
Abstract
Abstract
Introduction:
Few centers worldwide have advanced single-incision pediatric endosurgery (SIPES) for pediatric age group. Up to our knowledge this is the first study assessing the safety of SIPES cholecystectomy in children with sickle cell disease (SCD) done by surgical residents.
Aims:
To determine the feasibility, safety, and expediency of SIPES cholecystectomy in children with SCD performed by surgical residents.
Materials and Methods:
Retrospective study of all SIPES cholecystectomies performed in our unit from April 1, 2011 to March 31, 2018. We compared the outcome of SIPES cholecystectomy done by fellows and residents. SIPES Covidien 5–12 mm port was inserted through umbilicus. Long 50 cm laparoscope, straight regular instruments, and transabdominal gallbladder traction suture were used in all patients. The cystic duct and artery were identified and divided. The gallbladder is then dissected off the liver and extracted from the abdomen through the port.
Results:
Forty-three SCD patients underwent SIPES cholecystectomy for 7 years. Mean HbS was 37.56%. Mean age was 10 years. Twenty-four cases (56%) and 19 (44%) were performed by 8 fellows and 10 residents, respectively. Nine other procedures were done simultaneously with cholecystectomy and were excluded from the mean operative time (MOT). The MOT for all cases was 85 minutes, 78 minutes for fellows and 94 minutes for residents (P value is <.001). One extra port was inserted in 2 patients at the beginning of the series.
Conclusion:
SIPES cholecystectomy in children with SCD is safe and feasible if done by residents under supervision. Stepwise training is essential in this challenging surgery. Involving residents with other SIPES procedures and hands-on minimally invasive surgery single port workshops help them in improving their skills.
Introduction
Minimally invasive surgery (MIS) has revolutionized surgical treatment. Few centers worldwide have advanced single-incision pediatric endosurgery (SIPES) for pediatric age group. SIPES cholecystectomy is safe and a reasonable alternative to conventional laparoscopic cholecystectomy (CLC), leaving almost an invisible scar and great patients' satisfaction.1–3 Currently SIPES cholecystectomy is an alternative option to CLC in the routine management of choletheiasis.4–7 SIPES technique presents a challenge to teaching hospitals where you should balance the training efficacy and patients' safety. Learning curve needs workshops either animal or simulation laboratory to improve surgeon's skill.
SIPES cholecystectomy is preferred for patients with sickle cell disease (SCD) because of the advantages of easier organ extraction through the umbilicus plus more than one operation could be done at the same time. 8 Although it has been reported before that mean operative time (MOT) in SIPES cholecystectomy is longer, but still it is comparable with CLC.9,10 Up to our knowledge there is no study assessing the safety of SIPES cholecystectomy in children with SCD performed by residents.
Aims
To determine the feasibility, safety, and expediency of SIPES cholecystectomy in children with SCD performed by surgical residents.
Materials and Methods
Retrospective study of all SIPES cholecystectomy performed by residents and fellows from April 1, 2011 to March 31, 2018. The fellow is a surgeon who has completed his general surgery residency and elected to complete further training in pediatric surgery. The resident is a doctor who is receiving training in adult general or pediatric surgery. The pediatric surgery rotation for surgical residents started from year 3. The training period for fellows is 6 months, whereas for residents it ranges from 6 weeks to 3 months. Operative time in minutes is calculated from skin incision to closure. After induction of general anesthesia and endotracheal intubation, patient was placed in supine position. SIPES port of 1.5 cm was inserted transumbilical. Covidien© (Medtronic) 5–12 mm port was used in all cases. Pneumoperitoneum has been created and maintained at a constant pressure of 8–10 mmHg. Long 50 cm laparoscope and straight regular instruments were used in all procedures. Traction of gallbladder fundus to right side of the abdominal wall was done by transabdominal suture introduced percutaneously by curved needle. Once the gallbladder is properly retracted, the cystic duct and artery were identified, double clipped, and divided. The gallbladder is then dissected off the liver with hook diathermy and extracted from the umbilicus.
Results
Forty-three patients underwent SIPES cholecystectomy by surgical trainees for 7 years. Seventeen (40%) were male and 26 (60%) were female. Mean HbS was 37.56% (17.80–49.50). Mean age was 10 years (6–14 years). Twenty-four cases (56%) and 19 (44%) were performed by 8 fellows and 10 residents, respectively. The MOT for all cases was 85 minutes (62–127 minutes); 78 minutes (62–98 minutes) for fellows and 94 minutes (76–127 minutes) for residents. P value is <.001 (Fig. 1). Seven splenectomies, one appendectomy, and one herniotomy were done simultaneously with cholecystectomy and they were excluded from the MOT. One extra port was needed in 2 patients in the beginning of the series. There were no conversion. There was neither postoperative pulmonary complications nor wound infection.
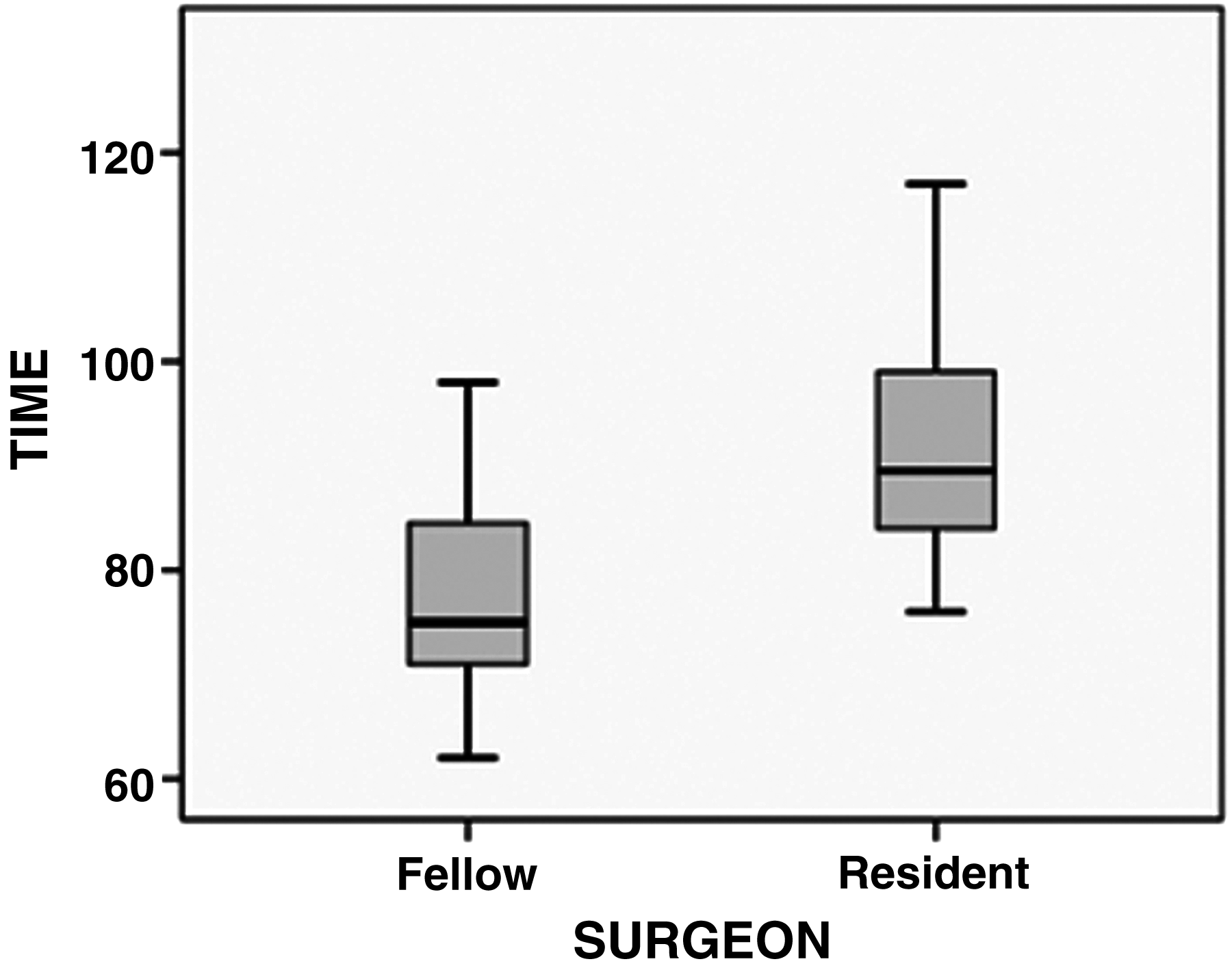
Mean operative time.
Discussion
Laparoscopy has constantly evolved with the aim of scarless surgery. The first sign of reducing the number of access ports was in the late 90s by a group in Hong Kong. 11 Natural orifice transluminal endoscopic surgery (NOTES) emerged as an option to laparoscopy. Single-incision laparoscopic surgery (SILS) through the umbilicus was used to replace NOTES to avoid the access through normal orifices and the risk for intra-abdominal contamination.12,13 SILS cholecystectomy is one of the most popular procedures in both adults and children.4,5
In 2003, SIPES has been introduced at our pediatric surgery department for many procedures such as cholecystectomy, splenectomy, appendectomy, Mitrofanoff, ovarian cystectomy, and fundoplication. SIPES became our standard technique for cholecystectomy in children with SCD in 2011 as our skills have improved with steep learning curve.
There are many types of SILS ports with different sizes in the market.3,13 The choice of the port depends on surgeon, availability, and cost factor. We found that Covidien (Medtronic) port is the most suitable one as it is small in size, easy access and it can adopt 15 mm port for introducing GIA® stapler and endobag if the procedure is combined with splenectomy.
Either transabdominal suturing or introducing a 2 mm Minilap Alligator grasper through the umbilicus or through a separate incision were used for proper visualization of Calot triangle as it is an essential step in SIPES cholecystectomy. 13 We have modified gallbladder fundus traction with straight needle by curved needle which was introduced percutaneously without intracorporeal aid (Fig. 2).
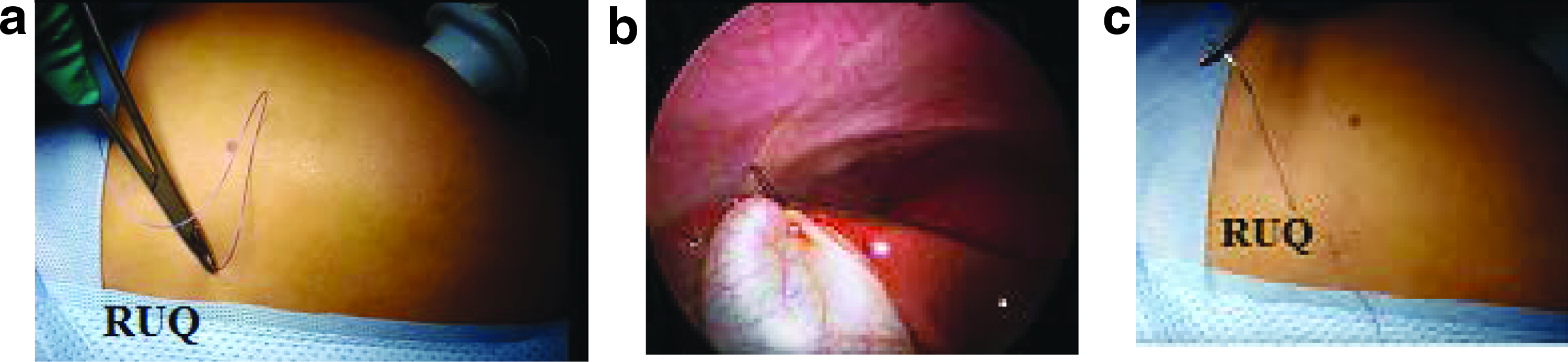
Modifications of gallbladder traction.
SCD is an autosomal recessive disorder, which is endemic in southern and eastern regions of Saudi Arabia. 14 Cholecystectomy is the most common surgical procedure performed in patients with SCD. In laparoscopy there are many pathophysiological changes associated with pneumoperitoneum and increased operative time, which may lead to perioperative complications such as postoperative acute chest syndrome. Dilip et al. recommended that CLC should be performed by a senior and experienced surgeon in SCD patients to minimize pulmonary complications. 15 Our series showed that SIPES cholecystectomy is well tolerated by SCD patients when performed by trainees.
SIPES is good for retrieving large-sized spleen through umbilicus, instead of Pfannenstiel–Kerr incision in SCD patients when cholecystectomy is combined with splenectomy. We agree with others that SIPES is a safe and feasible technique for combined splenectomy and cholecystectomy. 8
The effects of instrumental crowding, as well as the absence of triangulation, are among the common technical challenging issues; newly developed angled light cord extensions and extra long endoscopes allowed enhanced visualization and better maneuverability. 16 Steep training methods was applied for our residents, starting by assisting then proceeding to gall bladder bed dissection and later on Calot dissection. Confusion of crossing image is another issue in SIPES, which will be adapted after the first 10–15 minutes.
Our MOT is long for SIPES cholecystectomy in comparison with the CLC. Our data showed that the MOT for fellows is significantly lower than that for residents. We think that the fellows are familiar with conventional MIS, in particular with CLC at the time of their training in general surgery.
Conclusion
SIPES cholecystectomy in patients with SCD performed by residents is safe and feasible with almost invisible scar without increase in morbidity. More than one procedure could be done at the same time. Learning curve has improved with experience and hands-on MIS workshops.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.