
Abstract
Abstract
Objective:
To evaluate the experience and result of combined laparoscope and flexible ureteroscope (f-URS) pyelolithotomy in dealing with large-burden complex renal calculi in children <1 year old.
Methods:
Eleven patients (7 males and 4 females) <1 year old were retrospectively reviewed between December 2015 and May 2017, who had been diagnosed with renal calculi and received combined laparoscope and f-URS pyelolithotomy. The operations were carried out under general anesthesia. Patient' characteristics, presenting symptoms, operative times, and blood loss, stone-free rate, and postoperative complications were all collected retrospectively.
Results:
All 11 patients received combined laparoscope and f-URS pyelolithotomy. All operations went smoothly without conversion record and blood transfusion. Average time consumed was 109 minutes (55–187 minutes), and blood loss reported was 16 mL (10–25 mL). Average hospital stay after operation was 7 days (5–11 days). On mean follow-up of 6–12 months, no symptomatic urinary tract infections and urinary calculi were detected.
Conclusion:
Laparoscope combined f-URS pyelolithotomy is considered safe in the treatment of large-burden multiple renal calculi in infant patients with a high stone clearance rate. It has certain advantages in the treatment of renal calculi in infants <1 year old, and it could be an alternative treatment when other treatments fail or are unavailable.
Introduction
Urinary calculi are not uncommon in pediatric population but relatively rare in infants <1 year old. With the development of technology, urinary calculi in older children and adults can be treated by endoscopic or extracorporeal shock-wave therapy avoiding open surgery. For pediatric renal calculi, extracorporeal shock-wave lithotripsy (ESWL) is the first-line therapy. But for large-burden complex stones, ESWL would not work every time, and for infantile patients a series of general anesthesia would be needed accordingly. Endourological treatment, which is widely used in adults, is difficult to use in infant cases because of the special conditions such as small diameter of ureter in infants. Therefore, treating infant urinary calculus has been a more difficult problem. Most infants with urinary calculi, especially large-burden multiple stones, eventually have to be treated by open surgery. This not only brings more harm to patients but also prolongs the length of hospitalization and aggravates the financial burden of patients. We use laparoscope combined flexible ureteroscope (f-URS) for treating large-burden multiple renal calculi of infants, and good results have been achieved.
Patients and Methods
Clinical data
From December 2015 to May 2017, 11 infants with multiple renal calculi, including one on both sides, were reviewed. There were 7 males and 4 females. Monthly age ranged from 4 to 11 months, with an average of 7.5 months. The first onset symptom in 8 patients was unknown fever, and urinary tract infection (UTI) was then confirmed. Hematuria was found in the other 3 patients.
We assessed several variables, including stone burden (stone burden was assessed on preoperative imaging using the cumulative stone diameter method) and location, operation times, changes in glomerular filtration rate (GFR) after surgery, hospital stay time, success rate, and complication rate. Each patient was tested for urine culture, and patients with positive cultures underwent treatment with antibiotics for 2 weeks. Ultrasonography and diethylene triamine pentaacetic acid (DTPA) scans were performed for preoperative evaluation. Plain kidneys, ureter, and bladder (KUB) film and ultrasonography were used to evaluate patients at the fourth week after operation. Stone-free rate was defined as the absence of residual fragments >4 mm. All stones were collected for composition analysis. Double J stent was removed under cystoscope 1 month after operation. We followed patients during the next 3 months for potential delayed complications.
Operative methods
General anesthesia with endotracheal intubation. Retrograde insertion of the 3F double J stent into the ureter was performed by cystoscopy first in lithotomy position. After the insertion of double J stent, the patients were then positioned in the lateral flank position with 45° inclination and close to the edge of operating table. Access is first obtained by the Hasson technique through an infraumbilical incision. After placement of a 10-mm trocar, the abdomen is insufflated with CO2 and maintained at a pressure of 8–10 mmHg. The other two 5-mm trocars were placed under direct vision: one at the level midway between the xiphoid and umbilicus, and the other in the lower quadrant. Standard 5-mm instruments were used in the operation. For left side, transmesocolic approach was performed, and the paracolic sulci approach was performed for right side. Gerota's fascia was identified and incised. After the ureter, renal pelvis and ureteropelvic junction are exposed, a transabdominal holding suture (3-0 suture on a straight needle) was placed by passing the needle through the anterior abdominal wall, through the renal pelvis and back out through the anterior abdominal wall. The extracorporeal holding suture serves to stabilize the renal pelvis during manipulation and suturing. The pelvis was opened along the long axis of the kidney. The stone in pelvis was removed first (Fig. 1), and the f-URS was inserted from the trocar of the laparoscope into the pelvis through the pelvic incision, examining the pelvis, upper, middle, and lower pole of the kidney in turn. After the stones were found (Fig. 2), stones were fragmented using a holmium laser and then removed by the stone basket (Fig. 3). The pelvis was rinsed after stone removal, and checked for any residual fragment, and then the pelvic incision was sutured. After the aspirator sucked the intraperitoneal effusion, a drainage tube is placed in the inferior pole of the kidney at the operative side.

After opening the pelvis, the stone in the pelvis was removed first.
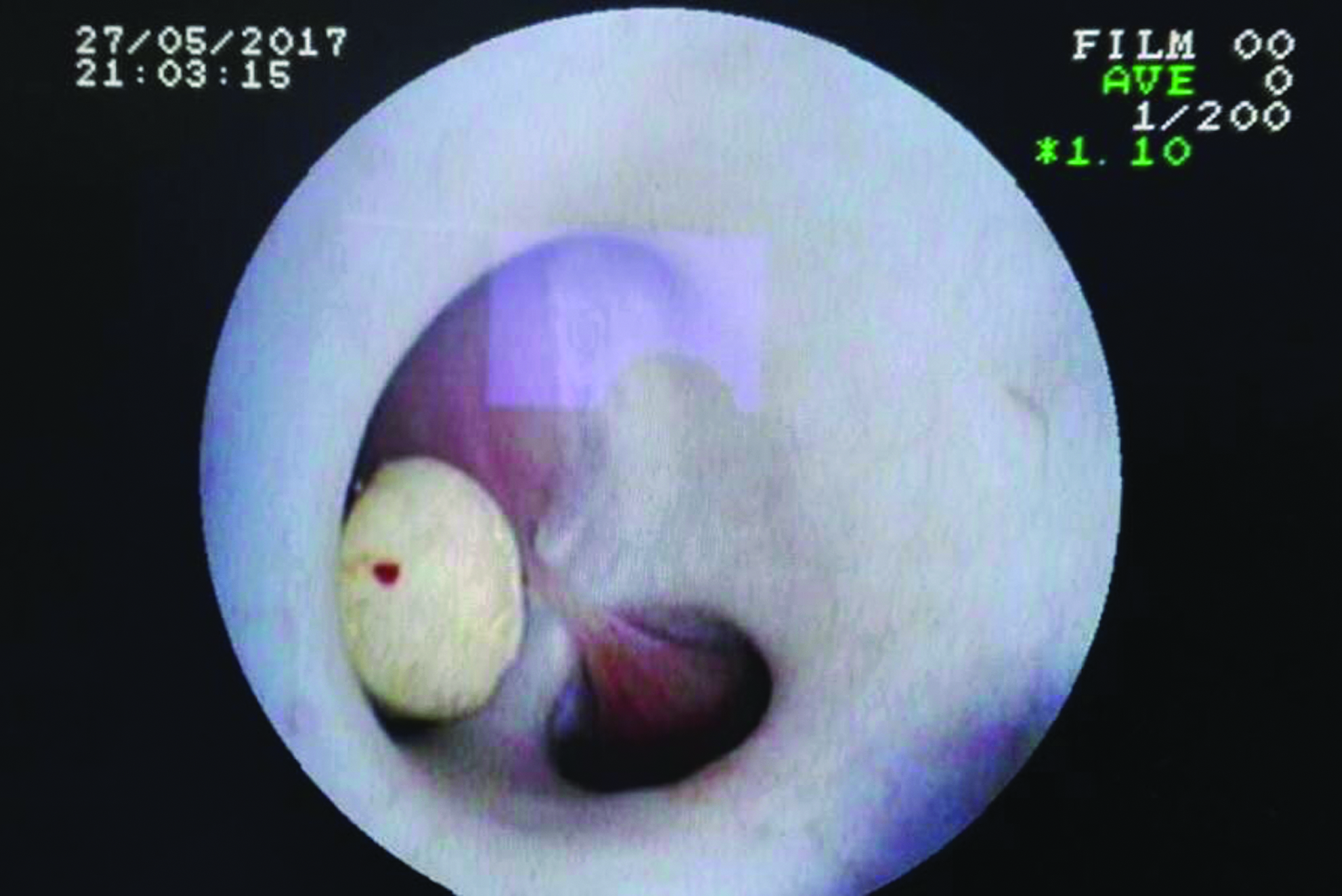
A stone in renal calyx found by flexible ureteroscope.

Parts of stones removed by flexible ureteroscope.
Results
There were 10 cases of pelvic calculi with multiple calyceal calculi and 1 case of bilateral pelvic calculi. The stone size ranged from 0.7 × 1.1 cm to 1.2 × 2.5 cm. The calculated stone burden ranged from 2.5 to 4.6 cm (average 3.2 cm). There were 10 cases with mild hydronephrosis. All cases have no evidence of hydronephrosis (including prenatal ultrasonography) before the onset of calculi. Radionuclide scans showed an obstructive curve. There were 7 cases with no obvious impairment of renal function on the affected side, 3 cases with <40% and >30%, and no cases with <30%. The left and right renal functions of one case with double kidney stones were 46% and 54%, respectively.
All patients were followed up from 6 to 12 months after operation. All 11 operations were successfully completed, and no cases of conversion to open surgery or blood transfusion were found. The average operation time was 112 (55–187) minutes, and the intraoperative bleeding volume was 15 (10–25) mL. The average total drainage flow was 16 (5–38) mL, and the average hospital stay was 7 (5–11) days. There were no patients with server fever after operation. No perirenal cyst formation was observed after operation. No residual stones were found after operation, and the stone clearance rate was 100%. There were no cases of renal atrophy. No recurrent UTIs occurred after removal of double J stent, and hydronephrosis cases were significantly reduced. Stone composition analysis showed that most of them were mixed stones, including calcium oxalate in 5 cases, calcium phosphate in 2 cases, xanthine in 2 cases, and magnesium ammonium phosphate in 2 cases (Table 1). During the follow-up period, there was no recurrence of stones.
Patient Characteristics
Discussion
Urinary calculi are one of the most common diseases in urology. Urinary calculi are common in adults, and the number of infant calculi patients is significantly lower than that of adults, but there are obvious regional and environmental differences. Literature reports show that infant calculi in the population ranged from <3% to as high as 30%.1–3 Studies have reported that the peak incidence in children is 6–8 years old, and very few infants <1 year old suffer from calculi. 4 However, after the incident of melamine-contaminated milk powder, the number of urinary calculi in infants in China increased in a short period of time. In addition, 11 cases of infant calculi were reported from the Kangba area of China. There was no exposure to melamine-contaminated milk powder in the feeding history of children in this group, but there were some cases of substitution or partial substitution of breast-feeding by goat's milk or yak's milk or even bamboo cake.
The etiology of urinary calculi is complex. Kidney stones are crystalline mineral deposits formed in the kidney. The formation of kidney stones is related to urine volume, urinary calcium, and other electrolyte concentrations, and urinary citrate and magnesium, which are the inhibitors of stones.5,6 It is also related to urinary infection, urinary pH value, and malformations. Although there are many similarities with adult urinary calculi, the causes of pediatric urinary calculi also have their own features. 1 Metabolic abnormalities, congenital malformations, and infections account for a large proportion of the causes of urinary calculi in children. 7
In most times, conservative treatment is performed for small stones without obstruction, symptoms, and functional impairment in infant patients. Some studies have reported that the self-discharge rate of stones is related to the transverse diameter of stones: the self-discharge rate of stones with transverse diameter <5 mm can reach 98%, whereas the self-discharge rate of stones with transverse diameter >6 mm is only 15%, and those with transverse diameter >8 mm can hardly self-discharge.8,9 In terms of intervention methods, adults can promote stone excretion through physical exercise, dietary adjustment, drug treatment, and other methods. However, infants have a simple diet and limited locomotion. Therefore, for infant urinary calculi intervention methods appear to be limited. It is particularly important to find the cause of infant calculi. We suggest that children under the age of 1 should be routinely screened for metabolic abnormalities and structural abnormalities of the urinary system, and those who are in a position to do so may undergo relevant genetic screen.
Sarica et al. 6 demonstrated higher frequency of UTI, and stone attacks affected the growth status of the infants in a remarkable manner than the other cases. Urinary calculi with symptoms and impairment of renal function need early clinical intervention. At present, the surgical treatment of adult urinary calculi has been quite diversifying. Specifically, there are many ways to deal with different locations and sizes of kidney stones, such as ESWL, ureteroscope and f-URS lithotripsy, percutaneous nephrolithotripsy (PCNL), laparoscopy, and open surgery lithotripsy. Moreover, with the advance of technology, open surgery and other traumatic treatment methods have retreated to the second line. In principle, the same treatment modalities are used for adults and children. However, the specific circumstances of pediatric therapy must be taken into account when treating infant patients.
For more frequent spontaneous passage of stones in children, it has traditionally led pediatric surgeons to recommend ESWL over other treatments. 8 The subcutaneous tissue of children is weak and extracorporeal shock wave is not easy to attenuate; ESWL has achieved good results in pediatric patients. However, less-efficient ESWL disintegration might be seen in children with stones composed of cystine, brushite, and calcium oxalate monohydrate. ESWL has little side effect on the long-term renal function of children, whereas the decrease of GFR cannot be ignored. 10 Ureteroscopy and flexible endoscopy are effective treatment alternatives for stone removal in children. 11 However, as the ureteral diameter in infants is relatively small, it is difficult to perform ureteroscopy or flexible endoscopy; even if it can be performed, a double J stent is always needed to be placed preoperatively. For infantile patients, the risk of ureteral injuring is high, and more anesthesia is needed. The efficacy and safety of PCNL have already been proven in adults. 12 Due to the potential risks, such as bleeding, major complications associated with sepsis, the fear of exposure to radiation, and parenchymal injury from the fluoroscopy, urologists were reluctant to use adult instruments in the management of pediatric patients with kidney stones. Some scholars claim that percutaneous nephroscopy is not restricted in pediatric patients; however, complications such as high postoperative fever and bleeding requiring blood transfusion were reported.13–16 The all-seeing needle technique or micro-PERC has recently gained popularity in endourological practice. 17 The micro-PERC technique is considered to have advantages, such as prevention of bleeding and organ injury and other potential complications. 17 However, the absence of an appropriate tract diameter and equipment for the extraction of fragmented stones make it limited in dealing with large stone burden cases. 18 As stone burden be mentioned, almost all the available less invasive methods were limited while dealing with large-burden stones in infant patients.19,20 In pediatric patient populations, combined use of two or more methods is always needed in dealing with large-burden stones. 21
In this group of cases, the surgical method used is pyelolithotomy, which does not damage the renal parenchyma and can avoid the loss of nephron unit caused by puncture scar during PCNL. The operation involves opening the renal pelvis, which is at risk of injuring the renal vessels. Therefore, in the implementation of this operation, all operations need to be carefully performed under direct supervision. Laparoscopic combined f-URS can remove stones completely most of the time, as the stone clearance rate is relatively high, and it is not limited to the special location just like the lower calyx, and can be treated for the possible coexistent ureteral stone at the same time. For staghorn calculi or other huge stones, it is difficult to remove them through the pelvis. Holmium laser can be used to fragment them. Because the pelvic incision is larger than endoscopic channels such as nephroscope and ureteroscope, the stone does not need to be powdered when lithotripsy and larger fragments can be removed directly. It would decrease time consumption significantly. In addition, this method can simultaneously deal with possible malformations such as ureteropelvic junction obstruction.
For a laparoscopic operation of the kidney, the trocar arrangement of this method is almost the same as that of the transperitoneal approach laparoscopic pyeloplasty. However, considering the potential need to remove larger fragments of stones we recommend that at least one 10-mm access be arranged. Either 3 or 5 mm of the other two trocars would be acceptable. However, for multiple calculi, it is more convenient for flexible endoscopy to enter the pelvis from the upper abdomen 5-mm trocar in the treatment of lower calyx calculi. For obstructive calculi, especially those complicated with preoperative infection, the pelvis and renal adipose capsule often adhere obviously, resulting in bleeding easily during the process of separation and tissue tearing easily in the process of suture. Accuracy and a gentle touch during the operation would be helpful in controlling postoperative complications. Although there is no healing problem in this group of cases, the incision leakage after calculi surgery is not uncommon. We recommend to place a perirenal drainage tube as a routine procedure for beginners.
Compared with other methods, laparoscopic combined f-URS has some limits. It is a much more invasive method most of the time. This method is performed transperitoneally; as it requires incision of the renal pelvis, there is a risk of abdominal infection. In addition, in cases without hydronephrosis, it is relatively difficult to expose the renal pelvis. The small sample size and retrospective nature of our study are the limitations. Additional randomized controlled studies with a larger series are needed.
In conclusion, the selection of the most appropriate treatment has to be based on the individual stone problem, the available equipment, and the urologist's expertise in treating children. Laparoscope combined f-URS pyelolithotomy is safe in the treatment of large-burden multiple renal calculi in infant patients with a high stone clearance rate. It has certain advantages in the treatment of renal calculi in infants <1 year old, and it could be an alternative treatment when other treatments fail or are unavailable.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.