
Abstract
Abstract
Introduction:
In pediatric population, the two most common indications for splenectomy include traumatic rupture and hematological diseases such as hereditary spherocytosis, idiopathic thrombocytopenic purpura, sickle cell disease, and autoimmune hemolytic anemia. Traditionally, splenectomy has been an open procedure; however, since the first laparoscopic splenectomy was reported in 1991, the minimally invasive laparoscopic approach has become increasingly popular. In most public hospitals in Brazil, where vessel sealing devices are not available, most surgeons seem to prefer open splenectomy to guarantee intraoperative safety and improved outcomes.
Objectives:
To compare outcomes between open and laparoscopic splenectomy in children in a public hospital in Brazil.
Materials and Methods:
Retrospective study conducted between January 2010 and June 2018. Patients from 0 to 14 years old who underwent open or laparoscopic splenectomy at the University Hospital of Federal University of Paraná were included. Clinical, laboratory, imaging, and surgical data were collected.
Results:
For 8 years, 35 patients underwent splenectomy. Mean age was 4 years old and 54% were female. Of the 35 subjects, 69% had sickle cell anemia and 23% spherocytosis. The most common indication for surgery was a previous episode of splenic sequestration. The 13 laparoscopic surgeries were performed without harmonic scalpel or other vessel sealing devices. During the laparoscopic procedure, 2 patients experienced intraoperative complications: bleeding and prolonged surgical time due to technical problems with the equipment. Mean operative time was higher in laparoscopy group than in open group (186 minutes versus 66 minutes). Oral feeds began earlier on the laparoscopic group. Postoperatively, there were more complications on the open group, and no reoperations. There was only one fatality, likely secondary to fulminant sepsis, which occurred 34 days after the surgery in a patient who was undergoing prophylactic oral antibiotics therapy.
Discussion:
Performing laparoscopic splenectomy without harmonic scalpel or other vessel sealing devices is feasible, but it implicates in a significantly higher surgical time. Laparoscopic splenectomy had earlier oral feeds and fewer complications than open surgery.
Introduction
Minimally invasive surgery is considered to be one of the major advances to surgical practice in recent history. Since first described in 1991,1,2 laparoscopic splenectomy has become widely accepted as an alternative to the traditionally open approach. Laparoscopic approach to splenectomy has been shown to be a relatively safe procedure, with low mortality and complication rates, as well as shorter hospital stays and recovery time, low hemorrhage rate, better surgical access, less postoperative pain, and better aesthetic result.2,3 Currently, its range of indications is varied and addresses a considerable number of pathologies, especially traumatic rupture and complications of hematological diseases.4,5 The goal of this study is to compare outcomes after open and laparoscopic splenectomy and to describe the surgical technique used by our service. Owing to the lack of availability of harmonic scalpel or other vessel sealing device, our pediatric surgery service uses an anterior or anteroposterior approach and monopolar energy—a method that has not only been shown to be both safe and efficient, but also may be an option for other institutions that also have limited resources.
Materials and Methods
This is a retrospective review of pediatric surgery patients who underwent splenectomy at the Hospital de Clínicas of Universidade Federal do Paraná and their postoperative outcomes. Medical records were reviewed and analyzed for gender, age, indications for splenectomy, surgical technique, operative and postoperative complications, postoperative length of stay, and surgical time. Preoperative diagnoses were established by pediatric hematologist and all indications of splenectomy were carefully discussed by a multidisciplinary team, including pediatric surgery. Patients were divided into two groups based on surgical approach: (1) open splenectomy and (2) laparoscopic splenectomy. The choice of technique, laparotomy versus laparoscopy, was determined by surgeon's preference. The primary endpoint of this study is to compare outcomes, including operative time, intraoperative bleeding and complications, postoperative complications, and need of transfusion.
Preoperatively, all patients were administered polyvalent pneumococcal, meningococcal, and Haemophilus influenzae vaccines, and underwent ultrasonography to estimate spleen size and the presence of accessory spleens and gallstones. Routine antibiotic prophylaxis was administered at the onset of surgery.
All the data obtained through medical records were registered in a spreadsheet (Microsoft Excel®) and subsequently analyzed statistically utilizing the Prism Graphpad software.
The study was approved by the IRB.
Surgical technique
Two different approaches of splenectomy were analyzed in this study: laparoscopic and open. In the open laparotomy procedure, a left subcostal incision was made and the intestines were mobilized as necessary to expose the underlying spleen. Dissection was performed at the splenic hilum and greater curvature of the stomach, exposing the hilar and short gastric vessels. Once exposed, the vessels were ligated and divided, and the spleen was removed. 6 Further exploration was made to find any accessory spleen. The cavity was reviewed and the abdomen was closed in a standard way.
In the laparoscopic group, patients were positioned in a slightly right lateral decubitus position and three trocars were placed, two 5-mm and one 10-mm, with the 10-mm trocar set in an infraumbilical incision. Pneumoperitoneum was performed either with a Veress needle or through an open incision in the abdominal wall and was maintained at the maximum of 12 mmHg. Two 5-mm surgical ports were inserted under direct vision: one on the epigastric at the midline and the other in the left flank.6,7 A suture was passed to lift the lower splenic pole, and dissection with monopolar or manual ligation was performed from the lower to the upper splenic pole. individual hilar vessels were isolated and controlled with clips (metallic or hemolock®) or manual ligature before division (Fig. 1). The spleen was removed through the largest port with a plastic bag. To ensure hemostasis, abdomen was reviewed.
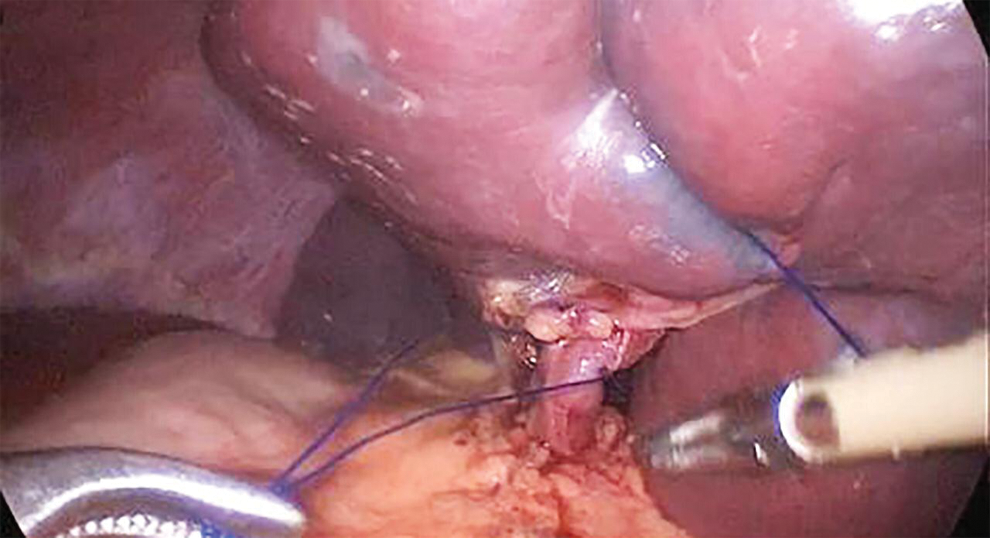
Manual ligature of hilar vessels.
Results
The study included 35 patients who underwent splenectomy at the University Hospital of Federal University of Paraná between January 2010 and June 2018. Of these subjects, 22 underwent open surgery (laparotomy group) and 13 video splenectomy (laparoscopy group). For 32 (91.4%) patients, a history of splenic sequestration was the main indication for splenectomy; 24 (68.5%) patients had sickle cell anemia and 8 (22.8%) had hereditary spherocytosis. The remaining 3 patients had idiopathic thrombocytopenic purpura, autoimmune hemolytic syndrome and hypersplenism, respectively.
Preoperative data comparison
Table 1 shows the demographic and clinical variables of each group. The mean age in the laparotomy group was 4.8 years versus 4.3 years in the laparotomy group. There was no statistical difference when comparing the mean age of the patients between the groups (t-test, P = .66).
Groups Demographic and Clinical Variables
At baseline, the two surgical groups were statistically similar. There was no significant difference in preoperative serum hemoglobin between the laparotomy and laparoscopy groups, with mean serum hemoglobin of 9.22 and 8.67 mg/dL, respectively (t-test P = .37). Ultrasonographic findings of the abdomen were also compared: preoperative cholelithiasis was observed in one of the patients from the laparoscopy group. Three patients in laparotomy group had undergone previous laparoscopic cholecystectomy, compared with only 1 patient in the laparoscopy group. Ultrasonography also revealed a slightly larger spleen axis length in the laparotomy group (11.76 cm) compared with the laparoscopy group (11.64 cm); however, the difference was also not statistically significant (t-test, P = .93).
Surgery and early postoperative data
A subcostal incision was chosen in all patients submitted to open surgery and all received antibiotic prophylaxis with cefazolin. Two patients from the laparoscopy group experienced intraoperative complications: intraoperative bleeding with no blood transfusion needed and prolonged surgical time due to technical difficulties with the insufflator (Table 2). Surgical time was statistically longer in the laparoscopy group with a mean procedure time of 185.7 minutes (range: 85–390) compared with mean surgical time of 66.4 minutes (range: 45–120) in the laparotomy group (t-test, P = .01) (Fig. 2).
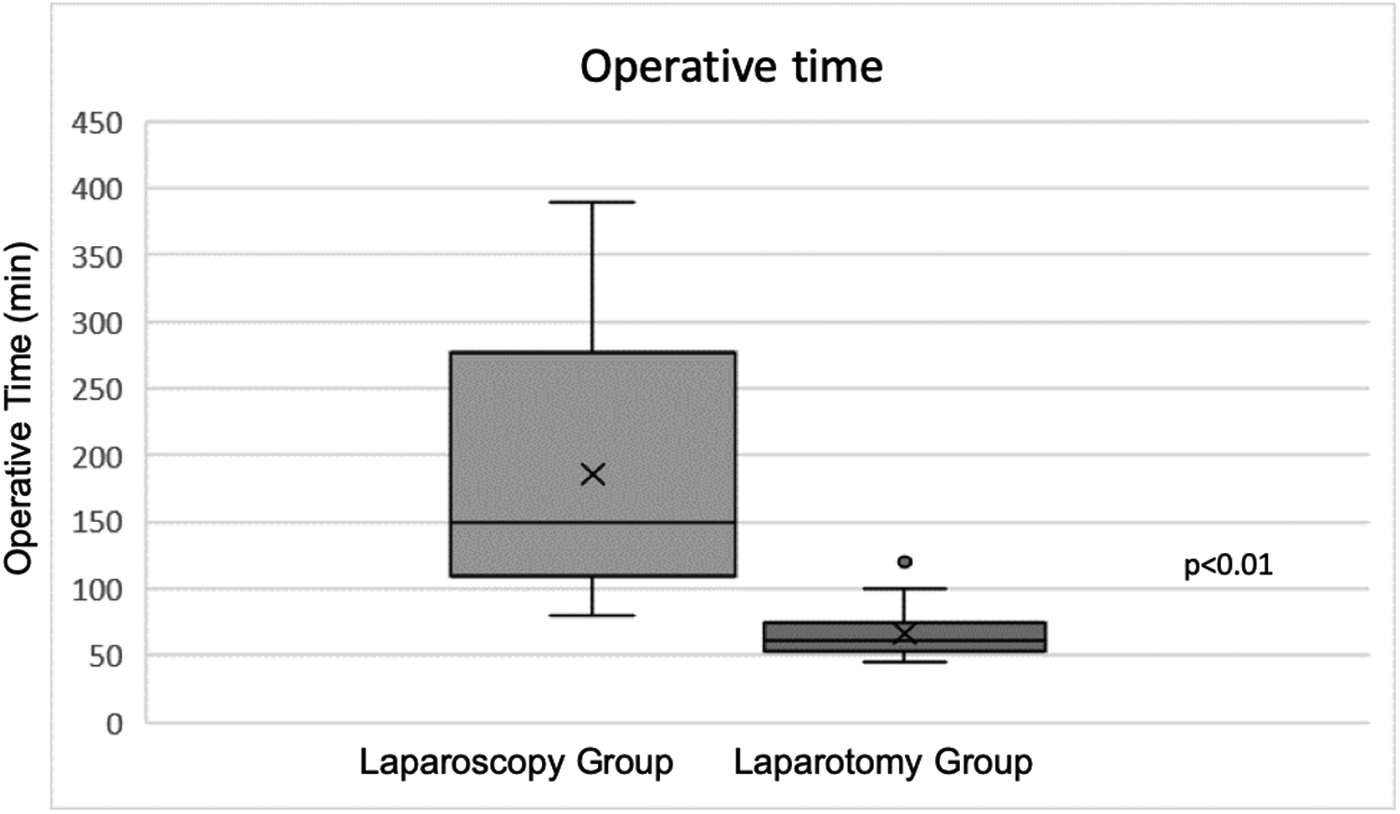
Comparison between laparotomy and laparoscopy group operative time (P < .01).
Surgery and Postoperative Outcomes
In the postoperative period, the beginning of oral feeds occurred earlier in the laparoscopy group (t-test, P = .04), in which 53.8% of the children received diet in the immediate postoperative period, versus 13.6% in the laparotomy group. In the laparotomy group the introduction of oral feeds occurred predominantly on the first postoperative day (72.7%). The longest time for diet introduction in both groups was 2 days (Table 2).
A total of 7 subjects experienced postoperative complications during their hospitalization: 6 (85.7%) belonged to the open laparotomy group and 1 (14.3%) to the laparoscopic surgery group; therefore, laparotomy had significantly more early postoperative complications than laparoscopy (chi-square test, P = .01) (Table 2). Complications in the laparotomy group included bacterial pneumonia, surgical wound infection, oxygen desaturation, febrile episode, diarrhea, and abdominal distension. In the laparoscopy group, the complication presented was the need for blood transfusion.
The mean length of hospital stay was statistically similar: 3.8 days in the laparotomy group and 3.7 in the laparoscopic group (t-test, P = .80) (Table 2).
Late postoperative data
Patients in both groups were evaluated postoperatively at 7, 30, and 90 days. At the 1-week follow-up, the only reported complaint was a febrile episode in the laparoscopy group. One month after surgery, there was one surgical wound infection and one febrile episode in the laparotomy group; in the laparoscopy group, one of the patients died after a probable postsplenectomy fulminant sepsis that occurred 34 days after the surgery in a patient who was undergoing prophylactic oral antibiotics therapy.
At 3 months' return, none of the patients presented with any complications.
The size and weight of the spleen were evaluated in anatomopathological examination. The mean size of the organ removed in the children from laparotomy group was 12.47 cm on its largest axis, compared with 11.5 cm in laparoscopic group (t-test, P = .23). The mean weight of the spleen was 272.9 g in the laparotomy group and 209.9 g in the laparoscopy group (t-test, P = .36). Overall, was no statistical difference in splenic length and weight between groups (P > .05) (Table 2).
Discussion
For the past few decades, minimally invasive surgical approaches have become increasingly popular. Although evidence-based pediatric surgical practice has improved over the years, more than a third of the surgical procedures still lack sufficient evidence-based literature support. 8 In 2002, laparoscopy was deemed the gold-standard splenectomy technique; however, the benefits of this minimally invasive approach have not been demonstrated by strong, level 1 evidence, but instead have been described by the first-hand reports of experienced surgeons. 9
In the pediatric population, splenectomy is mainly performed for benign hematological diseases, including hereditary spherocytosis, idiopathic thrombocytopenic purpura, sickle cell disease, and autoimmune hemolytic anemia. 9 In our study, the majority of patients (68.5%) had sickle cell disease.
Massive splenomegaly has been defined in literature as splenic weight ranging between 500 and 1000 g. 10 Zhu et al. defined massive splenomegaly as a splenic margin below the umbilicus or anteriorly extending over the midline. 11 Laparoscopy is the gold-standard procedure for splenectomy; however, it is still controversial and even considered a contraindication for massive splenomegaly. 12 We used the limit of 500 g on anatomopathological examination to define massive splenomegaly. In this study only 4 patients had massive splenomegaly, half of them were approached with laparoscopy and the other half with laparoscopy. There was no statistically significant difference in splenic size between the two groups.
In our patients, individual hilar vessels were isolated and controlled with clips (metallic or hemolock) or manual ligature before division. Some authors state that clips are easily placed but can become dislodged and require accurate vessel dissection and that sutures can be a tedious option, are time consuming in laparoscopic surgery, and leave foreign materials. 13 A review of the literature reveals that surgical technique using vessel-sealing systems, such as Ligasure, is considered the only means of achieving hemostasis without the use of clips and endostaplers.14–18 In this study, however, we were able to perform a laparoscopy using only monopolar and manual ligation with consistent hemostasis and safe surgical outcomes. The only disadvantage to our approach is longer operative time.
Laparoscopy is a feasible, safe, and effective surgical procedure alternative to open splenectomy for pediatric patients. 19 Feng et al. demonstrated that laparoscopy was associated with shorter hospital stays, less blood loss, and longer operative times in children. Furthermore, laparoscopy has the potential of reducing blood loss during operation because of reducing the trauma of surgical access compared with laparotomy, which may further shorten the length of hospital stay. 19 In our study, however, the only patient who received blood transfusion was in the laparoscopy group. In accordance with other studies, our laparoscopy group experienced longer operative time and earlier commencement of oral diet. Therefore, the longer operative time did not reflect on longer hospital stay, since it was similar on both groups.
This study also demonstrated a higher risk of postoperative complications, such as pneumonia, surgical wound infection, diarrhea, and fever, after laparotomy compared with laparoscopy.
The risk of infection due to encapsulated bacteria (Streptococcus pneumoniae, H. influenza, and Neisseria meningitides) is increased after splenectomy, and postoperative antibiotic prophylaxis should be administered routinely. 20 The study monitored the patients on postoperative day 7, 30, and 90 to monitor late complications. Despite antibiotic prophylaxis, both groups experienced some infection-related complications, including a surgical wound infection postlaparotomy, fever in both groups, and death by septic shock after laparoscopy.
Literature comparing the risks and benefits of open versus laparoscopic splenectomy in children is limited. Without robust reviews and randomized clinical trials, the decision to perform either laparoscopy or laparotomy usually depends on surgeon preference and experience. 19 In this study there was a statistically significant difference demonstrating that laparoscopy without sealers or staplers has longer perioperative time but earlier oral feed times and fewer complications than open surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.