
Abstract
Abstract
Purpose:
To characterize injury patterns and institutional trends associated with the utilization of laparoscopy in the management of pediatric abdominal trauma.
Methods:
The National Trauma Data Bank (2010–2014) was queried for encounters involving patients ≤14 years who underwent an open or laparoscopic abdominal operation within 48 hours of emergency department arrival. Patient, injury, and hospital characteristics associated with each approach were identified. Multivariate logistic regression was used to evaluate the influence of patient and hospital characteristics on operative approach.
Results:
Laparoscopy comprised 7.8% (n = 355) of all abdominal trauma operations. Patients undergoing laparoscopy had lower injury severity scores and higher Glasgow Coma Scale scores on arrival compared with laparotomy subjects (P < .001). Laparoscopic patients also had a shorter length of hospital stay (5.0 versus 8.6 days, P < .001), but longer time to the operating room (9.2 versus 6.3 hours, P < .001) compared with their open counterparts. The proportion of cases managed laparoscopically increased from 6.2% in 2010 to 10.1% in 2014 (P = .013), with increase in utilization primarily driven by university hospitals (P = .026) and level I pediatric trauma centers (P = .043). Conversion to laparotomy was uncommon (18.6%), and mortality in the laparoscopic cohort was low (0.4%).
Conclusions:
Use of laparoscopy has increased in the pediatric abdominal trauma population, typically in a less injured cohort of patients. As familiarity with and availability of minimally invasive techniques increase, this trend will likely continue.
Introduction
Over the past few decades, the standard of care for many abdominal injury patterns in pediatric trauma has moved toward nonoperative management (NOM).1,2 Successful application of this principle to the hemodynamically stable patient with blunt solid organ injury has reduced the role of operative intervention, given the low rate of NOM failure (∼5%).3,4 Abdominal exploration is now largely confined to patients with: (1) penetrating injuries that violate the peritoneum, (2) pneumoperitoneum or evidence of hollow organ perforation, and/or (3) persistent hemodynamic instability with suspected intra-abdominal pathology. 3 While these clinical scenarios generally mandate operative intervention, other patients may present a diagnostic and therapeutic challenge, such as the hemodynamically stable child with unexplained free intraperitoneal fluid.
Laparoscopy has been suggested as a diagnostic—and potentially therapeutic—approach when clinical uncertainty is high. 5 Laparoscopic exploration is attractive because it carries relatively low morbidity, and data regarding other diagnostic adjuncts, such as a focused assessment with sonography in trauma (FAST), remains mixed in the pediatric trauma literature.6,7 While laparotomy is the gold standard for patients requiring surgery, 8 it is associated with significant morbidity, occasional mortality, and an increased risk for future intestinal obstruction.8,9 In the appropriate clinical setting, laparoscopy can be safe and may reduce the rate of nontherapeutic or negative laparotomy.3,10 Unfortunately, research regarding the role of laparoscopy in infants and children with abdominal trauma requiring operative intervention is limited to small case series11,12 and single-institution reviews.3,5,10 To date, there are no multiinstitutional or nationwide investigations of the use of laparoscopy in pediatric abdominal trauma.
We hypothesized that pediatric patients undergoing laparoscopy after abdominal trauma would represent a more hemodynamically normal subpopulation and, therefore, would present with lower injury severity scores (ISS), higher Glasgow Coma Scale (GCS) scores, and mortality would be low. We further hypothesized that because minimally invasive approaches are now used more frequently in pediatric surgery overall, utilization of laparoscopy for trauma would increase over time. To illustrate the level of surgical uncertainty in this subset of patients, we additionally sought to examine the characteristics of patients who underwent an open abdominal operation after beginning with laparoscopy.
Materials and Methods
Study design and population
A retrospective cohort study was performed using the National Trauma Data Bank (NTDB), a national de-identified database sponsored by the American College of Surgeons (ACS) Committee on Trauma. NTDB is the world's largest trauma database, including data from over 900 centers. 13 NTDB was queried from 2010 through 2014 for all encounters involving patients ≤14 years who underwent an abdominal operation within 48 hours of emergency department (ED) arrival. This cohort was further dichotomized into patients who received an open and/or laparoscopic intervention. Patients who initially underwent laparoscopy but later required an open operation were also identified. Figure 1 presents the sample inclusion flow diagram.
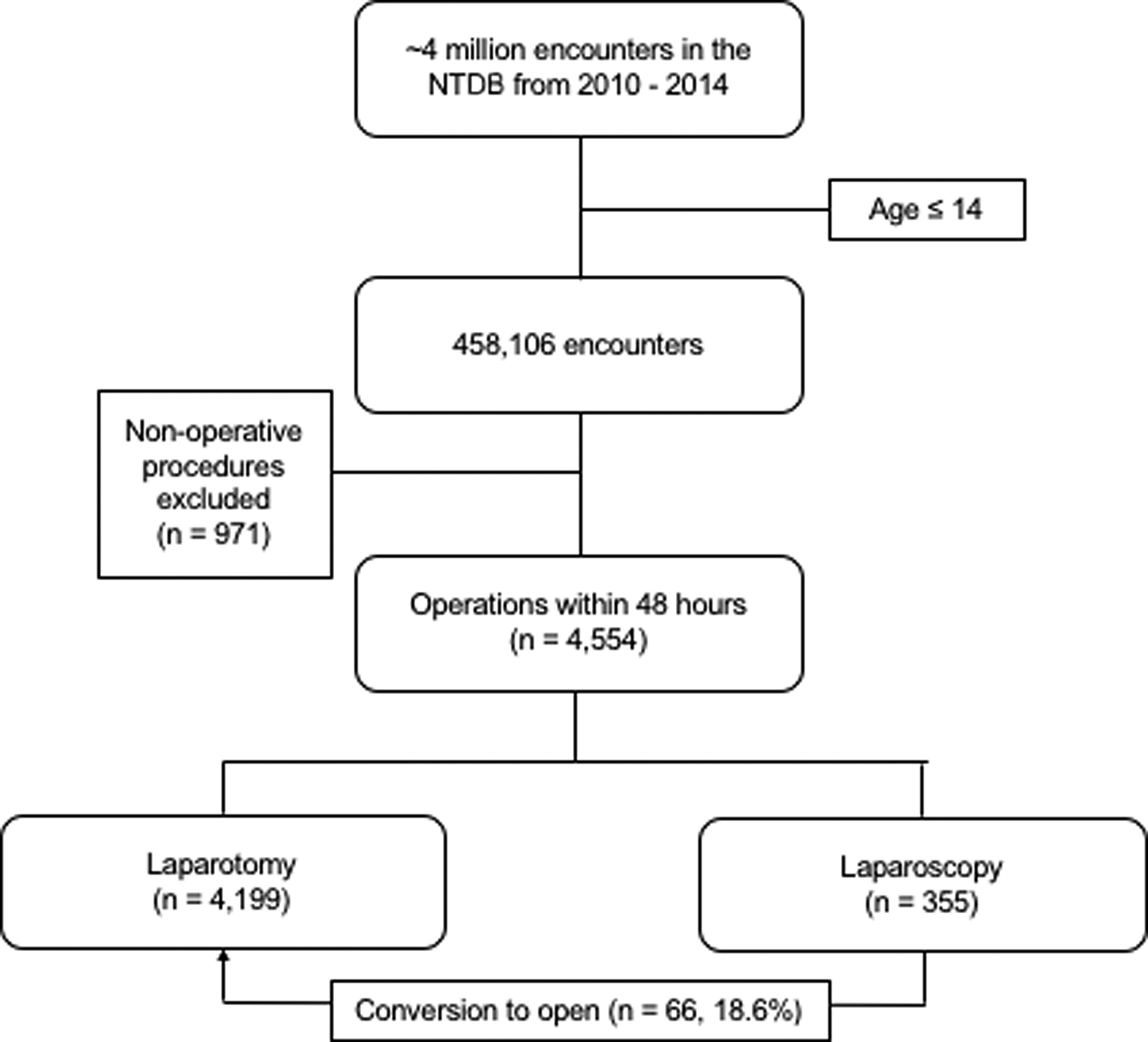
Inclusion and exclusion criteria for the study cohort. NTDB, National Trauma Data Bank.
Abdominal operations were defined using procedure codes 43.XX through 54.XX from the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM), corresponding to all “operations on the digestive system,” excluding operations on the esophagus. This cohort was refined by removing all encounters that only included “procedures” and not abdominal “operations.” Two investigators (R.S. and M.G.) performed this review manually with predetermined definitions and agreed on all excluded encounters. For example, encounters with procedure codes and without operative codes, such as 51.10, “endoscopic retrograde cholangiopancreatography (ERCP),” or 48.23, “rigid proctosigmoidoscopy,” were excluded as these interventions were classified as “procedures” and not abdominal “operations.” The remaining cohort was dichotomized into patients who underwent a laparoscopic intervention and those that did not, using the abstracted procedure code descriptions.
A conversion rate from laparoscopy to open abdominal operations was estimated by querying all remaining procedure codes for the sample that underwent laparoscopy for subsequent abdominal operations. The same methodology was utilized to dichotomize encounters into those that solely underwent laparoscopy and those in which an open procedure was performed. For example, while the first ICD-9-CM procedure code may be 54.21, “laparoscopy,” the same encounter may include a second code of 54.11, “exploratory laparotomy,” suggesting conversion to an open approach. A subset of ICD-9-CM procedure codes were either ambiguous or could be performed utilizing either laparoscopy or laparotomy but not specified. To present the most conservative estimated conversion rate, these cases were classified as open operations.
Patient, disease, and hospital characteristics associated with each operative approach were identified. Patient demographic characteristics included age, race, ethnicity, and gender. Disease characteristics included ISS, GCS score, mechanism of injury (blunt or penetrating), immediate disposition from the ED (operating room, intensive care unit, floor, etc.), time to procedure, hospital length of stay (LOS), and mortality. Hospital characteristics included institutional designations for teaching status (teaching hospital, community, etc.), ACS trauma center verification level, and ACS pediatric trauma center verification level.
Statistical analysis
We used STATA® 14.2 (StataCorp, College Station, TX) to perform all statistical analyses. Descriptive statistics are presented as means (standard deviations) and medians (range) for parametric and nonparametric data, respectively. Categorical variables are presented as frequencies (percentages). Student's t-test and analysis of variance calculations were performed for continuous variables, as well as Pearson's chi-square test of independence for categorical variables. All P-values were estimated using a two-tailed distribution with a significance level set a priori to α = .05. A multivariate logistic regression model was developed to evaluate the influence of patient and hospital characteristics on operative approach. Missing data were minimal (<10%) in all cases and were thus ignored in final analyses. This study protocol was approved by the institutional review board at the University of Pennsylvania on September 5, 2017 (Protocol No. 828145).
Results
Cohort characteristics
The final cohort included 4554 unique patient encounters. Patient, disease, and hospital characteristics are presented in Table 1. Overall, 355 (7.8%) pediatric patients underwent a laparoscopic intervention within 48 hours of arrival to the ED. Age, ISS, GCS, mechanism of injury, disposition from the ED, time to procedure, hospital LOS, and mortality were statistically different between children who underwent laparoscopy compared with those who underwent laparotomy. Patients undergoing a laparoscopic abdominal operation were found to be older, had a lower ISS, higher GCS, and were more likely to experience penetrating trauma. There were no differences in race, ethnicity, or gender between groups. Laparoscopy was more likely to occur at university hospitals compared with community and nonteaching hospitals, as well as at ACS-verified pediatric level I trauma centers versus non–pediatric-designated trauma centers. Table 2 presents covariates found to be independently associated with primary use of laparoscopy after adjusting for variables found to be significant in bivariable models. Older age, GCS >8, ISS <16, and admission to a university hospital or pediatric level I trauma center was associated with increased odds of initial laparoscopy.
Characteristics Associated with Operative Approach (n = 4554)
Values shown in bold represent statistical significance at p < 0.05.
n (%) for categorical variables; mean (standard deviation) for all continuous variables except ISS where data are presented as median (interquartile range).
ACS, American College of Surgeons; ED, emergency department; GCS, Glasgow Coma Scale; ISS, injury severity scores; LOS, length of stay.
Independent Predictors of Initial Use of Laparoscopy for Operative Approach after Adjustment in Management of Pediatric Abdominal Trauma
Mechanism of injury, disposition, time to procedure, and American College of Surgeons verification level were also included in the final model.
CI, confidence interval; GCS, Glasgow Coma Scale; ISS, injury severity scores; OR, odds ratio.
Regardless of teaching status or ACS trauma designation level, laparoscopic management of pediatric trauma increased steadily from 2010 to 2014. A total of 6.2% of all urgent (<48 hours) abdominal operations utilized laparoscopy in 2010, increasing to 10.1% in 2014. When stratified by hospital designation and teaching status, utilization trends of laparoscopy were mostly attributed to increased use among university hospital centers (P = .015) and level I-designated pediatric trauma centers (P = .1) (Fig. 2). From 2010 to 2014, the proportion of laparoscopic cases performed nearly doubled at university hospitals (6.3%–12.2%), while the frequency remained relatively stable at nonteaching and community centers. The rate of laparoscopy also increased at level I pediatric trauma centers, from 7.5% in 2010 to 13.3% by 2014 (Fig. 3).
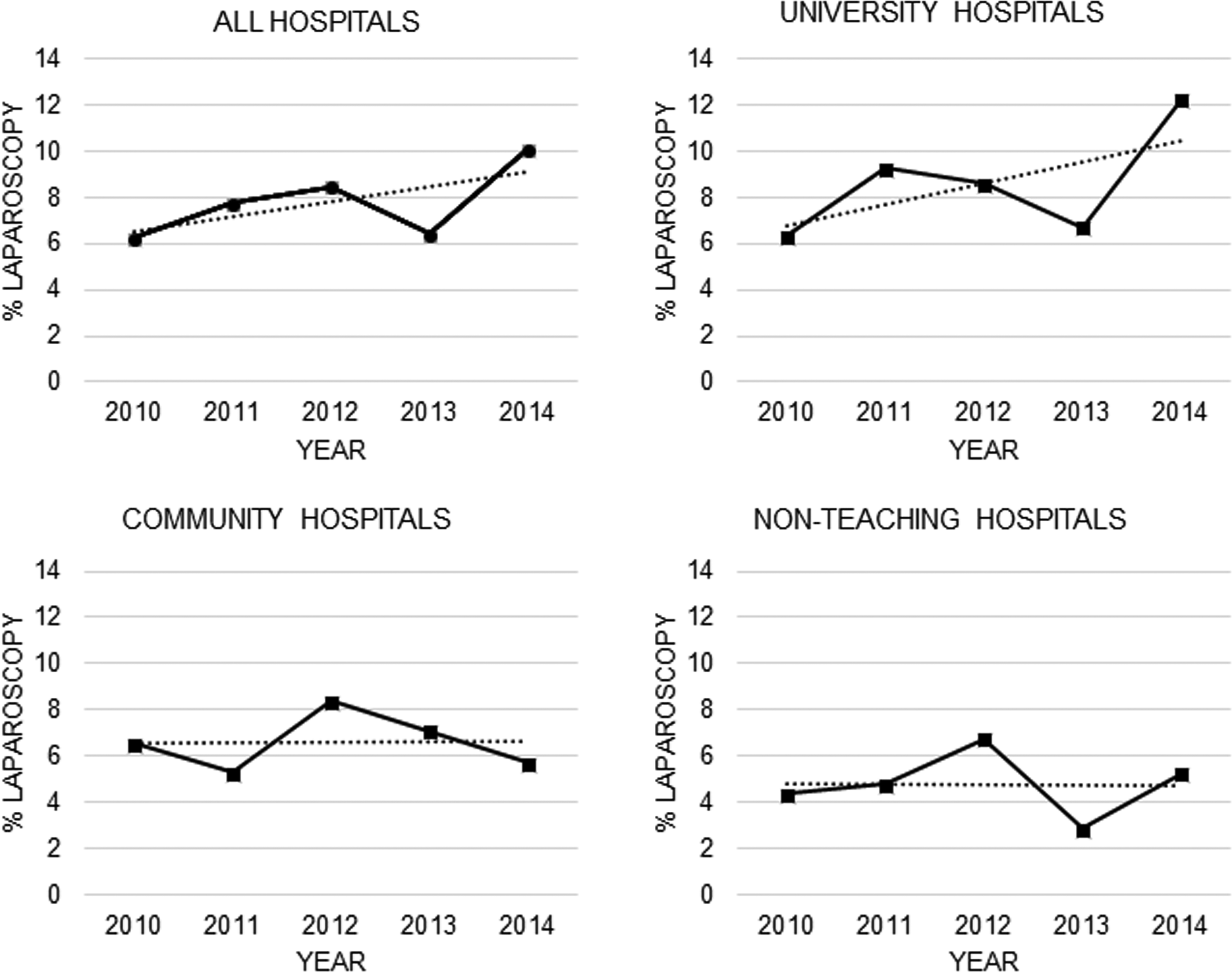
Use of laparoscopy is increasing (top left, P = .007). However, this shift is almost entirely accounted for by increasing use in university-based hospitals (top right, P = .015), with no trend either for increased or decreased use demonstrated in community or nonteaching hospitals (P = NS). NS, not significant.
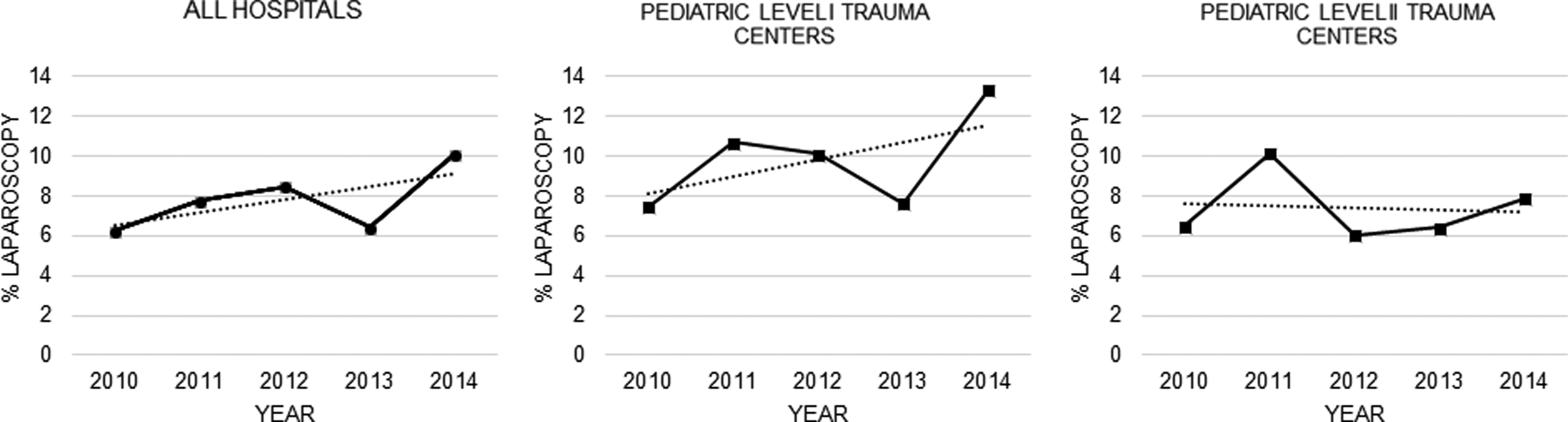
Increased use of laparoscopy may also be accounted for by growing utilization at pediatric level I trauma centers (middle, P = .1). No trend either for increased or decreased use was demonstrated in level II or nondesignated centers (P = NS). NS, not significant.
Associated diagnosis and procedure codes
To further characterize the two cohorts, the top diagnoses (Table 3) and associated procedures were queried. Of note, the most commonly associated primary diagnoses for patients undergoing laparoscopy included injuries with open abdominal wounds and unspecified abdominal/gastrointestinal injuries. The most common diagnosis associated with laparotomy was injury to the small intestine. The top mechanism of injury for both cohorts was a motor vehicle accident, comprising approximately a quarter of all cases for each. The second most common mechanism for laparoscopy was a fall versus a firearm injury for the laparotomy cohort. Procedure codes associated with laparoscopy were mostly radiological in nature, including X-ray, computed tomography (CT), and ultrasound of the abdomen. Exploratory laparotomy was the only surgical procedure noted in the top 10 additional procedures. Summing all open operations made these collectively the second most commonly associated procedure next to CT of the abdomen.
Top Five Mechanisms of Injury and Associated International Classification of Disease, Ninth Revision, Clinical Modification Codes by Operative Approach (n = 4554)
MVT, motor vehicle trauma.
Conversion to laparotomy
A full list of additional abdominal procedure codes was then generated. The purpose of this was to determine whether some of the patients who initially underwent a laparoscopic procedure also underwent an open abdominal operation or “conversion.” For 252 encounters, only a diagnostic laparoscopy was performed. Patient encounters in which an open operation was also discovered were then summed to estimate a laparoscopy-to-laparotomy conversion rate. A total of 44 codes were deemed open operations, corresponding to a conversion rate of ∼12.4% (44/355). These included the following ICD-9-CM codes: 54.11—“exploratory laparotomy” (n = 28); 54.19—“other laparotomy” (n = 5); 52.96—“anastomosis of pancreas” (n = 3); 52.95—“other repair of pancreas” (n = 2); 45.62—“other partial resection of intestine” (n = 1); 47.09—“other appendectomy” (n = 1); 50.22—“partial hepatectomy” (n = 1); 51.79—“repair of other bile ducts” (n = 1); 52.09—“other pancreatotomy” (n = 1); 53.72—“other and open repair of diaphragmatic hernia, abdominal approach” (n = 1). A subset of ICD-9-CM procedure codes (n = 22) were either ambiguous or could be performed utilizing either laparoscopy or laparotomy but not specified (e.g., 46.71—“suture of laceration of duodenum”). Including these cases corresponds to a conversion rate of 18.6%. All 66 cases were manually reviewed (R.S.) to ensure that all procedures occurred at the same time, indicating a conversion and not a reoperation.
Discussion
This study represents the first nationwide analysis of the use of laparoscopy in pediatric abdominal trauma. Both hypothesized trends were demonstrated. First, those in whom a laparoscopic approach was chosen were generally less acutely injured, older, and, presumably, more hemodynamically stable. In concordance with prior studies, patients undergoing laparoscopy had lower ISS scores and higher GCS upon arrival to the ED compared with patients going directly to laparotomy. Mortality was <1%. These patients also were more likely to be directly admitted to the floor compared with those undergoing laparotomy, and had a longer time to operation and a shorter hospital LOS. The evidence is concordant for the use of laparoscopy in those less severely injured than those who needed laparotomy. Second, we confirmed an increase in the use of laparoscopy over the 5-year study period. University hospitals and ACS-verified level I pediatric trauma centers accounted for virtually all the increase in utilization. Meanwhile, conversion to laparotomy was infrequent, performed in ∼18.6% of patients. This is a conservative estimate that included patients with additional procedure codes that were not definitively performed laparoscopically but could have been.
These findings have several important implications. First, the observed trends demonstrate that management of abdominal trauma continues to evolve in an attempt to reduce harmful and potentially unnecessary interventions such as negative laparotomy. 14 This began with selective NOM, which has repeatedly demonstrated a low failure rate4,15,16 and, over time, has become the standard of care for blunt solid organ injury.2,17 Advances in imaging techniques and improved sensitivity of CT also aim to decrease the need for morbid interventions, 14 and laparoscopy holds the potential to continue this trend.
As a diagnostic adjunct, laparoscopy confers several advantages over radiographic techniques. CT remains standard practice in the algorithm for trauma patients with suspected intra-abdominal injury, 18 and has allowed for a successful implementation of NOM. 5 However, when CT is not definitive, it may lead to diagnostic uncertainty and a need for additional testing or intervention. Common scenarios include patients with solid organ injury with pain beyond expected, leading to concern for associated hollow organ injury; or free fluid discovered in the absence of a solid organ injury, raising concern for suspected intra-abdominal pathology. In the case of hollow viscus perforation, the CT false-negative rate can be as high as 50%.19,20 While the use of FAST is well established in adult trauma, its utility is debated in the pediatric population. Ultrasound often cannot determine location of injury or type of fluid present, and only about half of children with an intra-abdominal injury present with a positive FAST exam.21,22 Finally, while diagnostic peritoneal lavage may help determine fluid type, it has similar limitations and is essentially obsolete. 5 Laparoscopy offers the ability to eliminate uncertainty, visualize an injury, and repair if necessary. Of the 355 patients who underwent laparoscopy, a diagnostic laparoscopy as the sole procedure was performed on 252 (71.0%). This suggests that surgeons are using laparoscopy frequently for diagnostic purposes.
Our findings suggest that the use of laparoscopy in pediatric intra-abdominal trauma is both safe and increasing in prevalence. Only one death was recorded in the laparoscopic cohort, and the utilization rate almost doubled at university hospitals and level I pediatric trauma centers in just 5 years. While it is impossible to determine the precise reason for its increased use, single-institution studies have reported that cultural change, commitment to using this modality at their trauma centers, and team familiarity likely play a key role.5,23 The increasing number of surgical trainees who are exposed to trauma laparoscopy during residency may also be a factor. Early concern regarding the use of laparoscopy for abdominal trauma was due to reports of a high missed injuries rate 24 ; however, recent studies and standardization of trauma laparoscopy have brought this down to almost zero.23,25,26
An in-depth examination of the 355 patients who underwent laparoscopy suggests that pediatric surgeons are indeed using this approach as both a diagnostic and therapeutic modality. NTDB captures all recorded procedure codes for each patient encounter, and thus other abdominal operations that were performed during the hospital stay could be queried. This allowed for estimation of a conversion rate, as well as a clearer understanding of which specific laparoscopic procedures were performed. In addition to diagnostic laparoscopy, laparoscopic repair or removal of the stomach, small bowel, appendix, colon, gallbladder, liver, diaphragm, and fascial defects were all reported. This echoes prior studies that noted the variety of traumatic injuries amenable to a minimally invasive approach,3,25,27 specifically hollow viscus or diaphragmatic injury.14,28 Concordantly, laparoscopy has been reported to obviate the need for laparotomy in 56%–82% of patients.3,5,10,25 Thus, in the appropriate clinical setting, there appears to be little downside to laparoscopy with numerous potential benefits to the patient. Cost, suggested as one of the few disadvantages, seems to be mitigated by a decreased hospital LOS. 23
Conversion from laparoscopy to laparotomy was infrequent (18.6%). Most cases of conversion were coded as an exploratory laparotomy, but the more detailed procedure codes included operations on the pancreas, small bowel resections, partial hepatectomy, and bile duct repair. These likely represent operations that are more difficult to perform laparoscopically, especially in the emergent setting. Other procedures such as duodenal/mesenteric repair or foreign body removal were ambiguous, as it is impossible to determine that these were performed laparoscopically or via open approach. There were a total of 22 of these procedures, which were included as conversion procedures to produce the most conservative estimate. Other reported conversion rates in the literature vary from 18.4% 5 to 32%, 23 but may be limited by small sample sizes. In some cases, conversion is the expected and planned outcome of a positive laparoscopic examination and thus should not be considered a failure in many cases. Other surgeons comfortable with advanced laparoscopic interventions may also utilize laparoscopy in a therapeutic manner to repair identified injuries.
The major strength of this study was the ability to use the world's largest trauma repository to analyze an uncommon intervention. However, there are several important limitations. As is the case with any large database, there is always concern for misclassification bias. Prior studies have noted a concern for underreporting of complication data, though NTDB data quality has improved greatly over time. 29 The potential for misclassification is especially important for this analysis, since accurate coding of procedures is paramount to dichotomizing patients to laparoscopic and open cohorts. In estimating a conversion rate, it is unknown whether surgeons identified an injury or not, then proceeded to an open operation, that is, was a negative laparoscopy an indication for an open operation for some surgeons? Also, centers voluntarily participate in NTDB, and selection bias may be present as these hospitals do not necessarily represent a national sample. NTDB does not yet have a weighted national sample database for pediatric trauma. A national study such as this does not provide the rationale for the choice of laparoscopy. This insight would be of great benefit. In addition, dynamic physiologic data (i.e., vital signs) were not available for review. It is assumed, based on higher GCS and lower ISS scores, that the laparoscopic cohort was not only less injured but also likely more hemodynamically stable. Finally, 14 years was defined as the upper age limit. Though older adolescent patients may be treated at pediatric trauma centers, we sought to capture a truly “pediatric” population, which is in accordance with prior research. 30
Laparoscopy is proving to be a useful modality in the management of pediatric abdominal trauma. Utilization is increasing, and its role will likely expand as surgeons become more accustomed to its use as both a diagnostic and therapeutic adjunct in trauma care. Stable patients who present with a high degree of clinical uncertainty for intra-abdominal injury or with surgical pathology amenable to laparoscopic repair may benefit significantly from its use. Future research should further define its growing role in the management of pediatric abdominal trauma, and educational programs/resources should be developed for pediatric surgeons who wish to incorporate trauma laparoscopy into their clinical practice.
Footnotes
Disclosure Statement
The authors did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest relevant to this article to disclose.