 1A and the urinary bladder in boys as shown in Figure 2A to help visualization of the pouch. Traction sutures through the abdominal wall were used some time for hanging the sigmoid. The surgeon stands near the patient's right shoulder with the camera to their left. The monitor is in line at the end of the table. Pneumoperitoneum started with the open technique and the patient was placed accordingly. The position of the working ports varies with the size of the child, ensuring triangulation and reasonable working space for the instruments. Trendelenburg position helps to gravitate the small bowel away from the operative field. At Trendelenburg position, the redundant rectum was retracted from the pelvis using an atraumatic grasper followed by exploration of the pelvis together with evaluation of the sigmoid length and rectosigmoid junctions in addition to pelvic floor hernia.
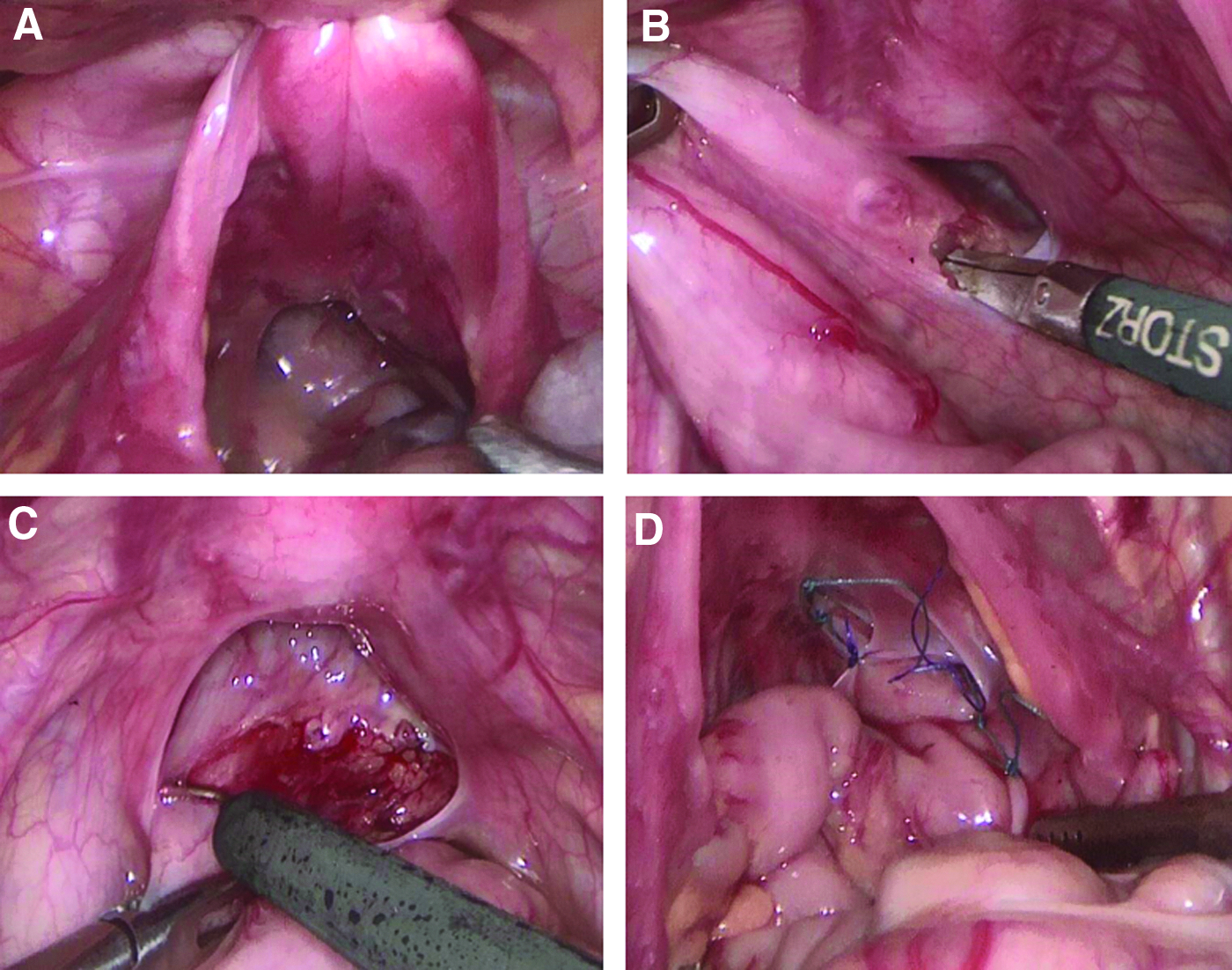
A panel of operative photographs wherein
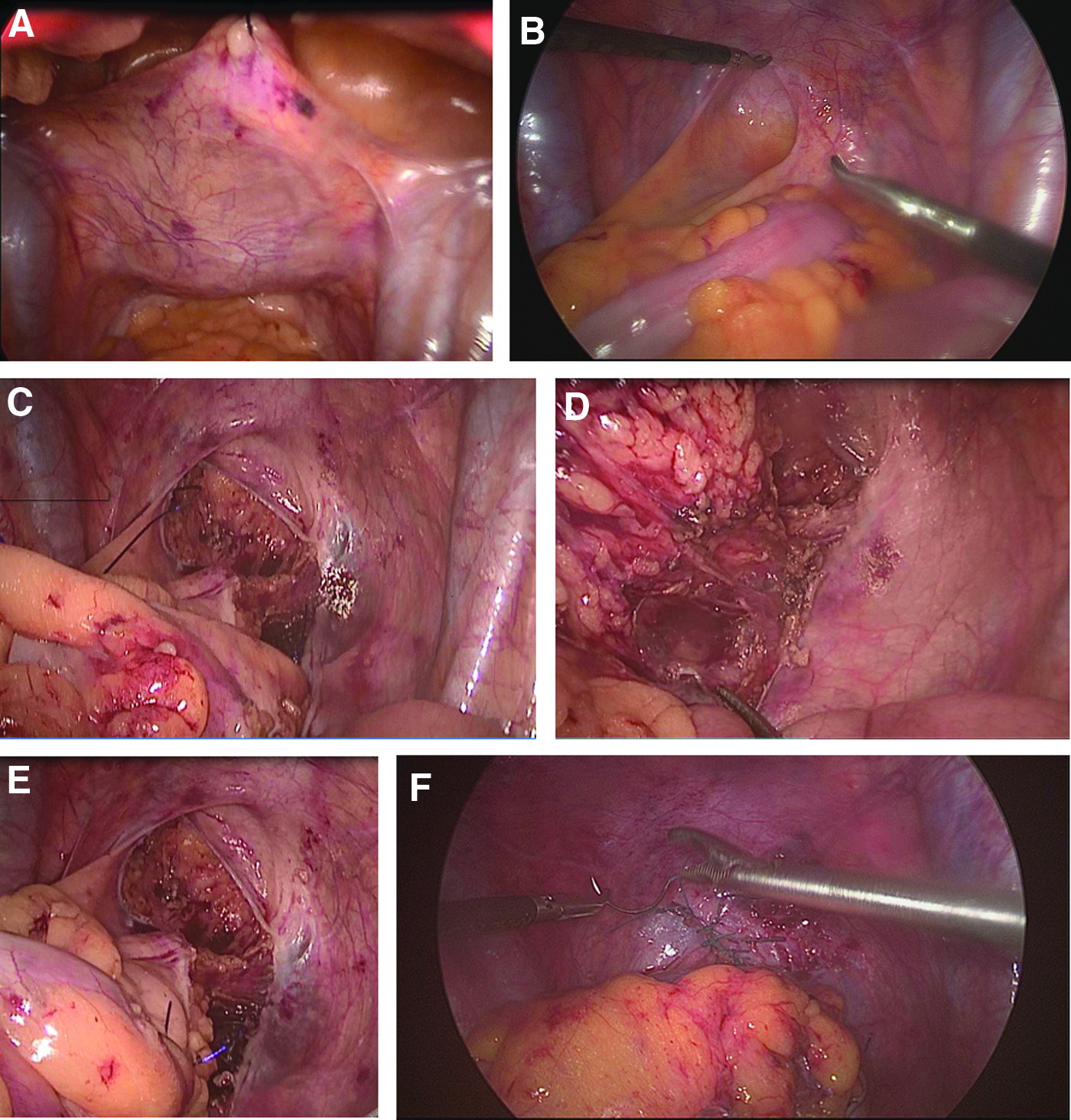
A panel of photographs wherein
Dissection usually started with the peritoneal sac anterior to the rectum as shown in Figures 1B, C and 2B, followed by the peritoneum on the lateral wall of the rectum on the right side with partial dissection of the mesorectum reaching the sacral promontory from above downward to the level of pelvic floor without division of the lateral ligament as shown in Figure 2C, D until the surface of the sacrum was clearly felt with an instrument. Fixation to sacral promontory was done using two Ethibond or Prolene sutures when redundancy is obvious followed by closure of the deep pouch by nonabsorbable sutures. Care should be taken to protect the ureters and vas deferens, in boys.
Plication suturing of the Douglas pouch peritoneum in girls and rectovesical pouch in boys is as shown in Figures 1D and 2E, respectively. The next step is fixation of the right side of the rectum and sigmoid to the lateral wall of areolar tissue in a posterolateral manner without rotation of the colon. Postoperatively, the patients were nothing per oral until peristalsis followed by soft diet for 4 days and were discharged on stool softeners and bowel management protocol. Follow-up was done regularly every month for at least 6 months, then annually.
Results
In the past 5 years, patients with failed primary surgery for RP were retrospectively evaluated. Sixteen patients showed recurrent complete RP and were managed with LSR after exclusion of other causes of recurrence. The study included 11 girls and 5 boys with age ranging between 3 and 12 years (mean 5.5 years). The primary surgical procedures were injection therapy in 10 cases and 6 following the Thiersh procedure with 9 cases showing both injection and Thiersh cerclage after failure of conservative treatment for at least 6 months. Operative time ranged between 40 and 100 minutes (mean 65.25 minutes).
Follow-up period ranged between 6 and 42 months with mean of 19.5 months. Only 1 case of postoperative mucosal prolapse was reported 6 months postsurgery. No full thickness recurrence was reported during the follow-up period. Other follow-up parameters such as constipation, incontinence, stool soiling, and discomfort were recorded, showing no complications.
Discussion
Chronic constipation stands as the common related cause for pediatric RP. Internal form of a hernia constitutes another hypothesis for precipitation for such a condition in children. Many surgical techniques and approaches have been described for this disease, denoting that the optimal procedure has not yet been established or does not apply to all cases.1,9,16
In the past two decades, different laparoscopic abdominal approaches such as suture or mesh rectopexy, resection rectopexy, levatorplasty rectopexy for RP repair have been described with different results. 16 Indeed, all literature reported lower recurrence rates than open techniques whether in children or adults. 17
The laparoscopic approach provides a golden solution to the problem of RP, which constitutes the standard form of transabdominal management of full-thickness RP.17,18 Advantages of laparoscopy include less pain, shorter hospital stay, and early recovery as compared with laparotomy.2,10 The current results of laparoscopic techniques are as good as open procedures if not better in long- and short-term results.18,19 These results were achieved irrespective of the method used (suture, resection, or posterior mesh), which added to the advantages of laparoscopy.19,20 Therefore, where expertise is available, this approach should be preferred. 17 (In our study, the mean age of cases was 5.5 years, which is similar to that reported by Gomes-Ferreira et al. 20 and higher but 2.6 years as reported by Antao et al. 1 )
The pediatric literature suggests equivocacy between mesh rectopexy and suture rectopexy, 11 but yet superior results were achieved after suture rectopexy in pediatric RP.19,20 Despite that only eight LSRs showed no recurrence after 36 months of follow-up in Ismail et al., 15 de Bruijn et al. reported excellent results of suture rectopexy recently after long-term follow-up in 90% of his cases of adult RP. 18 Among 40 patients in one series, there were no recurrences during an average follow-up of 36 months after 22 laparoscopic mesh rectopexies, 8 LSRs, and 10 laparoscopic resections of the redundant rectosigmoid. 15 Potter et al. with an average of 6 months follow-up reported just 1 recurrence of mucosal-type prolapse among 19 cases. 19
This is comparable with our results, but in our series it was applied for the recurrent cases after a failed primary surgical procedure not a primary procedure. Furthermore, despite that high complication rate of 61% has been reported after 25 LSRs, Koivusalo et al. reported just 1 case of full-thickness recurrence. 16 This may be because of improper selection of cases in his series including cases with neurogenic pathology as compared with our results of no recurrence. This advocates for proper selection of cases for LSR to get the best results.
Gomes-Ferreira et al. reported reduced recurrence rates following mesh rectopexy (13 procedures) versus LSR (5 procedures) in the context of redo surgery.20,21 This is comparable to laparoscopic mesh rectopexy and to our results. Gomes-Ferriera et al. also reported lower recurrence rates with mesh rectopexy; however, the cases were mostly geriatric and included the learning curve. 21 Contrary to that, de Bruijn et al. reported excellent long-term results of suture rectopexy in 90% of their cases. 18 Similar to other series, we demonstrate no recurrences in our patients undergoing LSR.18,22,23 Awad et al. and Ismail et al. have similar results, as well.2,15
We reported mean operative time of 65.6 minutes after plication of peritoneal pouch in front of the rectum, which is less than mean of 98 minutes reported by Gomes-Ferreira et al., 20 77.5 minutes reported in Awad et al., 2 and 60 minutes reported in Ismail et al. 15
The preoperative procedure used by our team included 1 day bowel preparation that was comparable with the initial experience of Potter et al., 19 wherein all patients were admitted preoperatively for overnight mechanical bowel preparation. This protocol was changed by his team since February 2007, avoiding preoperative mechanical bowel preparation without complication. In addition, he changed hospital stay from 2 to 3 days in an outpatient procedure without any complications. 19
In our technique for LSR, we preserved the lateral wings of mesorectal peritoneum attached to the rectum. Recently, the same principal was used with fixation to the sacral promontory using ProTack™ that proved to be a simple, safe, and effective procedure, showing promising results in children. 13
We reported only one mucosal prolapse during 19.5 months mean follow-up, while Saxena et al. reported no recurrence after 24 months follow-up. 23 Similarly, low rates of recurrence for other laparoscopic rectopexy procedures have been reported provided that the surgeons have enough experience. Ismail et al. reported a series of 40 patients with no recurrences, 15 as compared with Puri 14 and Potter et al. 19 who each reported recurrence rate of 5% despite using different techniques. LSR is followed in children with recurrent RP by Saxena et al.23,24
Although preoperative neurobehavioral disorder and constipation increase the risk of postoperative problems reaching up to 61% in a study for LSR in 27 patients, 14 of them had anorectal malformation, bladder exstrophy, sacrococcygeal teratoma, and myelomeningocele or associated with mental retardation and Asperger's syndrome,5,6,8 we proved in this study that LSR is technically simple, safe, and effective when performed in selected pediatric patients.
Till now, there is no treatment algorithm for recurrent RP in children owing to the variety of surgical techniques described and the low level of evidence within heterogeneous studies with small number of cases.19,20
Based on the results of this study, LSR is a valid option for treating RP in children with no associated neurological problems after failure of conservative treatment. Laparoscopic posterolateral suture rectopexy could be the standard approach in pediatric RP. Consequently, a surgeon should tailor intervention that suits individual patients, taking previous surgery and type of prolapse into account.
Conclusions
LSR is an efficient technique in well-selected cases of recurrent RP among children and could reverse this underlying pathology. Experience and strict selection criteria are mandatory for success. Longer follow-up and evidence are needed to standardize the technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.